
記住我








Fractures of the lower arm (distal radius and/or ulna) or carpal bones, collectively called “wrist fractures,” are a type of major osteoporotic fracture. Most lower arm and wrist fractures occur in women; the age-adjusted female to male ratio is 4:1 [1]. The mean age of wrist fracture is 60 years, in contrast to 81 years for proximal femur fracture [2]. The age-related incidence of wrist fractures varies notably from those of vertebral and hip fractures [1]. The incidence of forearm fractures in women rises rapidly after the menopause transition and then reaches a plateau after approximately age 65 years [1]. Wrist fractures are the most common type of clinical fracture among younger postmenopausal women [2]. Wrist fractures often occur among relatively healthy older people [1]. For example, compared with persons who have hip fracture, persons with wrist fracture are less likely to have impaired walking ability and more likely to go outdoors frequently [3]. Compared to women without fracture, women with wrist fractures are more likely to walk at a brisk pace [4]. Wrist fractures often occur as a result of a fall in women who are relatively healthy and active and have good neuromuscular function [5]. In aggregate, data suggest that wrist fractures most commonly result from a fall sustained while walking when the individual is still able to mount a protective response such as stretching out the hand or arm.
Most previous studies examining physical functioning after fracture have focused on hip fracture (after which only 40% of patient fully regain their pre-fracture level of independence [6]), whereas little attention has been paid to the trajectories of physical functioning after upper extremity fracture. If wrist and lower arm fractures are associated with declines in physical function trajectories, this finding has implications for clinical practice. For example, patients at high risk of decline in physical functioning after wrist or lower arm fracture should be targeted for interventions, including referral to physical therapy and occupational therapy to prevent or slow the rate of decline. Previous studies reported impaired physical functioning in several domains of activities of daily living following wrist fracture, including impairments in descending stairs, cooking meals, and shopping, and loss of grip strength [7,8,9,10]. To yield better insights into the effects of lower arm and wrist fractures on physical functioning, studies should include long-term follow-up and a non-fracture control group. Three longer term studies with a control (non-fracture comparison) groups have been performed [11,12,13], but only one of them compared results by age (younger women aged 50–64 years versus older women aged 65–99 years) [12]. Overall, associations of lower arm or wrist fractures with long-term physical functioning trajectories among postmenopausal women with a broad age range are not well-characterized.
The goal of this study was to evaluate change in physical functioning before versus after lower arm or wrist fracture during approximately 5 years of follow-up and determine whether these 5-year trajectories after fracture differed by age. In this nested case–control study, our research question was as follows: In postmenopausal women, what is the trajectory of physical functioning before versus after lower arm or wrist fracture, and does this trajectory of physical functioning differ by age? We hypothesize that lower arm or wrist fracture would be associated with declining trajectory of physical functioning several years after fracture and that the declines in physical functioning following lower arm or wrist fracture would be more pronounced among older compared with younger subgroups of postmenopausal women.
Methods.
Women’s Health Initiative Study DesignWe performed a nested case–control using the Women’s Health Initiative Study data. This study included data from the WHI Observational Study and the WHI Clinical Trials. The Women’s Health Initiative Study (WHI) was carried out at 40 clinical centers in the U.S. Details of the WHI Study design has been described in detail previously [14,15,16,17,18,19,20,21]. The WHI Observational Study and Clinical Trials enrolled postmenopausal aged between 50 and 79 years who were free of serious medical conditions at baseline. The WHI Extension studies followed all consenting participants from the observational study and clinical trials. WHI Extension Study 1 occurred between 2005 and 2010; WHI extension study 2 is ongoing (2010–2027).
Assessment of physical functioning levelDuring Extension Study 1 and Extension Study 2, physical functioning was assessed annually using the physical functioning subscale (10 items) of the RAND 36-item Short-Form Health Survey [22]. The 10 items assessed limitations in “vigorous activities (e.g., running, lifting heavy objects, or strenuous sports),” “moderate activities (e.g., moving a table, vacuuming, bowling, or golfing),” “lifting or carrying groceries,” “climbing several flights of stairs,” “climbing one flight of stairs,” “bending, kneeling, stooping,” “walking more than a mile,” “walking several blocks,” “walking one block,” and “bathing or dressing yourself.” Each of the 10 items had three response choices: limited a lot (score 0), limited a little (score 50), and not limited at all (score 100) (Supplemental Table 1). The well-validated SF-36 physical function score has been widely used to assess physical functioning limitations. The SF-36 physical function score is associated with objective performance-based measures of physical functioning [23, 24], adverse health outcomes, and mortality [25].
Table 1 Demographic and physiologic characteristics of study participants*Scores for the 10 items were averaged to obtain the overall physical functioning score for each participant. The total physical functioning score ranged from 0 to 100 with a higher score indicating better physical functioning. For each participant, up to six data points within 6 years of the initial matched physical functioning time point were used.
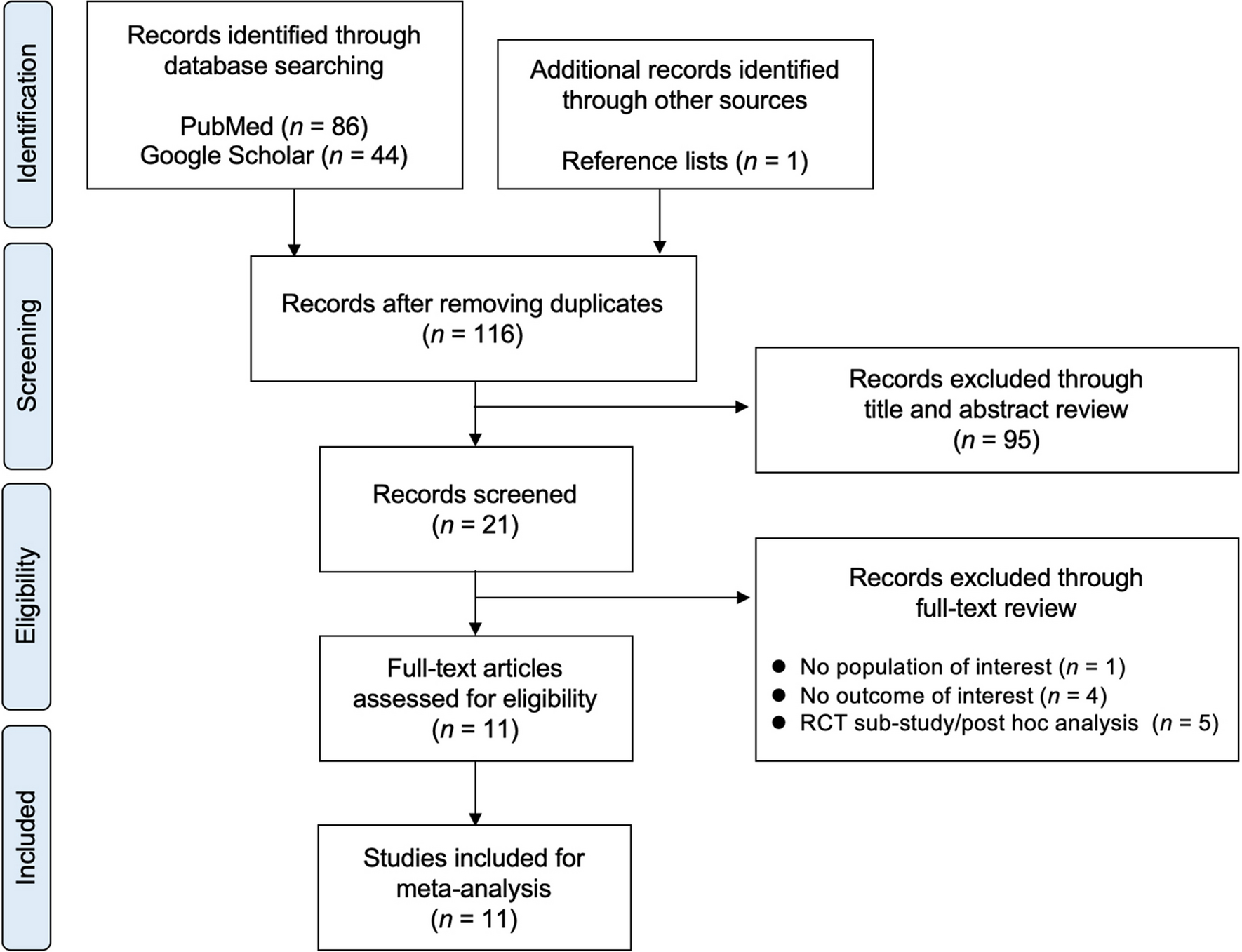
Case definitionThe algorithm for selection of cases and controls is displayed in Fig. 1. Cases were all participants with self-reported incident lower arm or wrist fracture during WHI Extension Study 1 or WHI Extension Study 2, during which physical functioning assessment was performed yearly by WHI. Of the 115,407 participants of the Extension Studies, information was available regarding model covariates (age, body mass index [BMI], smoking, alcohol intake, physical activity, myocardial infarction, stroke, treated diabetes, and cancer) for 113,056 participants.
Fig. 1
STROBE analytic flow diagram
Selection of cases and controlsThe algorithm for selection of cases and controls is displayed in Fig. 1. For cases, from the pool of 7571 participants with an incident lower arm or wrist fracture during WHI Extension Study 1 or WHI Extension Study 2, we excluded cases who had a lower arm or wrist fracture prior to the WHI Extension Studies (n = 4,498). This exclusion was necessary because there was no yearly assessment of physical function during the main WHI study; physical functioning assessments began during WHI Extension 1. We also excluded data from participants who did not provide information regarding physical functioning at the most recent visit before the lower arm or wrist fracture (n = 902) and at least one measure of physical functioning after the fracture (n = 86), resulting in 2099 cases. For controls, from the pool of 105,485 participants without a lower arm or wrist fracture, we excluded data from those who did not provide information regarding two consecutive physical functioning measures, resulting in a pool of 98,374 controls eligible for matching with cases.
We used frequency matching to match each participant who reported a lower arm or wrist fracture with 10 control group participants without lower arm or wrist fracture, by age at initial physical functioning measurement and initial physical functioning level (0 to 100), ensuring balance on these two predictors of physical function trajectory. The initial (pre-fracture) physical functioning level and age of the case became the matched control’s “baseline” time point at which we matched the corresponding control’s age and physical functioning level to that of the case. Once a given control group participant was matched, the participant was removed from the control pool to avoid duplicate selection. Ultimately, 2097 of 2099 cases were successfully matched to 10 controls each. The final analytic sample consisted of 2097 cases and 20,970 controls. Mean (SD) of total physical functioning measurements was 5.2 (1.5) in cases and 5.0 (1.4) in controls. Cases and controls were balanced on age at initial physical functioning measurement (mean 74.9 years) and initial physical functioning score (mean 71.3).
Each participant provided written informed consent and each institution obtained human subjects committee approval.
Assessment of lower arm and wrist fractureFractures were self-reported annually by participants. Participants were asked “Since the date on the front of this form, has a doctor told you for the first time that you have a new broken, fractured, or crushed bone?” Participants were asked to report the location of the fracture using the following response choices: hip, upper leg (not hip), pelvis, knee (patella), lower leg or ankle, foot (not toe), tailbone (not coccyx), spine or back (vertebra), lower arm or wrist, hand (not finger), elbow, upper arm of shoulder, jaw, nose, face, and/or skull, finger or toe, ribs and/or chest or breast bone, and cervical spine/neck. The fracture outcome of this study was lower arm or wrist fracture, to match the categories.
Assessment of other covariatesFor each covariate, we used the most recent data available, i.e., at the time of, or the most recent measurement before, each participant’s initial physical functioning measurement. At baseline, self-assessment questionnaires assessed participant age, race, ethnicity, highest educational attainment, and income. Subsequent questionnaires prospectively collected information regarding cigarette smoking, physical activity level, previous stroke, chronic obstructive pulmonary disease, diabetes mellitus, cancer, dementia or Alzheimer disease, and cardiovascular disease. For this study, we used the most recent information available for each participant, i.e., at the time of, or most recent prior to, initial physical functioning assessment.
Weight and height were measured at baseline and during follow-up (i.e., year three for observational study participants and annually for clinical trial participants during the clinical trial period). BMI was calculated as body weight in kilograms (kg) divided by the square of height in meters. The most recent BMI data (prior to, or at time of initial physical functioning assessment) was used for each participant.
Statistical analysisWe used SAS Proc Traj (SAS for Windows version 9.4, SAS Institute Inc., NC, USA), which is a trajectory procedure that uses a combination of hierarchical and latent growth curve modeling [26] to identify subgroups of participants with different physical functioning trajectories. We specified cubic modeling, which resulted in three physical functioning trajectory groups: decline in physical functioning, no change in physical functioning, and improving physical functioning. We fit logistic regression models with hierarchical adjustment levels, to examine associations of lower arm or wrist fracture with physical functioning trajectory group. The outcome of the logistic regression models was declining physical functioning trajectory, where the reference group was stable or improving physical functioning trajectory. Only 4.5% of cases and 5.4% of controls experienced improving physical functioning trajectory, and these participants were included in the combined reference group of improving or stable physical functioning trajectory.
In the regression models, we first adjusted for race, ethnicity, and WHI study component (Clinical Trial, Observational Study). Subsequent models further adjusted for cardiovascular disease, cancer, and treated diabetes at baseline. Fully adjusted models additionally included the following covariates: BMI, smoking, alcohol intake, and physical activity level. Covariates were selected a priori based on prior literature regarding factors associated with disability in older adults, e.g., cardiac disease, diabetes mellitus, cancer, and obesity [27]. Finally, we stratified results according to subgroups of interest designated a priori: age group at baseline (< 70 years, 70–79 years, ≥ 80 years), baseline physical functioning score (0–60, 65–80. 85–100), BMI category (< 25, 25 to < 30, ≥ 30), baseline physical activity level (< 5, 5 to < 15, ≥ 15 metabolic equivalent-hours/week), and Alzheimer disease [28]. Due to imbalance of matching factors (i.e., age and initial physical functioning score) across certain subgroups, analyses stratified by body mass index, physical activity, cardiovascular disease, and Alzheimer disease status were additionally adjusted for age and physical functioning score.
In a sensitivity analysis, we repeated the regression models after excluding any participants (n = 1567) who reported a fracture other than lower arm or wrist fracture at any point between their initial and final physical functioning measurement, additionally adjusting for initial physical functioning score and age at initial physical functioning assessment.
A two-sided P < 0.05 was considered statistically significant.
留言 (0)