
記住我









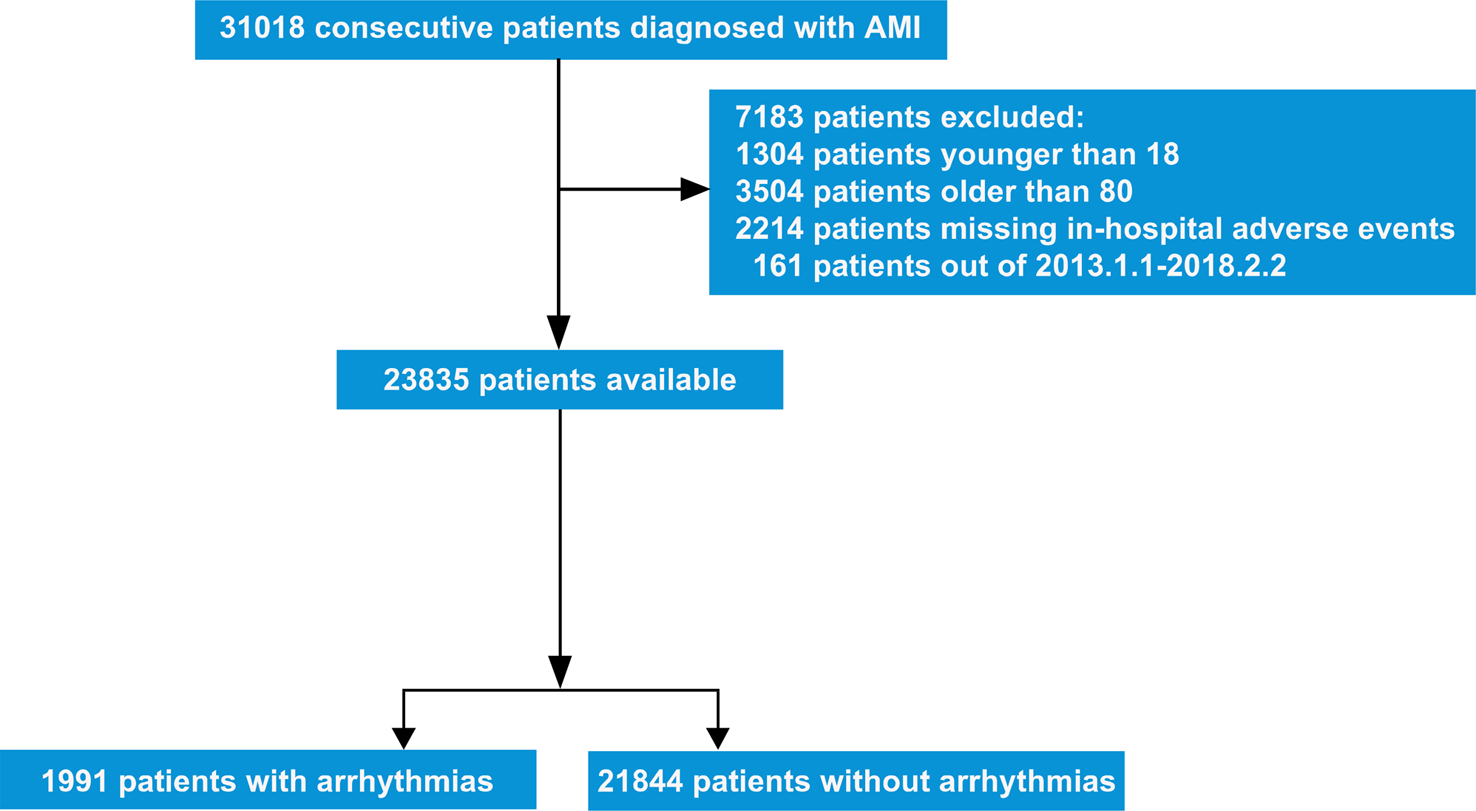
A 21-month-old female infant was admitted to the pediatric emergency room due to intermittent vomiting for one week and lethargy for one day. During the initial assessment, the patient was observed to have bradycardia, with a heart rate ranging from 60 to 70 bpm. Additionally, the electrocardiogram (ECG) revealed evidence of second-degree type II atrioventricular block (AVB), characterized by a 2:1 atrioventricular conduction ratio (Fig. 1A).
Fig. 1
Upon admission ECG and pacing ECG. A Admission ECG: sinus rhythm, second-degree AVB (type II), ventricular rate was 67 bpm. B Postoperative pacing ECG: QRS duration was 134 ms
After admission, the patient experienced a sudden episode of ventricular tachycardia and cardiac arrest. Following cardiopulmonary resuscitation, the patient regained consciousness and normal heart function. The infant had a full-term natural birth, and her developmental milestones were consistent with those of other children her age. On the day of admission, her weight was 15 kg, and a family history revealed that the father had a permanent pacemaker implanted due to third-degree AVB. A routine examination was performed, and reversible causes were ruled out, but the AVB did not recover. One week later, the patient underwent permanent pacemaker implantation using a single-chamber pacemaker (Medtronic™ SESR01) and SelectSecure™ 3830 lead under general anesthesia. The puncture of the left subclavian vein was unsuccessful, so a catheter delivery sheath (Model C315-S5, Medtronic™) was inserted into the right ventricle (RV) via the right subclavian vein. The 3830 lead was threaded through the delivery sheath and navigated to the middle septum of the RV (Fig. 2A, B and C), where it was screwed in place. Intraoperative bedside echocardiography was implemented to determine the appropriate position of the electrodes. The sensing and capture thresholds were acceptable, with a sensed R wave of 12 mV and a threshold of 1.0 V / 0.4 ms. The pacing duration of the QRS complex was 134 ms (Fig. 1B). After removing the C315 sheath and cutting it into the right atrium (RA), the 3830 lead was looped in the RA to anticipate future growth needs.
Fig. 2
Radiology of the pacemaker implantation and follow-up. A, B and C are the X-ray images obtained during pacemaker implantation from AP, RAO, and LAO views. The 3830 lead was made into a redundant loop for a reservation of the growth in the RA. D and E are the anteroposterior and lateral chest radiographs at a 3-year follow-up. F and G are the anteroposterior and lateral chest radiographs in 5-year follow-up. The length of lead reserved in the RA is decreasing (AP: anteroposterior, RAO: right anterior oblique, LAO: left anterior oblique)
One month after the operation, the pacemaker parameters were found to be optimal, with a threshold of 0.625 V / 0.4 ms, sensed R wave of 12 mV, and impedance of 475 Ω. A low limit frequency of 90 bpm was then set. A 3-year follow-up revealed that the position of the lead was normal (Fig. 2D and E). During the 5-year follow-up, the patient underwent an examination which showed that her growth and development were normal (Fig. 2F and G). Pacemaker programming confirmed stable lead parameters and normal pacemaker function. Although the chest radiograph indicated a reduced lead loop in the RA, the lead length was sufficient. Transthoracic echocardiography (TTE) showed normal cardiac function.
Case 2An 8-month-old male infant was admitted to the hospital following a transient loss of consciousness. Two days before admission, the baby experienced intermittent feeding and cyanosis around the mouth while crying. The following day, the baby had an episode of twitching, loss of consciousness, and paralysis of the limbs after crying, which lasted for 3–4 min. Concerned by these symptoms occurring multiple times, the parents sought medical treatment. During pregnancy, the fetal heart rate was found to be slow, ranging from 50 to 60 bpm. At birth, the baby weighed 2.5 kg and was delivered via a full-term cesarean section. However, after birth, the baby’s heart rate remained slow, leading to growth and developmental delays, and at 8 months of age, the infant was unable to sit alone. Upon admission, the baby weighed 5 kg, and ECG revealed a third-degree AVB with a ventricular rate of 42 bpm (Fig. 3A). TTE revealed a 6.4 mm left-to-right shunt in the atrial septum and a significant increase in the inner diameter of the RV by 19 mm, with an estimated pulmonary artery pressure of 50 mmHg. The left ventricular ejection fraction (LVEF) was 58%, and chest CT showed significant RV enlargement. A diagnosis of congenital third-degree AVB and atrial septal defect (ASD) was made.
Fig. 3
ECG at admission and ECG after pacing. A. ECG at admission showed third-degree AVB, and the ventricular rate was 42 bpm. B. ECG of epicardial pacing. C. ECG of endocardial pacing and the QRS duration was 137 ms
Following admission, the infant received temporary pacing treatment, and subsequently, an epicardial lead (Medtronic™ 4965) was implanted under general anesthesia. The pulse generator (Medtronic™ SESR01) was placed beneath the rectus abdominis muscle. A VVIR pacing mode was set after implantation, with a low limit frequency of 100 bpm (Fig. 3B). Following the pacemaker implantation, the infant’s growth retardation significantly improved.
Nine months after the operation, the threshold of epicardial lead was 1.25 V / 0.4 ms, and the impedance was 243 Ω. So, there was no significant change in the parameters at the implantation (threshold of 1.1 V / 0.4 ms and impedance of 360 Ω).
However, 16 months after the operation, the child experienced sudden syncope and twitching at home. The emergency ECG revealed that ventricular pacing could not be captured, and the threshold of the epicardial lead had increased significantly. The ventricle could only be captured by increasing the output voltage to 6 V / 1.0 ms. After adjusting the parameters, the estimated service life of the pacemaker was approximately half a year. TTE showed a 2.7-mm ASD, a 19-mm inner diameter of the RV, and a 65% LVEF.
To avoid further increased threshold of the epicardial lead and premature battery exhaustion, the pacemaker was replaced with a 3830 endocardial lead when the patient reached two years of age (16 months after epicardial pacing). At that time, the child weighed 11.5 kg. The 3830 lead was implanted through the left subclavian vein, and the pulse generator of the pacemaker (Medtronic™ SESR01) was placed under the pectoralis major muscle. The lead was coiled in a redundant loop in the RA to accommodate future growth needs. The epicardial lead and the previous pacemaker were removed. Echocardiography was utilized to confirm the placement of the lead anchored in RV and the redundant loop formed in the RA. The parameters were appropriately set (threshold 0.75 V / 0.4 ms, impedance 570 Ω), and the postoperative pacing durations of QRS complex was 137 ms. The pacemaker was programmed to VVIR pacing mode, with a lower limit frequency of 90 bpm (Fig. 3C). Figure 4 shows the chest X-ray images after epicardial and endocardial pacing, respectively.
Fig. 4
Chest X-ray imaging after epicardial and endocardial pacing. A The chest radiograph of an epicardial lead was implanted, and the pulse generator was buried beneath the rectus abdominis muscle. B The chest radiograph after endocardial pacing
During the 1.5 years of follow-up, the child’s growth and development were comparable to that of normal children, and the pacemaker functioned normally. The threshold and impedance of the lead remained stable.
At the most recent follow-up, conducted three years later, the patient reported no episodes of discomfort. A thorough examination, including a chest X-ray, indicated optimal positioning of the ventricular lead and generator. The ECG revealed a QRS complex pacing duration of 143 ms, as illustrated in Fig. 5. Notably, the ventricular pacing thresholds and impedance measurements were recorded at 0.88 V/ 0.4 ms and 468 Ω, respectively. TTE unveiled a 3.2-mm ASD, a 28-mm inner diameter of the RV, no tricuspid valve regurgitation, and a 54% LVEF.
Fig. 5
X-ray and ECG at the 3-year follow-up. A. Chest X-ray image from the AP view. B. Chest X-ray image from the lateral view. C. ECG displaying pacing rhythm with a QRS duration of 143 ms
留言 (0)