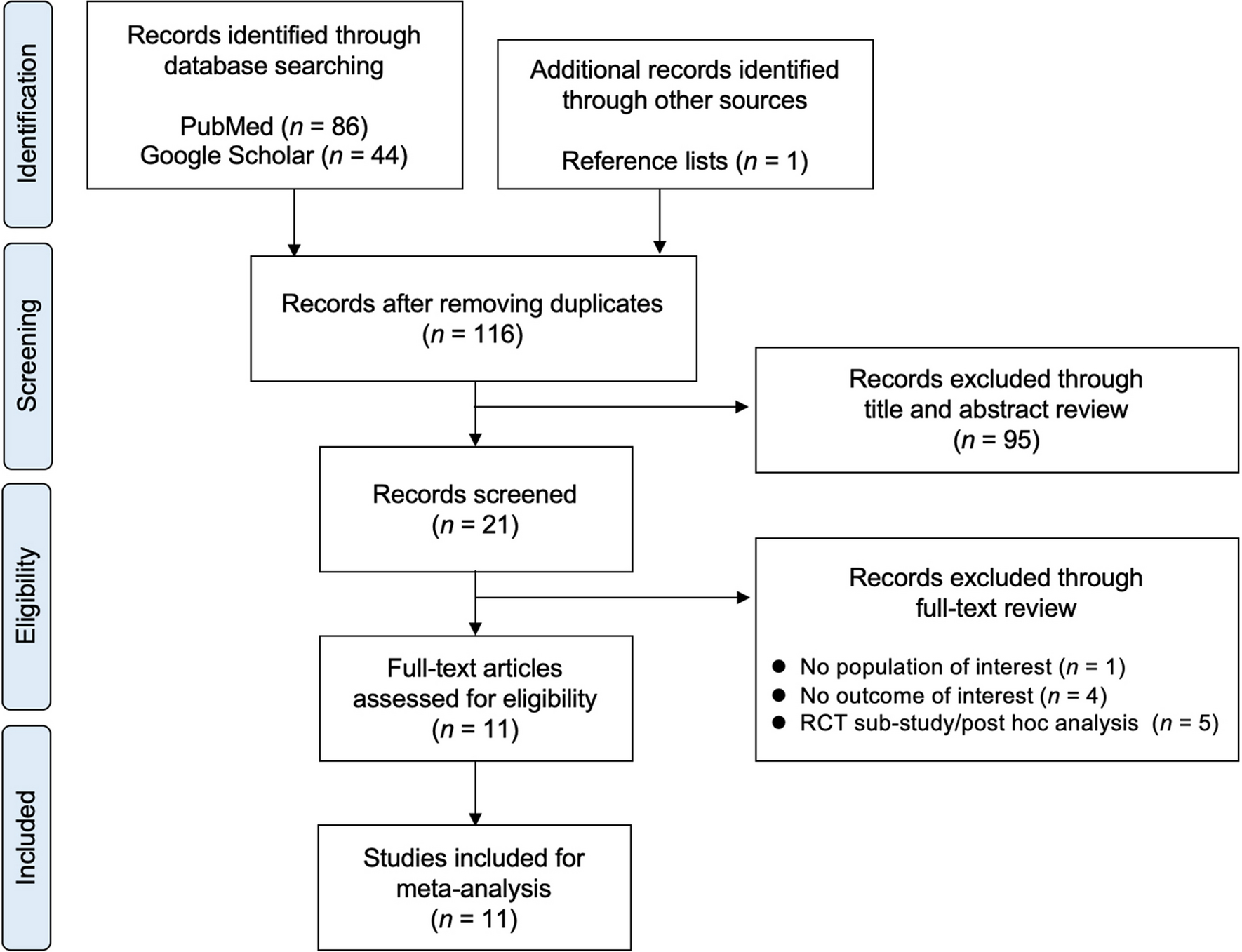
This nationwide population-level case–control study aimed to define the incidence and factors associated with an increased risk of contralateral hip fracture, and to establish the influence of contralateral fracture on early mortality risk. A total of 5566 patients sustained an index hip fracture during the study period with 138 sustaining a contralateral hip fracture within 12 months, giving an incidence of 2.5% within the first year (a 1 in 40 risk). Patients who sustained a contralateral hip fracture were significantly older at the time of index hip fracture compared to those who did not sustain a subsequent fracture. After adjusting for baseline variables, there was no difference in 30-day mortality rates between those who did and did not sustain a contralateral fracture. Socioeconomic deprivation was associated with a reduced risk of contralateral fracture, with those in the least deprived quintile demonstrating a significantly increased risk.
The finding of a 2.5% contralateral fracture rate within 1 year of index fracture is consistent with a number of non-registry studies that reported an incidence between 2.5 and 5.7% [8, 14,15,16]. Other studies are heterogenous with varying follow-up times [6, 7, 16, 17, 20], and a direct comparison is challenging. To the knowledge of the authors, there is one comparable study from Denmark which used large-scale registry data (n = 169,145) and reported a higher 12-month contralateral fracture incidence of 9% [6]. The discrepancy in the findings may be attributable to differences in inclusion criteria between the data registries, as the Danish registry included all hospital inpatient discharges. This difference may also represent advances in primary and secondary fracture prevention and the management of frailty, because Rgy et al. collected data from 1977 to 2001. Furthermore, the SHFA is a dedicated hip fracture registry, whereas the work by Ryg et al. utilised a data registry aimed to capture all hospital in-patients, regardless of diagnosis.
Current literature suggests that patients who sustain a second hip fracture have an increased early mortality risk [6, 8, 9, 21]. However, the current study conducted an adjusted analysis that controlled for confounding factors and did not demonstrate a significant difference in 30-day mortality risk between those who sustained a contralateral hip fracture and those who did not. It is likely that the small sample size of contralateral fracture patients in the present study (n = 172) may account for the difference in reported findings. It was demonstrated that advancing age and male sex were associated with increased 30-day mortality in the study population, which was consistent with previous registry-based studies [22, 23].
Demographic factors associated with a higher risk of contralateral fracture have been well-documented with increasing age, female sex and living alone being associated with a greater risk [6, 8, 24]. It may be that male sex confers a protective influence against contralateral hip fracture due to increased early mortality rates, precluding these patients from sustaining a further fracture. In the present study, mortality was only recorded as a dichotomous outcome at 30 days, and therefore competing risk analysis was not able to be performed to investigate this further. To the knowledge of the authors, there is no literature describing the influence of socioeconomic deprivation on risk of suffering a contralateral hip fracture. Socioeconomic deprivation is known to influence outcomes following hip fracture, with increasing socioeconomic deprivation associated with higher mortality and younger age at the time of fracture [22, 23, 25].The current study shows deprivation to be associated with a reduced risk of contralateral fracture. The authors recognise that those who are more socioeconomically deprived experience increased frailty, are younger at the time of hip fracture and have increased risk of not returning home following index hip fracture [22, 23, 25, 26]. This would suggest that socioeconomic deprivation may increase risk of sustaining a contralateral hip fracture; however, this does not seem to be the case. The findings of the present study are supported by Murena et al. who demonstrated that high BMI and malnourishment are associated with a lower risk of a contralateral fracture which are both traits associated with increased socioeconomic deprivation [27]. Deprived patients have a tendency to have greater multimorbidity, which may reduce their mobility and independence, increase the likelihood of being indoor home or residential care dwellers and thus reduce their risk of activity-related falls [28]. Further to this socioeconomic deprivation caries an increased risk of mortality following primary hip fracture which may contribute towards the reduced risk of sustaining a contralateral hip fracture reported in this study [22, 23].
The major strengths to the current study are the use of a large, highly validated data sample derived from a population-level specialist hip fracture registry, and the use of regression analyses to evaluate the association whilst adjusting for confounding factors. There are limitations to the current study. The data collection period was during the COVID-19 pandemic, and therefore differences in population behaviours and healthcare provision may have influenced the findings. The SHFA excludes patients who sustained a fracture surrounding a pre-existing implant (periprosthetic fractures), therefore the findings cannot be generalised to periprosthetic primary hip fractures. The use of registry data relies upon the accuracy of data collection; however, SHFA data is collected by trained clinical auditors and validated by analysts at Public Health Scotland, and were then validated further by two study authors. The use of registry data precluded the inclusion of highly granular patient-level variables related to comorbid disease and therapeutics, though this was mitigated by the inclusion of age, SIMD and ASA grade which are markers of frailty and systemic disease.






留言 (0)