In the United States, around 9 million women are affected by pelvic pain due to conditions such as interstitial cystitis/bladder syndrome, fibromyalgia, pelvic floor myalgias, chronic opioid use, or irritable bowel syndrome. Treatment options for concurrent pelvic floor disorders and pelvic pain can prove challenging due to the overall desire to avoid exacerbating overall pain while optimizing pelvic floor symptoms. The primary aim of this study was to compare both perioperative pelvic muscle training and vaginal reconstructive surgery among women who experienced or lacked preoperative pain and to inform better approaches to management of women with preoperative pain.
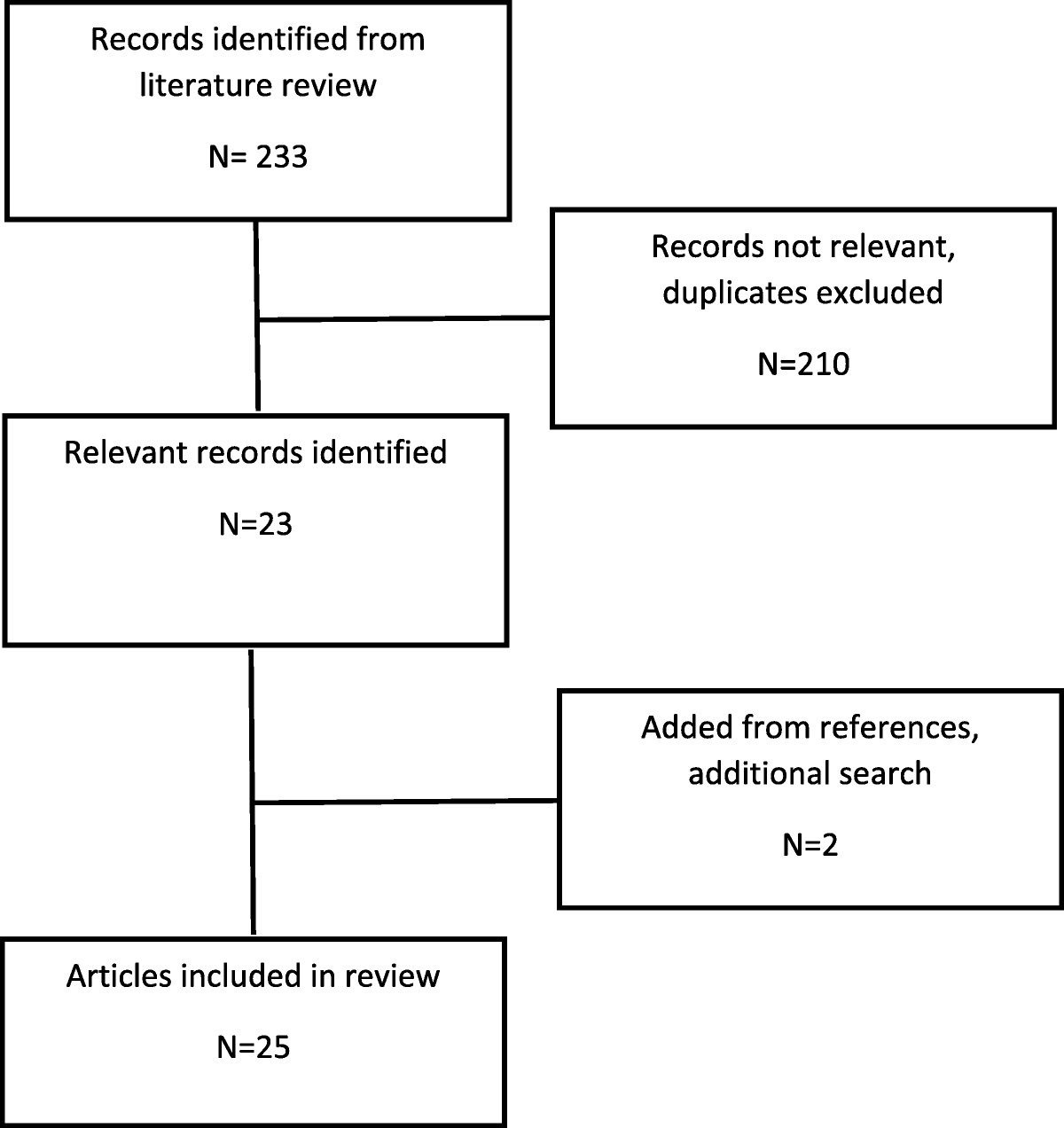
The study was a secondary analysis of the Operations and Pelvic Muscle Training in the Management of Apical Support Loss (OPTIMAL) randomized clinical trial, as performed via the Pelvic Floor Disorders network. The main study's design was a 2 × 2 randomized factorial design with a surgical intervention and a perioperative behavioral intervention. The Eunice Kennedy Shriver National Institute of Child Health and Development data and specimen hub provided the data for this study. Included were 374 women undergoing surgery for both stress urinary incontinence and stage 2–4 pelvic organ prolapse from 2008 to 2013. All participants underwent vaginal prolapse repair and midurethral sling, and were randomized to either perioperative pelvic muscle therapy or usual care. The Pain scale, the Pelvic Floor Impact Questionnaire, the Pelvic Floor Distress Inventory, and the Patient Global Impression of Improvement were all completed by patients at baseline and repeated through month 24. The OPTIMAL trial had a primary outcome of surgical success as defined by anatomical success, but the primary outcome of this secondary analysis was a change in pain scale scores over 24 months after surgery.
Three hundred seventy-four women participated in the original trial, with 368 in this secondary analysis. One hundred nine of the 368 women reported preoperative pain. Women with pelvic pain were more likely to be Hispanic, but there were no differences in surgical procedures performed, hospital stay, complications (ie, bladder injury, suture exposure, etc), or estimated blood loss in women with and without pelvic pain. Women with preoperative pain experienced greater pain at all time points, but also exhibited greater pain improvement at 24 months after surgery. Women with preoperative pain had worse baseline pelvic floor symptoms than those without pain. Although women with pain and women without pain had improvements in distress symptoms measured with the Pelvic Floor Distress Inventory, women with pain saw a greater improvement after surgery. All distress subscales improved significantly more in women with pain than women without pain. One additional interesting finding was that women randomized to sacrospinous suspension and pelvic muscle therapy had greater improvements in postoperative pain than those randomized to usual care. Notably, rates of surgical anatomic success and extent of Patient Global Impression of Improvement were not different between women with and without pain.
Strengths of the study include its design as a secondary analysis of a large prospective multicenter randomized controlled trial. A substantial proportion of participants reported at least moderate pain at baseline but were not selected based on preoperative pain. Women in the trial were randomized to types of vaginal reconstructive surgery and pelvic muscle training, which allowed the authors to draw conclusions in categories of physical therapy treatments and surgeries for women with and without preoperative pain. Limitations of the study include a lack of preoperative pain data, pain diagnoses, and participant medications in the OPTIMAL trial. Furthermore, the study used no validated pain scale and was limited by OPTIMAL trial data collection intervals. Thankfully, data collected at numerous points over 24 months in some regard accounted for pain symptoms over time.
The study found that, for patients with preoperative pain, significant improvement in pelvic floor symptoms and pain takes place after vaginal reconstructive surgery. Similar postoperative improvement rates were found. In addition, perioperative pelvic floor muscle training may be beneficial for patients with planned sacrospinous ligament fixation.




留言 (0)