The urinary bladder hernia is defined as a state of sliding a part or whole bladder wall to the inguinal canal, with an incidence of 1–4% of all adult inguinal hernias [1,2,3,4]. The bladder hernia is more common in males in their 50 s than females and usually presents a groin bulge associated with voiding difficulty, double voiding, or frequent urination. The risk factors of bladder hernia are suggested to be obesity, weakening of the bladder tone and abdominal pelvic wall, and increasing intravesical pressure [10]. Soloway et al. [6] classified bladder hernias into three categories paraperitoneal type, extraperitoneal type, and intraperitoneal type. The paraperitoneal type is the most common type and is defined as the extraperitoneal portion of the bladder is involved and lies along the inner wall of the sac. Extraperitoneal type is siding only the bladder wall to the inguinal canal. Intraperitoneal type, the second most common type, is defined as the bladder entering hernia sac, thus completely covered by the peritoneum [6]. In our case, the bladder hernia was categorized as the paraperitoneal type. The patient complained of voiding difficulty in urination associated with bladder hernia because his symptoms improved completely after surgery.
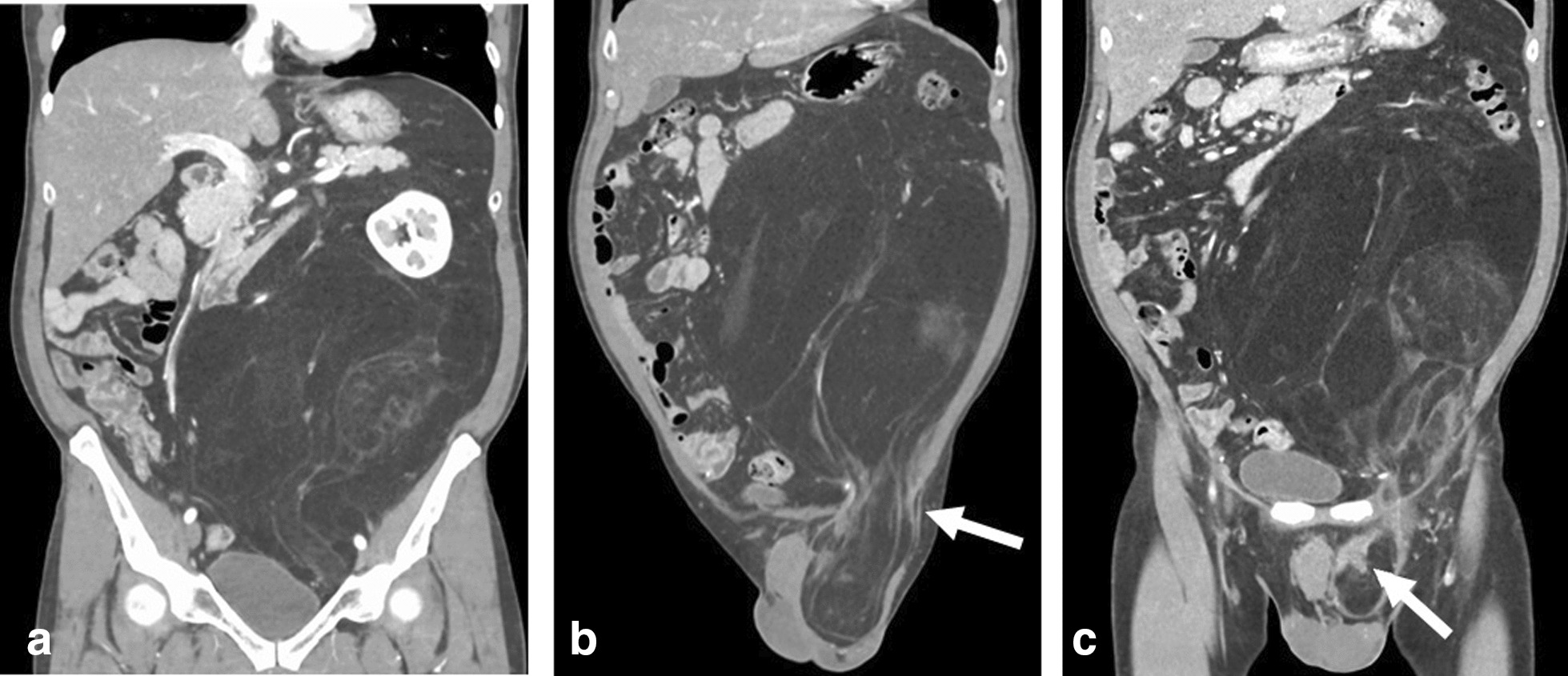
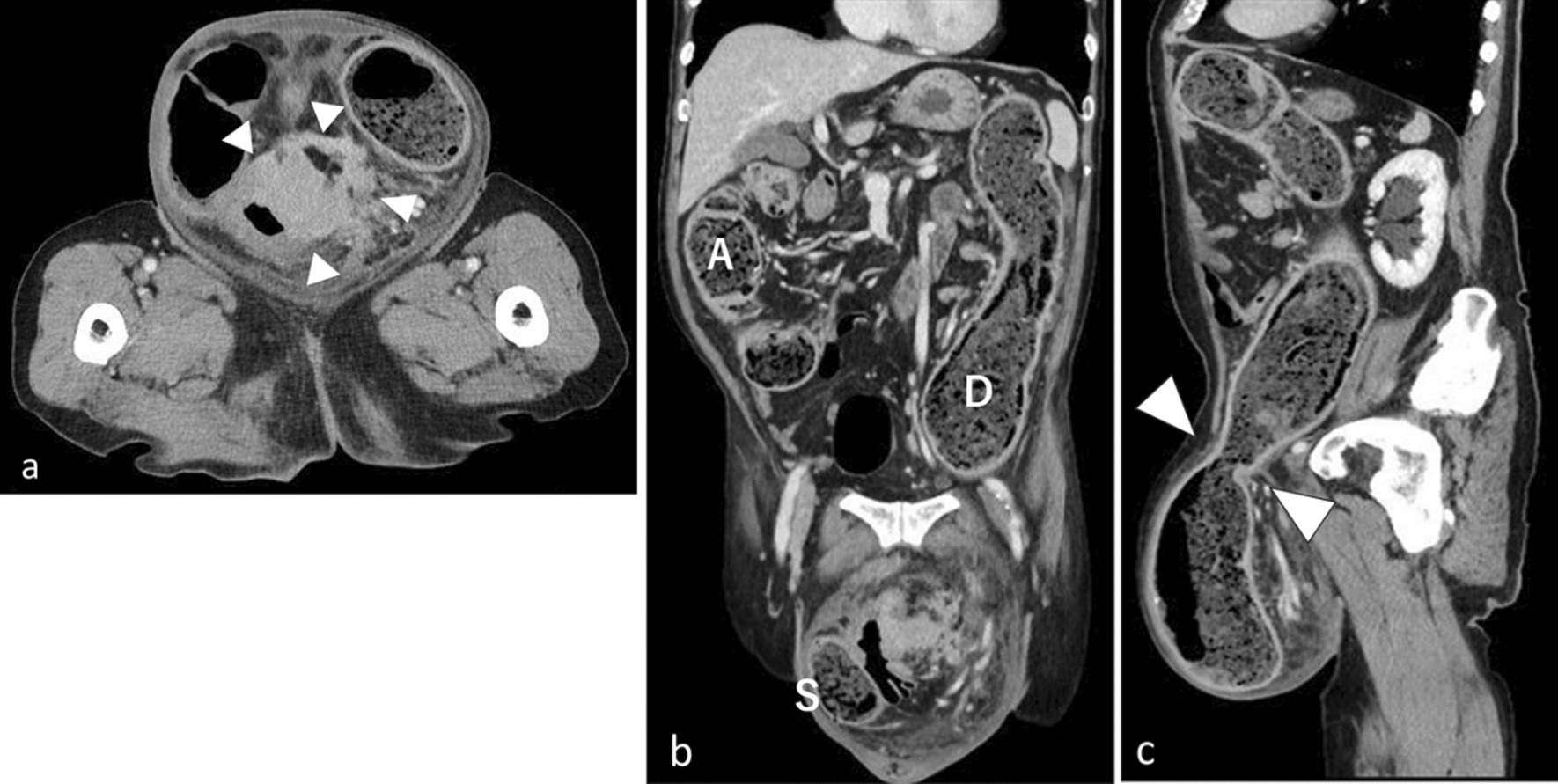
Preoperative imaging studies such as abdominal ultrasonography and CT scan are useful for the diagnosis of inguinal urinary bladder hernia [11]. Detailed evaluation with cystography or cystoscopy is also needed because a high incidence of urological malignancies (11.2%) is reported in patients with bladder hernia [12]. Unfortunately, preoperative definitive diagnosis of inguinal bladder hernia is reported to be less than 7%, and most cases are diagnosed at surgery [12]. In addition, the risk of bladder injury during surgery for inguinal bladder hernia reaches 12%, especially in cases with chronic enlarged prostate or pericystitis with firm adhesions [12, 13]. The resection of the bladder is recommended in cases with bladder tumors or necrosis, or diverticulum existing on the bladder [14, 15]. In this case, ultrasonography confirmed the bladder protruded into the inguinal canal when the bladder filled with urine, and cystoscopy showed no tumor or mucosal abnormality in the bladder. An abdominal CT scan identified the positional relationship between the inferior epigastric vessels and the protruded bladder and ruled out the presence of a bladder tumor. A precise preoperative imaging study is thus necessary for categorizing the bladder hernia type accurately, making herniorrhaphy safer, and avoiding intraoperative bladder injury.
Most patients with an inguinal bladder hernia have received open, tension-free repair, but recent laparoscopic herniorrhaphy seems to be more useful because this approach can confirm the type of bladder hernia and adequately return the protruded bladder to the normal position. There are two procedures for laparoscopic herniorrhaphy such as TAPP and TEP. Since we can diagnose the bladder hernia by precise imaging and classify it into three types preoperatively, we suggest that these procedures be selected according to the type of bladder hernia. For the paraperitoneal type, TAPP is useful because the contents of the hernia can be detected at the beginning of the surgery and injury to the bladder or bowel can be avoided. Next, TEP seems to be preferable for the extraperitoneal type because the prolapsed bladder can be easily detected during dissection and the bladder can be reduced to its normal position. Finally, for the intraparietal type, both procedures can be performed safely. Surgeons should use their experience to decide which procedure to use. Meanwhile, there are concerns about intraoperative bladder injury during laparoscopic surgery due to technical difficulties [16, 17]. Therefore, further studies are needed to clarify the superiority of laparoscopic herniorrhaphy for inguinal bladder hernia. In the present case, we utilized the HPIA technique which starts the peritoneal incision 4 cm above the hernial orifice and dissects at the dissectible layer to the hernia sac. This approach facilitated an easy and safe dissection around the protruded bladder in a cranial-to-caudal manner, leading to an accurate recognition of the whole protruded bladder and an avoidance of intraoperative bladder injury. In addition, in the case of bladder hernia observed during TAPP, the circular incision technique, which incises directly at the hernia orifice, may cause injury to the bladder. Therefore, HIPA TAPP will be advantageous in avoiding such intraoperative adverse events.







留言 (0)