
記住我



A 34-year-old woman with ES was scheduled for laparoscopic total hysterectomy due to heavy bleeding during menstruation. Her weight, height, and body mass index were 73.3 kg, 1.62 m, and 28 kg/m2, respectively. She had a small ventricular septal defect at birth and was diagnosed with ES at the age of 7. She subsequently presented with severely limited exercise tolerance and began taking phosphodiesterase-5 inhibitors, prostacyclin receptor agonists, and endothelin receptor antagonists. In addition, she received home oxygen therapy. At 31 years of age, she was diagnosed with idiopathic thrombocytopenic purpura. Further, laboratory assessment revealed a mild prolongation of activated partial thromboplastin time. Since then, she had been hospitalized several times for hemoptysis and heavy menstrual bleeding.
Upon presentation to our hospital, the patient was in shock with a heart rate of 75–90 beats per minute (bpm) and arterial pressure of 86/54 mmHg due to severe bleeding. She developed progressive tachypnea; the oxygen saturation (SpO2) was around 80% during oxygen (O2) therapy using a simple face mask at a flow rate of 5 L/min. The laboratory findings were as follows: hematocrit level, 31.5%; platelet count, 10,000/µL; and activated partial thromboplastin time, 90.7 s. Arterial blood gas analysis yielded the following findings: pH, 7.445; PaO2, 47.8 mmHg; PaCO2, 29.3 mmHg; HCO3−, 19.7 mEq/L; and base excess, −3.5 mmol/L, with an O2 flow rate 5 L/min via a simple face mask. The patient also developed progressively worsening hypoxemia and cyanosis. After admission, she received a blood transfusion of red blood cells and fresh-frozen plasma, as well as intravenous immunoglobulin therapy. The perioperative team and her relatives discussed the risks of anesthesia and surgery and also considered nonsurgical management. Despite the related risks, a consensus was reached that hysterectomy was the best treatment alternative.
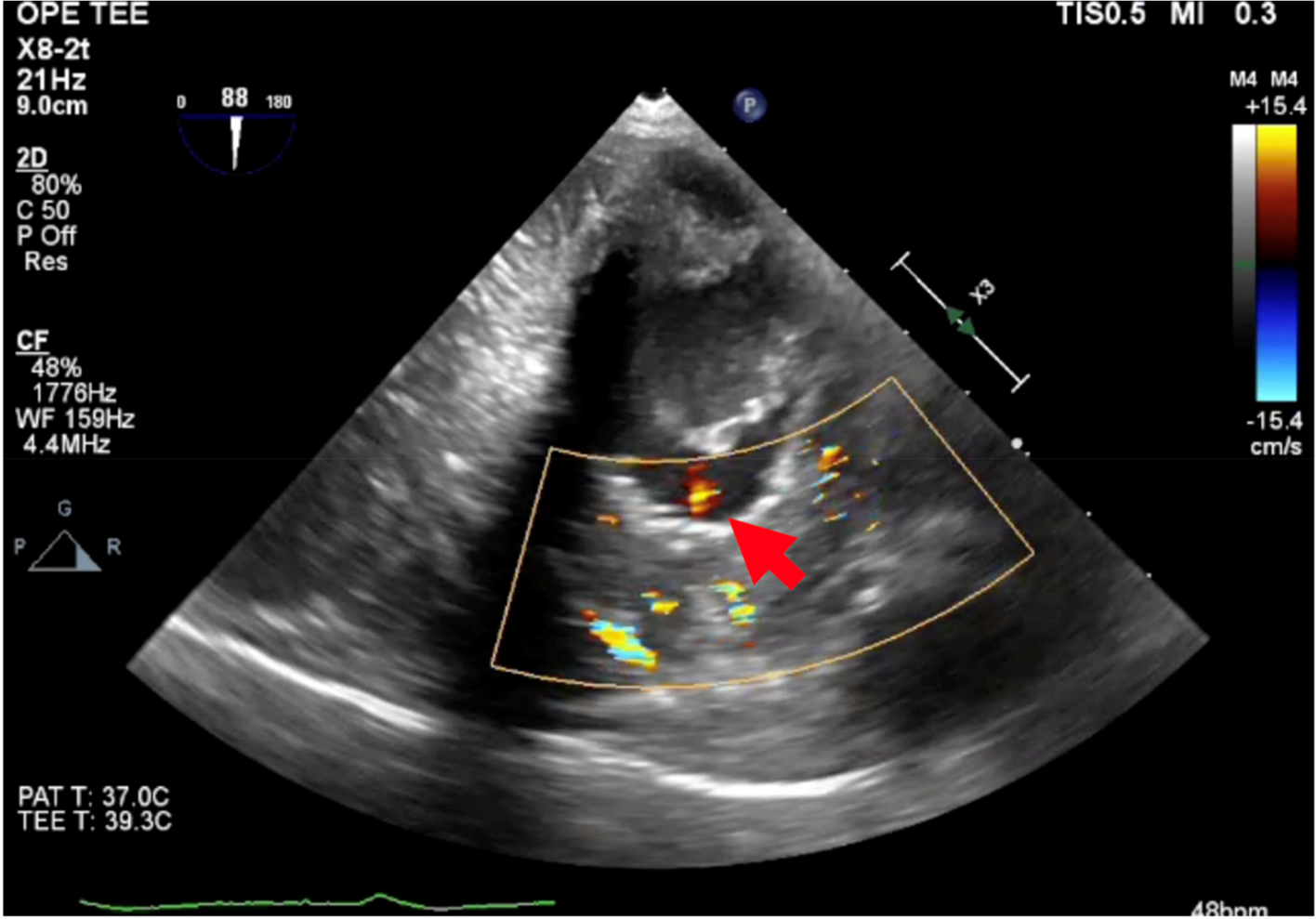
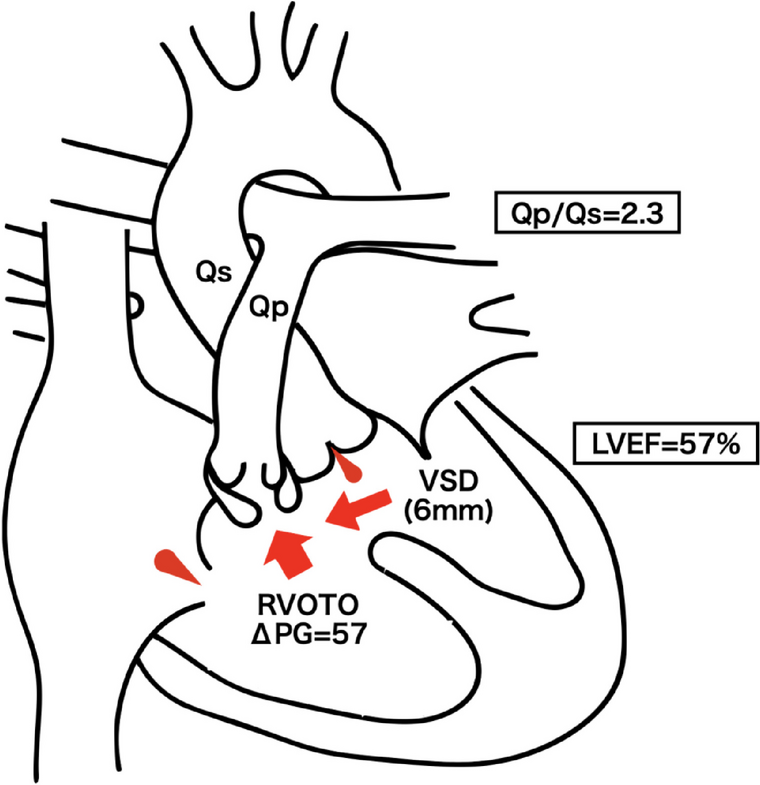
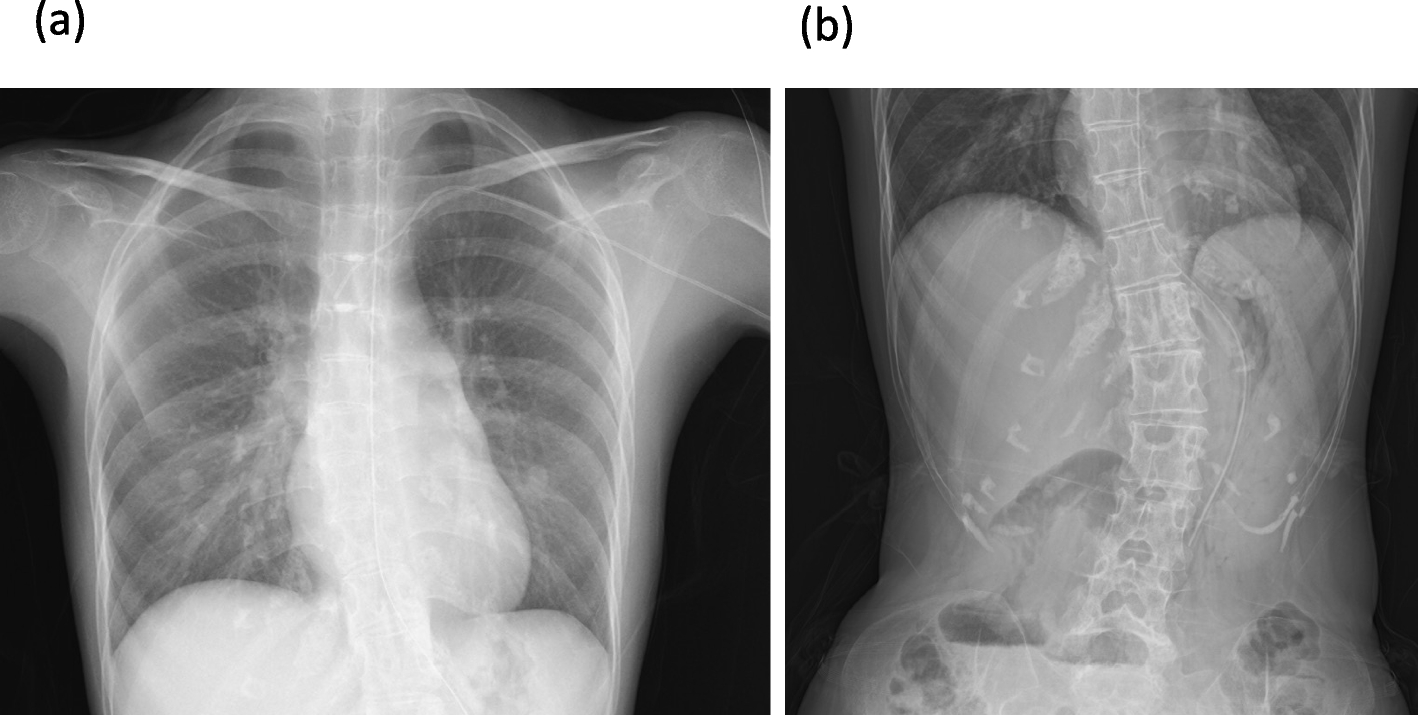
The patient underwent thorough preoperative assessment, including 12-lead electrocardiography (ECG), chest radiography, transthoracic echocardiography (TTE), full blood count, hepatic and renal function assessment, coagulation screening, and arterial blood gas analysis. Chest radiography revealed cardiomegaly, central pulmonary artery dilation, and disappearance of peripheral pulmonary vascular shadows. ECG revealed a sinus rhythm with right axis deviation and right ventricular hypertrophy. TTE demonstrated good left ventricular function; however, there was systolic displacement of the interventricular septum into the left ventricle, indicating right ventricular pressure overload. The peak gradient of tricuspid regurgitation increased markedly to 118 mmHg. The interventricular septum had a defect with a bidirectional shunt. Post-blood transfusion, blood values included the following: preoperative hemoglobin, 12.9 g/dl; hematocrit, 40.9%; platelet count, 101,000/µL; and activated partial thromboplastin time, 59.6 s.
A gynecologist recommended laparoscopy over open hysterectomy. Laparoscopic surgery involved a risk of exacerbation of the right heart failure due to changes in venous return and increased PVR due to pneumoperitoneum. Nevertheless, it was selected due to its benefits of minimal invasiveness, light pain, and faster recovery. We were prepared to switch to laparotomy if hemodynamics became unmanageable post-insufflation.
General anesthesia with peripheral nerve block was scheduled without any premedication. We used standard monitoring: ECG, pulse oximetry, end-tidal carbon dioxide partial pressure (PETCO2), noninvasive blood pressure, and bispectral index monitor (BIS™, Medtronic, Minneapolis, MN, USA). A radial artery catheter was inserted before anesthesia, and the FloTrac sensor® (ver.4.00, Edwards Lifesciences, LLC) were attached. Cardiac output (CO), cardiac index (CI), and stroke volume (SV) were evaluated using the HemoSphere monitor. Rapid anesthesia induction was achieved using 0.2 mg/kg of remimazolam, 100 µg of fentanyl, 50 mg of rocuronium, and continuous remifentanil infusion at 0.15 μg/kg/min. After tracheal intubation, transesophageal echocardiography (TEE) and central venous catheterization were performed. Additionally, rectus sheath and transversus abdominis plane blocks were administered for postoperative analgesia. Noradrenaline infusion at 0.02 μg/kg/min was started after the peripheral nerve block. Anesthesia was maintained using 1% sevoflurane and remifentanil up to 0.25 μg/kg/min, with bolus administration of rocuronium, as required.
The ventilation mode was pressure-controlled ventilation volume guaranteed (PCV-VG). Here, the target parameters were as follows: expired tidal volume, 6 mL/kg; inspiration-to-expiration ratio, 1:2; FiO2, 0.8 with air; positive end-expiratory pressure (PEEP), 5 cmH2O; and peak inspiratory pressure (PIP), ≤ 25 cmH2O. The PETCO2 was maintained at 35–40 mmHg by adjusting the respiratory rate (RR). Intra-abdominal pressure during pneumoperitoneum was maintained at ≤ 8 mmHg, with a head down tilt of 15° being allowed.
There were no acute episodes of hypotension, bradycardia, or arrhythmias during anesthesia induction or maintenance. Pneumoperitoneum or changing the patient’s position from supine to the head down position had no significant effect (Fig. 1). During pneumoperitoneum establishment, arterial blood gas analysis yielded normal findings (Table 1); blood pressure and heart rate remained unchanged, with the CI remaining at approximately 3.8 L/min/m2. Blood loss was 20 mL; accordingly, intraoperative blood transfusion was not required. The durations of surgery and anesthesia were 95 min and 183 min, respectively. The patient was subsequently extubated in the operating room.
Fig. 1
Anesthetic record. Parameters included are heart rate (bpm), saturation of percutaneous oxygen (SpO2; %), blood pressure (mmHg), central venous pressure (mmHg), cardiac index (L/min/m2), peak inspiratory pressure (cmH2O), end-tidal carbon dioxide (mmHg), and respiratory frequency (bpm). We thank you for your thoughtful suggestions and insights. The manuscript has benefited from these insightful suggestions
Table 1 Results of sample analysis and results for FiO2, SpO2, and FECO2The patient was transferred to the intensive care unit and could breathe spontaneously through a face mask with an O2 flow rate of up to 6 L/min; SpO2 was generally maintained at ≥ 90%. No episodes of hypotension occurred during the postoperative period. The patient received fentanyl infusion for 12 h at 25–50 µg/h. Analgesia was supplemented with intravenous acetaminophen. Oral administration of pulmonary vasodilators was resumed immediately on the day of surgery. The patient recovered uneventfully and was discharged 6 days postoperatively.
留言 (0)