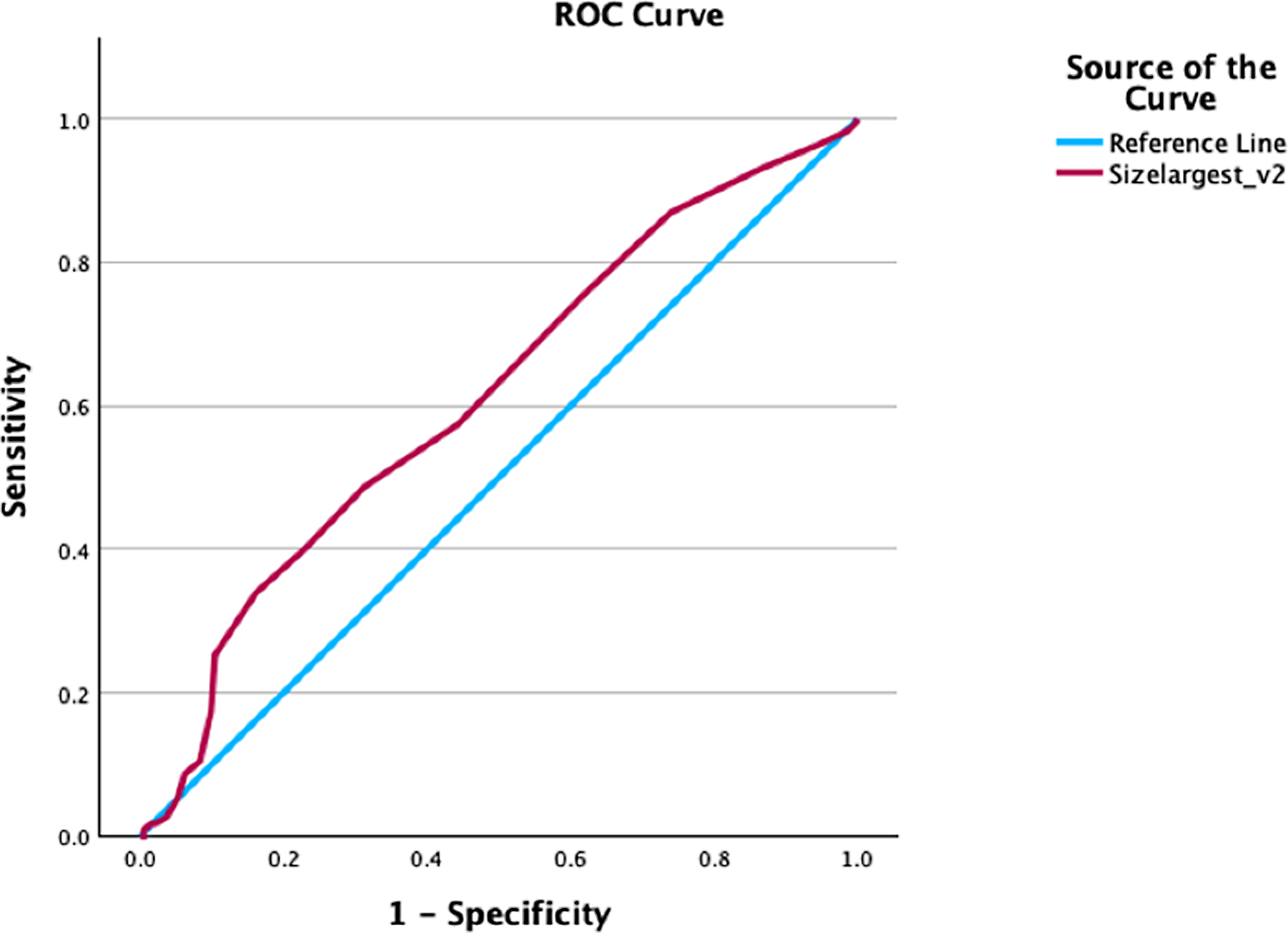
In this study, the largest diameter, area, and volume were used as spatial parameters for one-, two-, and three-dimensional measurements, respectively, in terms of natural recognition. After performing systematic analysis and comparing ROC curves, the AUC values indicated that the models including two- and three-dimensional measurements combined with patients’ clinical data had better diagnostic performance for predicting ESWL efficacy than models with one-dimensional measurements. However, we did not find a significant difference between the two- and three-dimensional measurements. Interestingly, when we included only the size parameter for the measurement, there was no significant difference in the predictive ability between the above methods in three different dimensions in most instances.
Stone load is a complex parameter that is related to many different indicators, such as size, composition, shape, and internal structure. Among them, size and composition have always been considered the two most important focuses for urologists. A previous study confirmed that there was a significant relationship between composition and the CT Hounsfield value in clinical practice [21]. With improvements in grayscale and temporal resolution, noncontrast CT has been considered the first choice for evaluating the characteristics of ureteral stones. However, to our knowledge, many factors could affect the quantitative analysis procedure. In particular, most previous studies performed a linear measurement on axial images to describe stone size. Contrary to the routine method, some researchers have consistently reported a significant discrepancy between axial and coronal orientation on the largest diameter and area, respectively, and they found that stones were often underestimated on the axial images and needed to be measured on the coronal images instead [22, 23]. The shape of ureteral stones can vary greatly from round to elongated, and the course of the ureter in the abdomen also varies. Therefore, most ureteral stones remain along the long axis orientation in the craniocaudal plane, and axial slices are usually rarely assigned to the largest diameter. In contrast to previous studies, we reconstructed the scan data in three orientations and found that the underestimation of stone size could occur randomly in coronal and sagittal reformations without any differentiation. Therefore, comparisons between the largest diameter/area from all orientations may be the most accurate method of quantitative description for further analysis.
On the other hand, the choice of window level/width for displaying the stone was also found to be an important factor in the accuracy of size assessment. For example, Argüelles Salido E et al. attributed the CT scan using the BW as the technical method with high accuracy for size determination, and the AW will overestimate [20]. Furthermore, Eisner BH et al. recommended the use of a magnified BW for CT measurement of ureteral stones as the most accurate method based on in vitro and in vivo experiments [24]. In line with the above findings, our study compared the largest diameters and areas in three orientations under both abdominal and bone window conditions. We also showed that the size and area under AW were significantly larger than those under BW. However, no significant difference was found in the diagnostic performance of measurements between AW and BW selection in predicting ESWL efficacy in this study.
Clinically, to select an appropriate treatment strategy for each individual, predicting the probability of successful ESWL is important to reduce follow-up costs after diagnosis. Previous studies commonly used both stone size and CT mean value as independent risk factors for the efficacy of ESWL [25, 26]. However, there were still significant differences in the heterogeneity of the corresponding evaluation standards. According to the AUA and EAU guidelines, the diameter has always been used as the standard parameter in most clinical centers. Although the diameter is the easiest measurement for urologists to obtain, a more accurate and convenient method to assess the stone burden is still needed. To overcome the confusion and to account for the irregular shape and complex composition of the ureteral stones, we re-evaluated the data and found that the two- and three-dimensional measurements were more valuable. However, when the mean CT value was removed, the models including one-, two-, and three-dimensional measurements were mostly not significantly different according to the comparisons of AUC. The above comparisons showed that the role of mean CT Hounsfield is important in reflecting stone density. Although the cutoff values of CT Hounsfield for assessing the likelihood of successful SWL outcome varied widely in many previous studies, there was an inverse association between stone density and SWL success, which was the same trend as our results. [9, 13, 17, 25]
In addition, our results are consistent with some previous studies on the independent factors for predicting ESWL effectiveness [15, 17, 26]. In contrast, the difference in the analytical procedure is that due to the apparent collinearity between the variables, only one of the parameters could be included in the following multivariate regression analysis if there was a highly correlated relationship. In this study, we systematically compare the size variables in terms of natural recognition from one to three dimensions in a progressive manner. Using the corresponding parameters in the multivariable logistic regression analysis, we demonstrated that the combination of size and mean CT value had the best predictive value for ESWL efficacy. However, when only the spatial parameters were included in the analysis, we found no significant difference between length, area, and volume in predicting ESWL efficacy. Additionally, considering the consistency of assessment, automated 3D volume calculation may be the best choice to avoid interobserver variability in manual two-dimensional assessment, which was the same view as in some previous studies [27,28,29]. However, in the absence of automated volume measurement software, the two-dimensional measurement combined with the mean CT value should be considered, and the predictive ability remains the same according to our results, which was different from a previous study by Yamashita S et al. [30] The reason may be that in their study, patients were followed for 3 months after ESWL, which may introduce many uncertainties into the results in the long term. Similarly, compared to early previous research, the efficacy of one-session ESWL was lower (48% versus 70%) [31]. We supposed the reason was that the endpoints of the study and follow-up methods were different, which may have significantly affected the final ESWL efficacy evaluation. In view of our clinical experience, medication, diet, and physical activity status may all affect the patients' ability to pass stones. In contrast, we called the patients back to our hospital in 3 or 4 days and compared the stone status by ultrasound or CT with the primary findings before ESWL treatment in this study, and the evaluation results would be closer to the reality of the direct efficacy of ESWL.
Our study has several limitations. First, retrospective studies cannot completely avoid selective bias, and the sample size may be limited. Second, the choice of ESWL treatment was determined by the urologist's suggestions and the patient's will, which may introduce some subjective bias. Third, there are various types of lithotripters available in the global medical market. However, there may be discrepancies in the parameter names across different lithotripsy machines. Furthermore, the range of these parameters may vary to some extent. All the above settings in clinical use were determined by the technician's experience and the patient's endurance in clinical experience, and the stopping point of ESWL also depended on the technician's suggestions. Although all technicians operating the ESWL machines had more than 5 years of experience after formal technical training in ESWL, there was still some subjective perception of the endpoint of ESWL.
In conclusion, the two- and three-dimensional measurements combining the size parameter and CT attenuation values on ureteral stones were determined to be the best predictor of ESWL efficacy compared to considering only the spatial parameter. Three-dimensional measurement using software should be considered first to avoid interobserver variability in the manual drawing process when it is convenient for the urologist to make a clinical decision for the patients.




留言 (0)