
記住我





The present study was approved by the Clinical Trial Ethics Committee of Beijing Tongren Hospital (TREC2022-KY091). Informed consents were obtained from all patients recruited during the preoperative period. The trial was registered prior to patient enrollment at the Chinese Clinical Trial Registry (ChiCTR2200066583, https://www.chictr.org.cn/showprojEN.html?proj=178475, Principal investigator: Yin Bao, Date of registration: 09/12/2022). This manuscript adheres to the applicable STROBE guidelines.
PatientsTwenty male hypopharyngeal carcinoma or larynx carcinoma patients underwent total laryngectomy and 40 patients (20 male and 20 female) with nodules or polyps at the vocal cord underwent selective micro-direct laryngoscopic resection between December 10, 2022, and April 10, 2023 at the Beijing Tongren Hospital in Beijing, P. R. China.
Inclusion criteria: ①ASA I ~ III level; ②Age between 50 and 75-years-old; ③BMI: 22 ~ 28 kg/m2; ④Patients undergoing elective total laryngectomy or micro-direct laryngoscopic surgery.
Exclusion criteria: ①History of head and neck surgery; ②Head and neck chemoradiotherapy affect laryngeal structures; ③Laryngeal cancer invading important laryngeal structures which could affect data measuring; ④Intraoperative damage to important laryngeal structures; ⑤Patients who were severely obese or had the abnormal anatomical structure of the neck.
Data collection and analysisSpecimen preparation and measurementFresh larynx specimens were obtained from 20 male hypopharyngeal carcinoma or larynx carcinoma patients from December 10, 2022, to April 10, 2023. Each side of the specimen was regarded as a separate object. All the objects were randomized into 4 groups (n = 10 in each group). Simulated SLN blocks were manipulated by injection of 2-, 3-, 4-, and 5- mL 2% lidocaine mixed with 0.01% methylene blue dye using a 22-gauge 50 mm blunt-tip peripheral nerve block needle (UniPlex NanoLine, PAJUNK®, Canada). The iSLN block injection technique was used on the specimen under direct visual observation. (as shown in Supplementary Fig. 1).
At 30 min after dye injection, macroscopic anatomical dissection was performed to expose the thyrohyoid membrane. Superficial areas of the deposited lidocaine/methylene blue mixture were measured. The occurrences of methylene blue dye overflowing from the puncture site at the thyrohyoid membrane (MOPT), penetrating the anterior epiglottis space, and staining the anterior epiglottis space, the hyoid, and the thyroid cartilage were recorded. Distances between the iSLN and hyoid (D1), thyroid cartilage (D2), and the anterior midline of the neck (D3) were measured (As shown in Fig. 1D).
Fig. 1
Schematic diagram illustrating anatomy and ultrasound localizations
A Diagram of ultrasonic probe location; B Schematic diagram illustrating anatomy and ultrasound localizations Measurement of SLN puncture site to surrounding structures under ultrasound; C Schematic diagram illustrating anatomy and ultrasound localizations Dissection of the right side of the larynx; D Measurement of SLN puncture site to surrounding structures on the fresh larynx specimens; E Photograph of the lidocaine/methylene blue mixture deposited after SLN blocking. iSLN, internal branch of the superior laryngeal nerve; THM, thyrohyoid membrane; Hy, hyoid bone, greater horn; Thyr, thyroid cartilage; SLA, superior laryngeal artery; uD1, distance between the iSLN and hyoid; uD2, distance between the iSLN and thyroid cartilage; D3, distance between the iSLN and anterior midline of the neck; uD4, the vertical distance from the skin surface
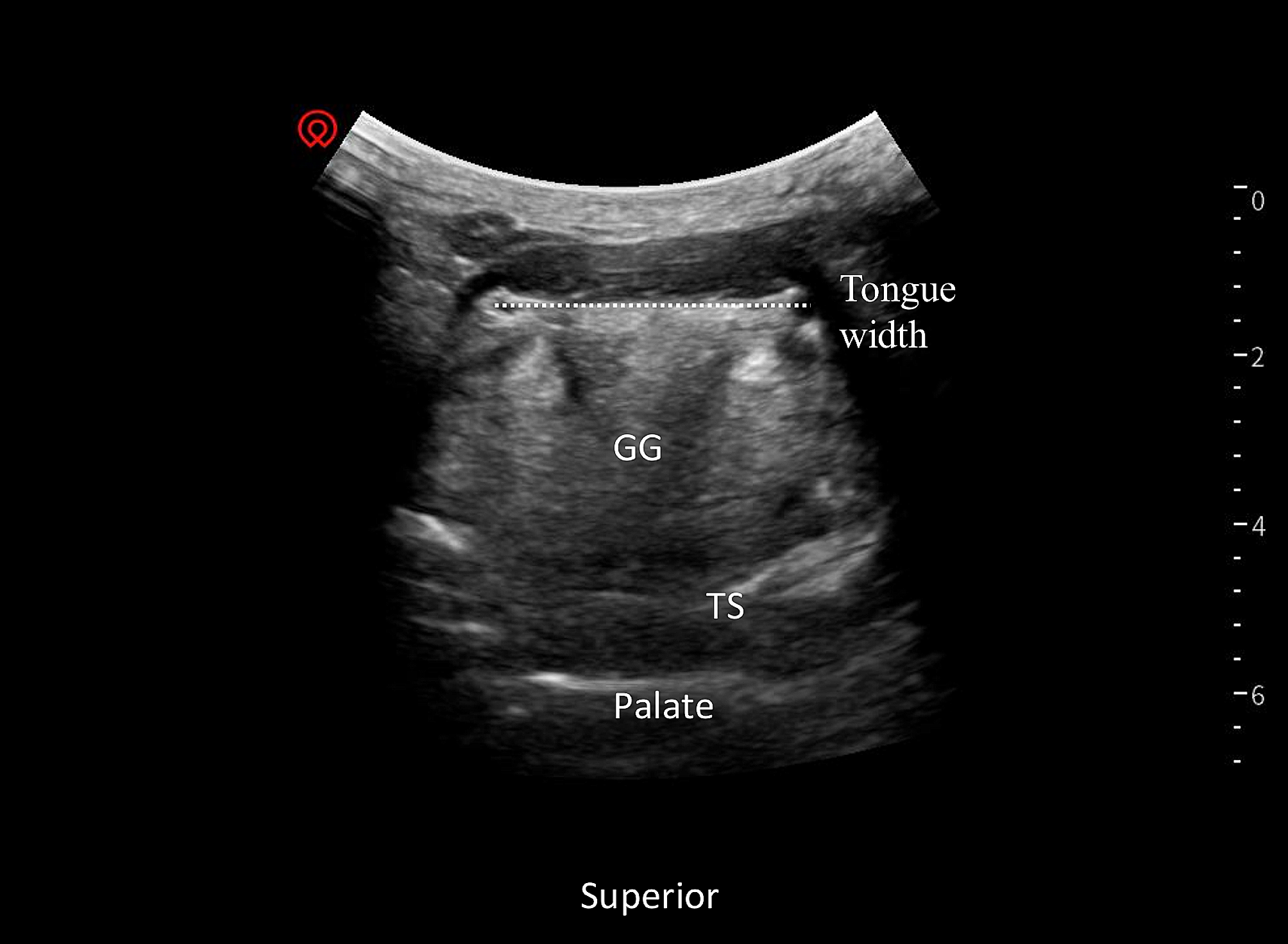
Ultrasound-guided noninvasive measurementsTwenty male and twenty female patients with nodules or polyps at the vocal cord from December 10, 2022, to April 10, 2023, were prospectively included in our noninvasive ultrasound measurement investigation. A 6–15 MHz high-frequency linear array probe was placed over the neck area in the supine position (As shown in Fig. 1A). Sonographically, the iSLN was established lateral to the superior laryngeal artery and crossed the surface of the thyrohyoid membrane. Lengths between the location of iSLN and hyoid (uD1), thyroid cartilage (uD2), and the anterior midline of the neck (uD3), and the vertical distances from the skin surface (uD4) were measured under ultrasound scanning (Fig. 1B).
Statistical analysis Determining the sample sizeTo perform a hypothesis test for this study, it was assumed that there were significant differences in the rate of MOPT among the groups. According to our pilot tests, the incidence of thyrohyoid membrane dyeing among all the dye-injected fresh specimens in the 2-, 3-, 4-, and 5- mL injection groups were 18%, 47%, 66%, and 100%, respectively. If α = 0.05 and β = 0.2 for 2-tailed testing, the sample size was calculated using the following formula: The minimal sample size for each group was 8. For a constant 20% failure rate of errors, we finally increased the sample size by 10 per group, for a total of 40.
Statistical testsOne-way repeated-measures ANOVA was used to compare the vertical and horizontal diameters of blue dye-stained areas on the thyrohyoid membrane among groups. Fisher’s exact test was used to compare the occurrences of MOPT, the permeated anterior epiglottis space, and the dyed anterior epiglottis space, hyoid, and thyroid cartilage. Distances between the iSLN and hyoid (D1/uD1), thyroid cartilage (D2/uD2), and the anterior midline of the neck (D3/uD3), and vertical distances from the skin surface (uD4) were assessed for normality by the Kolmogorov–Smirnov (K-S) test, and descriptive statistics were calculated using GraphPad Prism software (version 9.2.0; GraphPad Software Inc., San Diego, California, USA). Statistical significance was defined as a P value of less than 0.05.
留言 (0)