Women of South Asian background are known to have higher rates of stillbirth than women in other high-income countries, such as Australia or the United Kingdom. To reduce the rate of stillbirth, leading societies recommend antenatal fetal monitoring or induction of labor (IOL) at 41 weeks of gestation regardless of race/ethnicity. However, at 41 weeks' gestation, the risk of stillbirth for South Asian–born women is already up to 5 times higher than for Australian-born women. Initially, the UK National Institution for Health and Care Excellence recommended that all South Asian women undergo IOL earlier, at 39 weeks of gestation. However, this recommendation was criticized as being racist, and perpetuating the myth that race plays a factor in poor outcomes, so it was amended to state that South Asian–born women might benefit from additional monitoring and support. Still, there is no evidence to support this guidance. In July 2017, the State of Victoria in Australia implemented a new clinical guideline to provide South Asian women with biweekly cardiotocography and amniotic fluid measurement at 39 weeks of gestation. The aim of this study was to assess the impact of the new clinical guideline on the rates of stillbirth and select pregnancy outcomes for South Asian women.
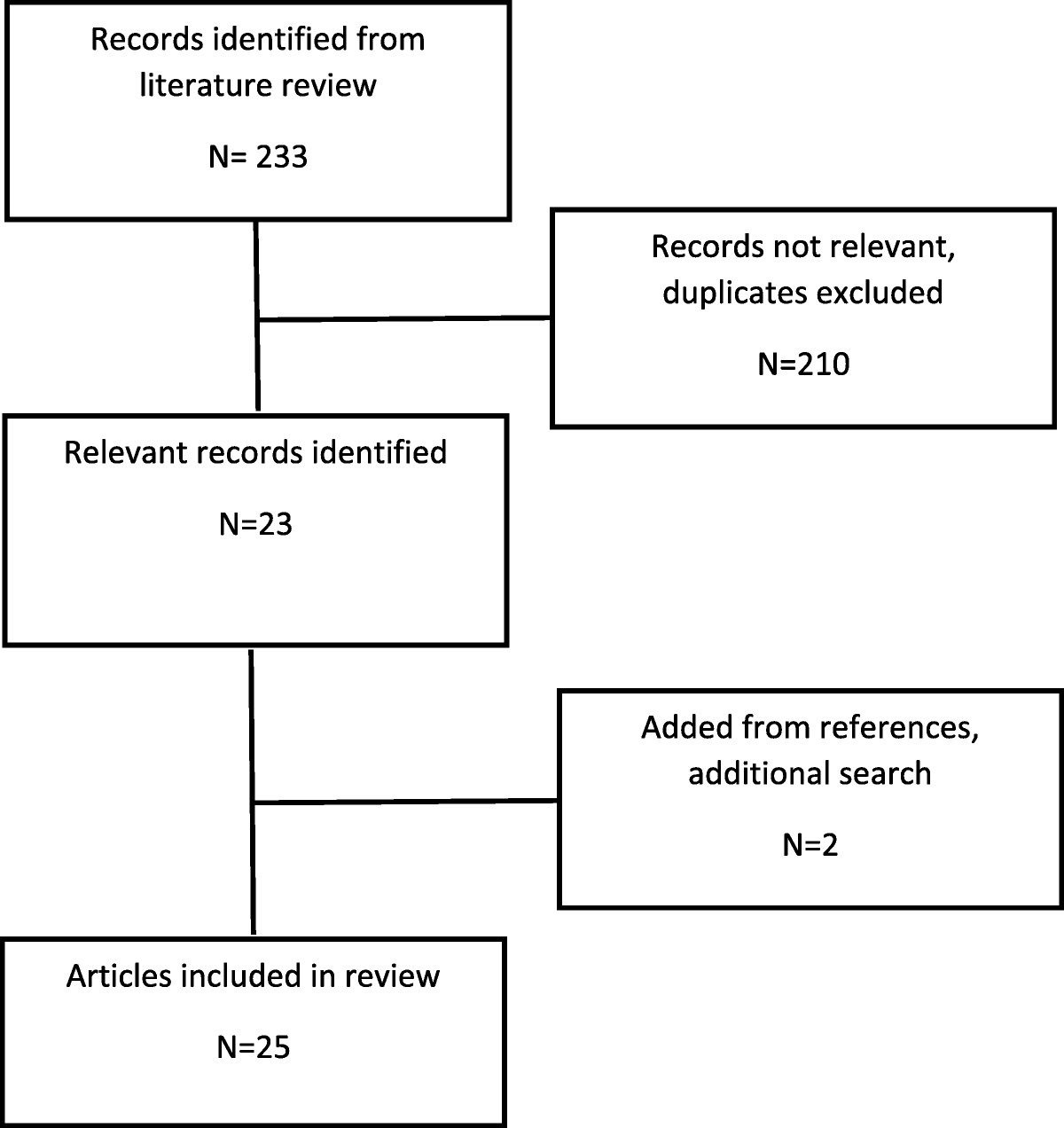
This was a cohort study that included women with singleton pregnancies who gave birth at term or beyond at a university- affiliated teaching health service located in 3 metropolitan areas in Australia from January 1, 2016, to December 31, 2020. Women were classified as South Asian born if they self-identified as being from Afghanistan, Bangladesh, Bhutan, India, Iran, the Maldives, Nepal, Pakistan, or Sri Lanka. The timeframe between January 1, 2016, and June 30, 2017, represented the period before the change in practice for fetal monitoring for South Asian women; the timeframe between July 1, 2017, and December 31, 2020, represented the period after. Although the new practice was applied to South Asian–born women in the second timeframe, fetal monitoring at 41 weeks was applied to all other women. The primary outcome was stillbirth at the onset of or during labor at 37 weeks and 39 weeks of gestation. The secondary outcomes included neonatal death at <7 days, admission to the special care nursery or neonatal intensive care, Apgar score <7 at 5 minutes, infant birthweight, gestation of birth, IOL, and mode of birth.
A total of 3506 South Asian women gave birth before the change in practice, whereas 8532 gave birth postimplementation. The rate of stillbirth at 37 weeks' gestation for South Asian–born women was 2.3 per 1000 births—a 2.6-fold higher rate than for other women (0.9 per 1000 births; P = 0.06). After the change in practice, the rate of stillbirth fell by 64% for South Asian–born women (95% confidence interval, 87%–2%; P = 0.047). The association was stronger when the results were restricted to births after 39 weeks of gestation. Also, after the change in practice, reduced rates for early neonatal death (3.1 per 1000 vs 1.3 per 1000; P = 0.03) and admission to the special care nursery (16.5% vs 11.1%; P < 0.001) were observed. The median gestation of birth for South Asian–born women was 39+3 weeks preimplementation compared with 39+2 weeks postimplementation, a difference of 1 day. The rate of IOL for South Asian–born women was 4.9% higher than other women (95% confidence interval, 1.3%–8.5%; P = 0.008). However, no significant difference was observed between the 2 groups in the rate of IOL per month after the change in practice, nor across the other secondary outcomes.
In conclusion, fetal monitoring starting at 39 weeks' gestation among South Asian–born women reduced the rate of stillbirth, neonatal death, and admission to the special care nursery compared with previous guidelines to begin monitoring at 41 weeks.




留言 (0)