
記住我


This was a randomized controlled trial that was registered in the Registry of Clinical Trials (code: NCT04478162). Premature infants and their parents were included in the control and intervention groups. The FICare model was applied to the parents of premature infants in the intervention group, and the NICU standard care was applied to the parents of premature infants in the control group.
SamplePremature infants who were hospitalized for at least 7 days between February 6, 2020, and August 15, 2021, in the NICU of a training and research hospital formed the population of the study. The NICU of the hospital has a capacity of 42 beds (2nd and 3rd level), and ~700 newborns are hospitalized annually. The participants of the study were calculated in accordance with the intervention group selection criteria and by performing power analysis. Power analysis was performed using GPower (v3.1.7) program. The effect range value was taken as 0.70 as the method used in cases where it is unknown how many units difference is significant between the groups. In cases where Type 1 error probability (a) was 0.05 (at a confidence level of 95%), at a power level of 80% and the effect range was 0.70, the study was planned with a total of 68 parents, including 34 parents for each group. At the end of the study, a post hoc power analysis was conducted to determine the adequacy of the sample size. As a result of the power analysis, for the details of the difference between the groups in terms of the scale score of fathers with premature babies in the neonatal intensive care unit, type 1 error: 0.05, n: 68 people, effect size = 1.990, and the power level according to the structure was determined as 1.000. To determine the difference in terms of the scale score of mothers with premature babies in the neonatal intensive care unit, type 1 error: 0.05, n: 68 people, effect size = 2.586 and power level according to temperature was determined as 1.000. These values show that the sample size is sufficient [15].
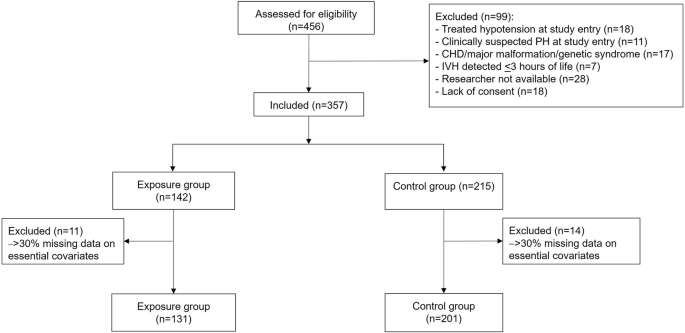
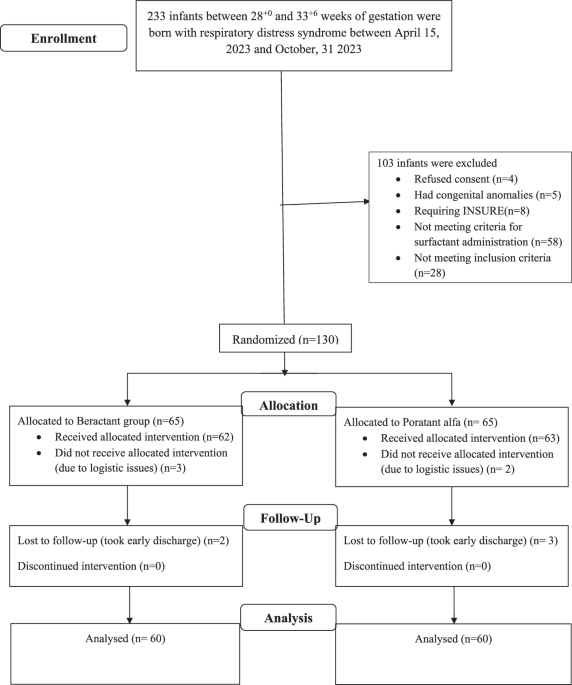
Of individuals meeting the inclusion criteria, 34 were assigned to the intervention group and 34 to the control group (Fig. 1). Premature infants and their parents were included in the control and intervention groups. Blinding could not be done to prevent the groups using the same mother’s hotel from being affected by each other. Therefore, the data of first the control group and then the intervention group were collected. “Control” and “Intervention” were written in closed envelopes to determine which group to start with first. The nurse in charge of the NICU, who was not the author of the study, was asked to choose an envelope. Since the standard care group appeared in the first selected envelope, it started to work with this group first. The FICare model was applied to the parents of premature infants in the intervention group, and the NICU standard care was applied to the parents of premature infants in the control group.
Fig. 1
CONSORT flow diagram of the study.
The inclusion criteria for preterm infants were as follows:
(1)Birth of the infant at the 28th–34th weeks of gestation,
(2)First parenting experience of the mother and the father,
(3)Parents’ willingness to participate in the study and being open to communication,
(4)Mother having breast milk,
(5)Staying in the NICU for at least 1 week,
(6)Participation of parents in the discharge training program.
The exclusion criteria for preterm infants were as follows:
(1)Undergoing a surgical intervention,
(2)Death of the baby,
(3)Transfer of the baby to another hospital,
(4)Failure of the parent to complete all phases of the study.
ProcedureThe forms used in the study were filled out within the first 48 h after the birth when the mothers and fathers in the groups felt fine and could establish healthy communication with the researcher (XX). The study was terminated by having the same forms filled out again within 24 h at the latest before discharge.
InterventionAll phases of the FICare model have been implemented. Parents in the intervention group were included in a 1-week training program within the scope of the Family Integrated Care model. A maximum of four couples attended the training in each session. A training program was also organized at weekend for those who could not attend it during the week. Training subjects consisted of the importance of breast milk, breastfeeding positions, hygienic care practices (eyes, nose, mouth, ears, skin, diaper change), bathing, nail clipping, kangaroo care, drug administration, first and emergency support, safe sleep, doctor check-up times, and vaccine follow-ups. Care practices were first shown on the model infant, and parents were asked to practice on the model. If parents did not understand certain points, they would be allowed to meet one-to-one every Monday morning. An average of 3-h training on FICare was given to healthcare personnel in the NICU. Moreover, a 4-h training on Family Integrated Care practice was organized for nurses working in the NICU. The process was coordinated by a senior nurse in the NICU. Parents who completed their training were enabled, with the support of nurses in the NICU, to take care of their infants and practice until they could do it on their own. When the clinical stabilization of their infants was achieved, parents were asked to attend at least three caregiving sessions and stay in the hospital for an average of 6–8 h. While preparations for discharge continued, peer interviews were held with experienced parents whose premature infants had been discharged from the NICU before. At discharge, a guide was given as a summary of the training program to facilitate the home transition. Furthermore, manual milking was taught in the first 6 h after birth, and the milking and breastfeeding process was supported by a lactation counselor.
ControlIndividuals received standard care provided by nurses from the time the premature infant was admitted to the NICU until discharge. The usual care process is carried on between the nurse and the mother. Mothers are allowed to perform limited care practices (bottom cleaning, breastfeeding) that the nurse considers appropriate. Mothers of babies who are planned to be discharged start staying in the hospital ~2 days before. Fathers are only informed and not included in the care.
Measures and instrumentationsThe discharge weight of the infants in the groups, the number of days spent in the NICU, the first breast milk intake, breastfeeding for the first time, and the time of transition to full enteral feeding were evaluated. The total scores of the scales applied to parents were calculated.
InstrumentsMother, father, and infant descriptive information formThe form includes questions about the mother’s/father’s age, education level, employment status, income status, family type, mode of delivery, infant’s sex, birth week, birth weight, discharge weight, feeding process in the NICU, and the number of days spent in the NICU [1, 2, 7, 8].
The scale for the readiness of the mother with a premature infant in the neonatal intensive care unit for discharge and home careDeveloped by Tiryaki and Çınar [16], the scale consists of 22 positive items of seven-point Likert type and four (feeding, perception of general condition, hygienic care, care practices) sub-scales. Each item in the scale is scored between 1 and 7 from, and the total scale score is obtained with the sum of the scores. A minimum score of 22 and a maximum score of 154 are obtained from the scale, and high scores indicate that parents’ readiness for discharge is high. The total variance of the scale is 72.886%. In the study in which the scale was developed, the intraclass correlation coefficient for mothers was found to be 0.835. The Cronbach’s alpha value of the developed scale was found to be 0.911.
The scale for the readiness of the father with a premature infant in the neonatal intensive care unit for discharge and home careDeveloped by Tiryaki and Çınar [16], the scale consists of 20 positive items of seven-point Likert type and three (feeding and care support, hygienic care, care practices) sub-scales. Each item in the scale is scored between 1 and 7 from, and the total scale score is obtained with the sum of the scores. A minimum score of 20 and a maximum score of 144 are obtained from the scale, and high scores indicate that parents’ readiness for discharge is high. The total variance of the scale is 67.36%. In the study in which the scale was developed, the intraclass correlation coefficient for fathers was found to be 0.942. The Cronbach’s alpha value of the developed scale was found to be 0.948.
Ethical issuesPermission was obtained from the institution where the study would be conducted and from the Clinical Research Ethics Committee of Sakarya University Faculty of Medicine (Approval number: 16214662/050.01.04/14). Verbal and written consent was received from the parents of premature infants after informing them about the purpose of the study, the design of the study, and how the data would be used.
Data analysisThe data were transferred to the IBM SPSS Statistics 23 program and completed. While evaluating the study data, frequency distribution (number, percentage) was given for categorical variables and descriptive statistics (mean, standard deviation) for numerical variables. The independent sample t-test was used to check whether there was a difference between the groups. The chi-square test was conducted to examine the relationship between the groups and categorical variables. Moreover, the dependent sample t-test was applied to examine changes over time. p < 0.05 was considered significant.
留言 (0)