Study design and patient population
This study was approved by the Institutional Review Board and was performed in agreement with the 1990 Declaration of Helsinki and its amendments. All patients signed a written informed consent for the therapeutic procedure. Due to the retrospective nature of the study, patient’s informed consent to the study participation was waived. We retrospectively searched the radiological information system (RIS) database of our Institution, identifying patients with HCC treated with a single-step combined locoregional therapy consisting of thermal ablation (RFA or MWA) followed by TACE between January 2017 and September 2021. Treatment decisions were based on a multidisciplinary tumor board (MDTB) consensus obtained during dedicated meetings. Indications for combined treatment were based on the following inclusion criteria: age > 18 years, Child–Pugh score A liver cirrhosis, unresectable single large (3–7 cm) HCC or multinodular HCC with no more than three nodules and a target lesion size ranging between 3 and 7 cm, and absence of vascular invasion or extrahepatic metastases on CT or MR pre-treatment studies. All patients who underwent combined treatment had already been deemed unfit for surgical resection after MDTB evaluation due to necessity of major resection in patients with severe portal hypertension (esophageal varices graded F2 according to the Japanese Research Society for Portal Hypertension, gastric varices, splenomegaly with platelet count < 100,000/mL, or current/previous ascites), unfeasible surgery due to lesion location, severe comorbidities, or patient refusal. Exclusion criteria for combined treatment consisted of age < 18 years, pregnancy or child-bearing potential, allergy to iodinated contrast medium or local anesthesia, low platelet count (< 45,000/μL), and impaired coagulation status (International Normalized Ratio – INR > 1.5). Allergy to iodinated contrast medium, low platelet count, or impaired coagulation status were considered as definitive exclusion criteria if correction (e.g. desensitizing prophylaxis, platelet infusion, vitamin K supplements) was deemed unfeasible or unsuccessful. Pre-treatment workup consisted of physical examination, laboratory tests, liver ultrasound, radionuclide bone scan, and contrast-enhanced CT of the thorax and abdomen, or contrast-enhanced liver MRI. All patients were affected by liver cirrhosis, diagnosed by histologic and/or clinical criteria (laboratory parameters, US and/or CT/MR signs). Severe portal hypertension was diagnosed by the presence of at least one of the above-mentioned criteria that excluded patients from surgical resection. HCC diagnosis was based on the guidelines in use at the time of MDTB evaluation and of combined treatment [1]. Patients with missing preprocedural and/or intraprocedural data, without post-procedural unenhanced CBCT scan, or without a 1/3-month follow-up examination were excluded from the retrospective analysis. Patients with poor quality CBCT scans due to severe image artifacts were also excluded.
Combined treatment
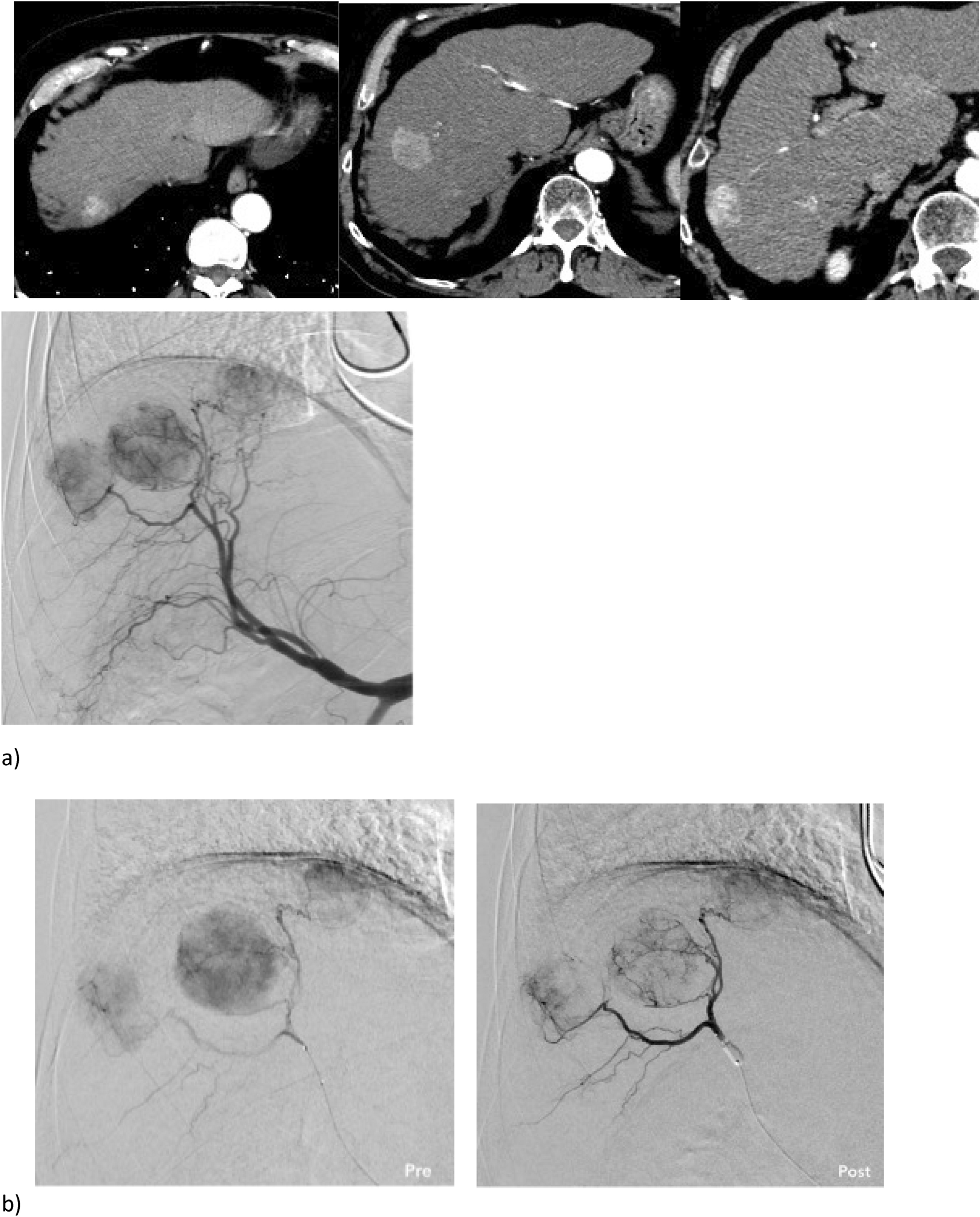
All combined locoregional treatments were performed in a fully equipped angio-suite using a single-treatment approach, by the same interventional radiologist, after antibiotic prophylaxis, with continuous patient monitoring provided by an anesthesiologist responsible for administering conscious analgo-sedation. After right common femoral or left radial access, main hepatic artery angiography was performed using a diagnostic catheter, to map liver vascularization, identify arteriovenous shunts, and to assess the feeding arteries of the target HCC. The distal tract of the segmental hepatic artery feeding the target HCC lesion was superselectively catheterized using a coaxial technique with a 2.7-Fr microcatheter (Progreat; Terumo, Japan). Thermal ablation (with RFA [RF Medical, South Korea] or MWA [Amica GEN, HS Hospital Service, Italy], based on lesion size and location, decided during the MDTB on a per-patient basis) was performed under US-guidance after local anesthesia and during patient sedation. Ablation procedures were carried out using one or more applicators, with a variable procedural time, based on the chosen technique and on lesion volume, according to the manufacturer recommendations. After the ablation, the electrode-needle was withdrawn while performing a tract-ablation, and a superselective TACE (conventional, with drug-eluting beads [DEB], or with radiopaque beads) was performed. Conventional TACE protocol was most often based on chemotherapic-in-oil (CiO) technique, in which the final emulsion contains the drug (doxorubicin, 50 mg) directly mixed in lipiodol, followed by gelfoam. DEB-TACE was usually performed using 100 micron (LifePearl, Terumo, Japan) or 100–300 micron (DC-Bead, Boston Scientific, USA) beads loaded with 50 mg of doxorubicin. TACE with radiopaque beads was performed with 70–150 micron (LCBead-LUMI, Boston Scientific, USA) beads loaded with 50 mg of doxorubicin.
The time between thermal ablation completion and TACE execution was less than 5 min. Intraprocedural contrast-enhanced CBCT was performed to identify the target tumors and their arterial feeders. The procedure was considered completed when all the drug was administered and/or slow flow was observed in the tumor-feeding artery. An unenhanced CBCT scan was acquired at the end of the procedure to check the immediate results.
Cone-beam CT imaging
CBCT technology is now wide-spread, as it is integrated in major angiographic systems (Allura XperCT, Philips Healthcare, The Netherlands; Syngo DynaCT, Siemens Healthineers, Germany). It renders a volumetric reconstruction of 2-dimensional images, obtaining satisfactory, clinically useful soft-tissue cross-sectional depiction. Over a 5-s interval, 310 projection images (at 60 frames-per-second) were acquired by the motorized C-arm at a fixed 120 kilovoltage peak (kVp) setting. The 2D images were then reconstructed into volumetric post-procedural images for a 250 × 250 × 194 mm field-of-view (matrix size 384 × 384 × 296) with a 0.6 mm voxel size. The CBCT acquisition was performed with continuous tube current modulation, obtaining an estimated radiation dose of around 3 mSv for every single acquisition, as reported by the procedural dose-report. Patients were instructed to maintain end-expiration apnea during the CBCT scanning.
Data collection, imaging evaluation and local response assessment
All data were extracted from the electronic medical records on the Radiology Information System and Picture Archiving and Communication System. Radiological report and medical records review was performed by an interventional radiologist with 5 years of experience. Review of images was performed by two interventional radiologists with 9 and 20 years of experience, respectively. All three readers were blinded to clinical, procedural, and tumor details during data collection and image evaluation. The following data were collected: patient characteristics (age, sex, underlying hepatopathy, clinical conditions [e.g.,, liver function according to Child–Pugh scale, ECOG performance status]), tumor characteristics (largest diameter, volume, number, distance and relationship with adjacent anatomical structures as well as vascularization [i.e., hypervascular or hypovascular lesions] based on CT and/or MRI imaging), and procedural details (ablation probe, TACE protocol). Lesion volume was calculated with the ellipsoid formula [17]. Technical success was defined both as correct needle placement within the target tumor, and as complete drug delivery during the TACE (or the obtainment of post-TACE flow-stasis for 10 heartbeats), with complete disappearance of tumor enhancement at post-treatment arteriography.
Unenhanced CBCT images obtained at the end of the treatment were evaluated to determine bead deposition/contrast distribution around the volume of the hypoattenuating ablation area. When any disagreements arose between the two investigators, the final decision was made in consensus.
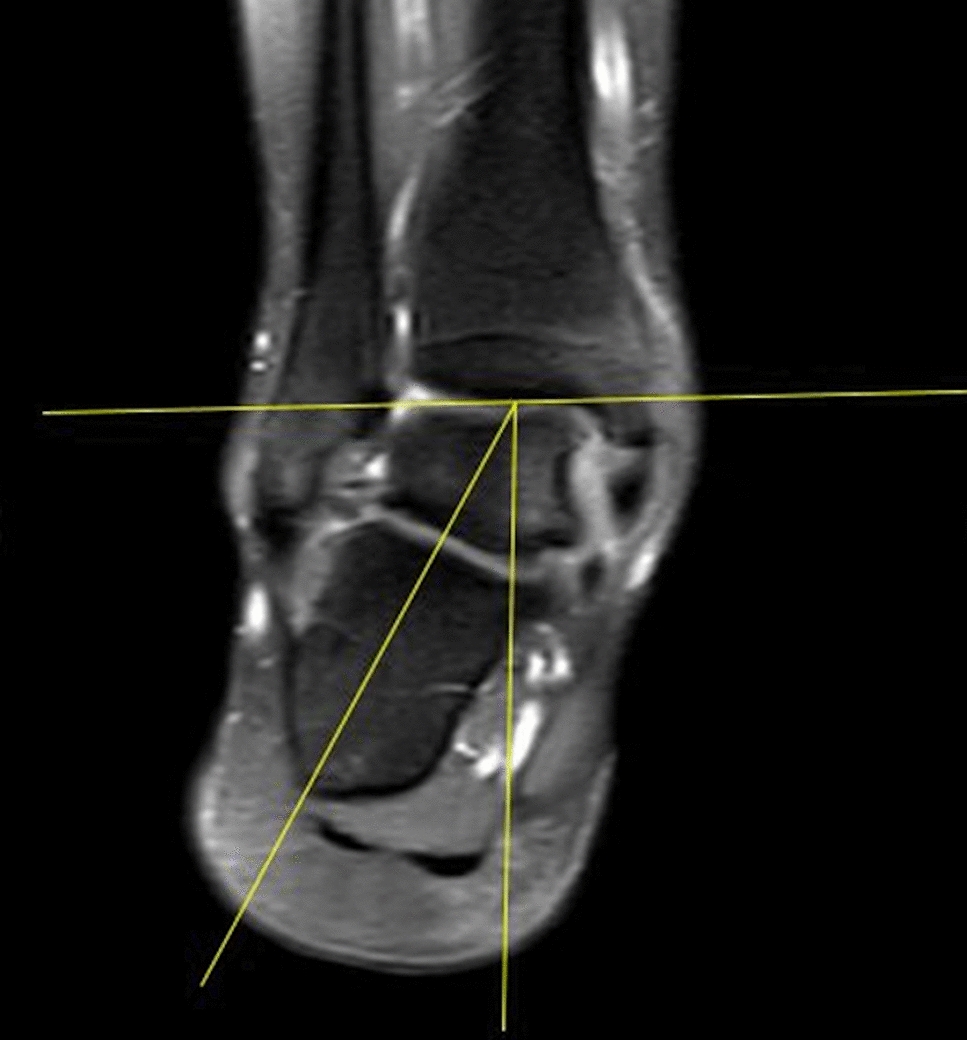
The “hug sign” was considered as: (a) complete: beads/trapped contrast agent deposition completely surrounding the post-ablation necrotic volume; (b) partial: beads/trapped contrast agent deposition incompletely surrounding the post-ablation necrotic volume; (c) absent: no beads/contrast agent around the post-ablation necrotic volume. In case of partial hug sign, the “hug sign angle” (HUGs angle) was calculated by subtracting the measured circumference without beads/contrast agent) from 360°. Treatment area was evaluated on CBCT images, including ablative necrosis and hug sign thickness. Volume assessments were obtained by manual segmentation of the necrotic area and tumor margins per single slice. To minimize errors, a mean value of two measurements was employed. Only the target tumor treated with combined procedure was evaluated.
Oncologic response of the target lesion was assessed on contrast-enhanced CT or MRI scans acquired at 1-month or 3-months follow-up, using m-RECIST criteria [18].
Primary end-point was the assessment of a correlation between HUGs angle and early tumor recurrence. Secondary end-points were assessment of technical success, patient overall survival, and treatment complications.
Statistical analysis
Continuous variables are reported as mean (± SD) and p-values were calculated with a two-tailed t-test for Gaussian continuous variables and with a Mann–Whitney U test for non-Gaussian continuous variables. Normal distribution was tested with Shapiro Wilk’s test. For categorical measures, frequencies and percentages are presented and p-values calculated with a squared-Chi or a two-tailed Fisher’s exact test as appropriate. Multivariate analysis was performed using a logistic regression model with residual tumor at 1-/3-months follow-up as dependent variable. The multivariable model included all variables considered in the univariate analysis with a p-value < 0.05; for variables included both as continuous and dichotomous, only the continuous variables were entered in the multivariate analysis due to collinearity issues. Odds ratios (OR) and 95% confidence intervals (95% CI) were reported. Statistical analysis was performed with STATA 15.1 (StataCorp LLC, USA).


留言 (0)