
記住我








A 12-year-old male with unremarkable past medical history initially presented to his pediatrician for lower extremity edema. He was hypertensive into the 140 s/100 s on repeated blood pressure measurements. He was discharged from clinic with a plan for salt restriction, follow-up blood pressure check, and weight loss. One month later, he presented to the emergency department for progressive worsening of his edema associated with intensifying headaches and one week of dry cough.
His exam was notable for pitting edema up to the knee and ascites. Vitals revealed increased weight (+ 12 kg) and hypertension. Labs revealed urine protein to creatinine and albumin to creatinine ratios that were immeasurably high (urine protein > 600 mg/dL, albumin > 440 mg/dL, and hematuria (133 RBCs/HPF)). Creatinine at presentation was 1.17 mg/dL (eGFR 56 ml/min/1.73m2). There was low C3 (9 mg/dL), borderline-low C4 (15 mg/dL), and low CH50 < 12.5U/mL. He had mild hyperkalemia and hypoalbuminemia of 2.2 mg/dL. Immunological workup was negative for the following autoantibodies: ANA, centromere B, dsDNA, Smith, SS-A, SS-B, Scl70, ANCA, and GBM. He had mildly elevated DNase B of 330U/mL with normal anti-ASO titers. Infectious studies were negative, including hepatitis A, B, and C serologies and HIV screen. ESR, CRP, LDH, and haptoglobin were within normal limits.
Initial management focused on achieving euvolemia with fluid restriction, low sodium diet, and diuresis using 25% albumin and furosemide. He was given IV methylprednisolone 1 g × 3 days, followed by prednisone 60 mg with a 6-month taper. A diagnostic kidney biopsy was performed after hospital discharge. Light microscopy demonstrated glomerulonephritis with a membranoproliferative pattern. Immunofluorescence (IF) staining of the mesangium and capillary loops was IgG3/Kappa dominant. The intensity of staining on a scale of 0 to 4 + was as follows: 3 + for IgG, 1 + for IgM, and 3 + for C3. All IgG was of the IgG3 subclass, and IF staining was negative for IgA, lambda light chains, and C1q. Electron microscopy showed numerous large mesangial and subendothelial immune complex deposits as well as rare small subepithelial deposits. Podocytes were diffusely effaced, and there was prominent remodeling of the glomerular basement membrane, with frequent areas of duplication. He was subsequently started on ACE inhibition for blood pressure and proteinuric control.
Given the concern for MGRS—specifically, PGNMID—from the biopsy findings, the following labs were sent: cryoglobulin, urine and serum immunofixation studies, C3 nephritic factor (C3NeF; hemolysis-based, C3 convertase stabilization assay), complement factor H, anti-CFH, circulating immune complex (including anti-C3b), and Machaon gene panel for C3 glomerulopathy. These were positive for C3NeF only; the genetic panel was negative for CFB, CFH, CFI, MCP, C3, and CFHR5 mutations. He was initiated on immunosuppressive treatment with mycophenolate mofetil (MMF) 6 weeks after his ED presentation. Despite 6 weeks of MMF and continued ACE inhibition, he had persistent hypocomplementemia, nephrotic-range proteinuria, and elevated creatinine. Pediatric hematology/oncology was consulted for further investigation of his monoclonal gammopathy, and hematologic malignancy such as underlying lymphoma or multiple myeloma was ruled out with a normal PET scan and bilateral bone marrow aspirates and biopsies. In discussion at adult nephrology/oncology tumor board, daratumumab was recommended over rituximab due to its efficacy in clonal population targeting in adult patients with PGNMID even though there was no clone identified in this patient. Additionally, the discussion reviewed the favorable safety profile and tolerability based on experience in pediatric patients with T-cell acute lymphoblastic leukemia.
Our patient began daratumumab 16 mg/kg infusions 4 months after presentation. His regimen consisted of 8 weekly infusions, followed by 8 infusions every other week and now an ongoing monthly maintenance dose. His response to daratumumab was impressive; by 1 month after the first infusion, his UPCR fell to below nephrotic-range for the first time, and his serum albumin and complement levels normalized. His C3NeF also normalized. Improvement in creatinine and cystatin C occurred more slowly, with a consistent downtrend after 6 months of therapy (creatinine 0.81 mg/dL and cystatin C 1.3 mg/L, eGFR 76 mL/min/1.73 m2). These continue to improve at the time of this manuscript. Changes in disease-relevant laboratory indicators as a function of time and medication changes are demonstrated in Fig. 1. The patient has had no side effects from daratumumab, though his T, B, and NK cells are quantitatively low and he has received a single dose of intravenous immunoglobulin (IVIG) for hypogammaglobulinemia. Due to his quantitative immune defect, he was empirically initiated on fungal and Pneumocystis jirovecii prophylaxis though his lymphocyte antigen and mitogen proliferation studies are currently normal indicating no qualitative immune deficit.
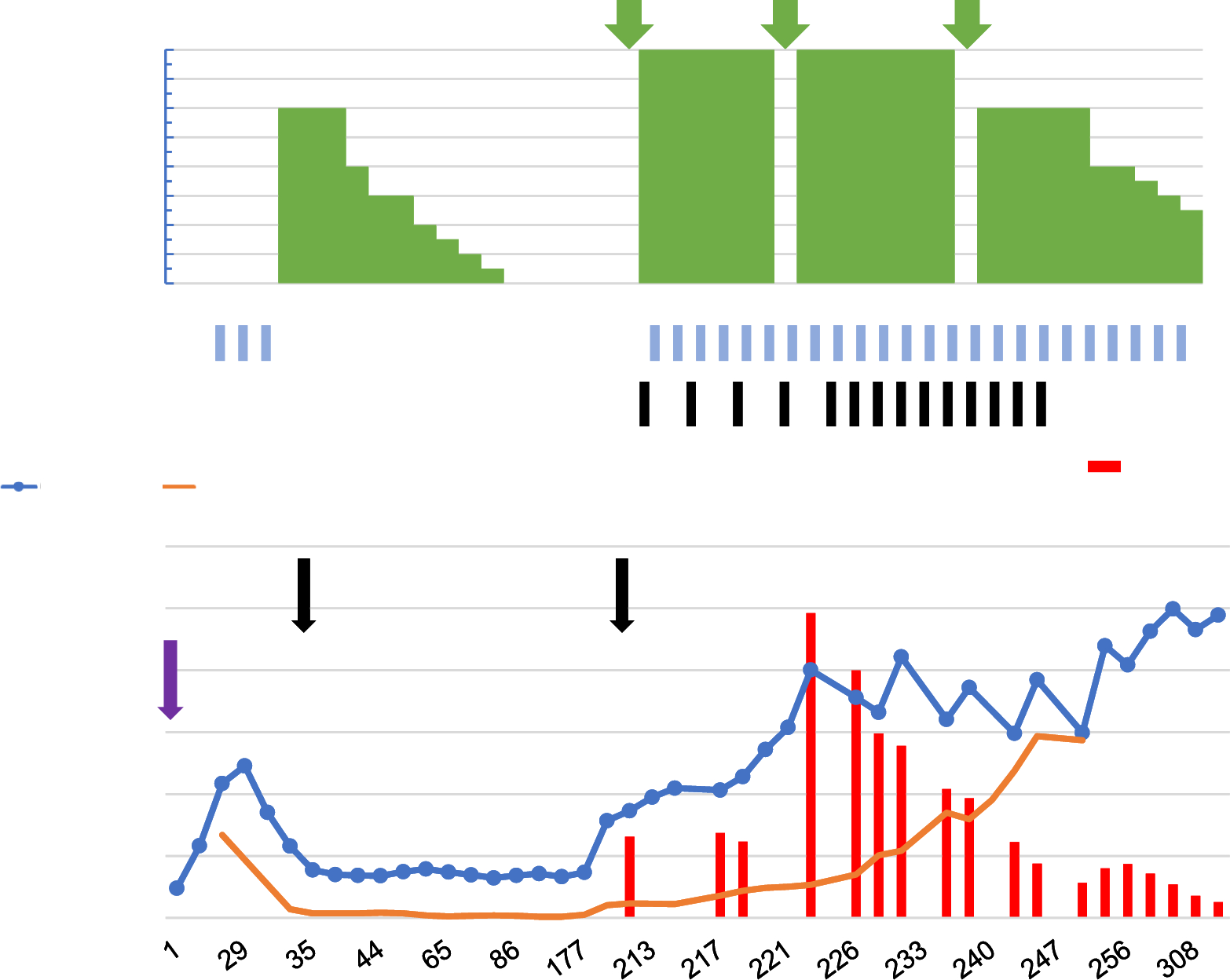
Fig. 1
Response of various serological markers of disease activity to immunosuppressive therapies over time
留言 (0)