
記住我

There are varied theories on the pathophysiology of RIH. These suggest that RIH develops due to compensatory changes in CSF production, CSF reabsorption, cerebral venous outflow restriction, displacement of CSF by patching material, or a combination of these pathways [1, 3•, 6]. The following discussion on RIH pathophysiology considers similarities between SIH and IIH, specifically similarities in compensatory changes of venous flow and elastance of the craniospinal space, which are presumably also occurring in RIH.
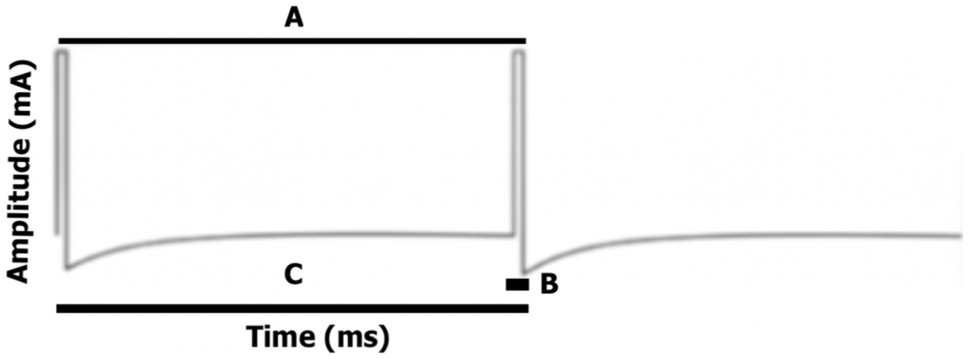
Fundamentally, intradural venous sinus pressure is a key component of intracranial pressure equilibrium as per Davson’s equation of CSF absorption [18,19,20,21]. Venous pressure also influences craniospinal elastance. Elastance measures the pressure response of the intracranial system to a known change in volume. In a state of increased elastance, a little addition of volume can provoke a disproportionate increase in intracranial pressure (Fig. 1). Increased craniospinal elastance has been shown to occur in IIH and cases of compensated SIH and may exist in patients with RIH [22, 23•].
Fig. 1
Hypothetical intracranial pressure–volume curve. As a system moves from a state of lower elastance (dotted line) to higher elastance (solid line), the same increase in volume results in higher intracranial pressure
What causes this system of increased craniospinal elastance? One reason is a venous system that is reaching the limits of its compensatory abilities. In normal physiology, veins are capacitance vessels, accommodating large volumes of blood and acting as a buffer for changes in pressure and volume. They inherently have less elastance than arteries and can distend largely to accommodate changes in volume without resulting in significant pressure shifts, and vice versa. However, venous elastance is increased in an overcompensating venous system. This means that the normal craniospinal space reserve and ability to buffer changes in intracranial volume are diminished. Increased craniospinal elastance can lead to higher ICP, which is pathological in IIH and compensatory in SIH [22, 24].
Typically, in uncompensated SIH, it is hypothesized that there is actually low craniospinal elastance, which can directly cause low intracranial pressure itself or occur due to CSF volume loss [22, 25]. This theory is supported by lumbar infusion testing showing that the pressure–volume index (PVI), or the volume that is needed to be added to raise the pressure tenfold, is higher in patients with proven CSF leaks and in patients with a short duration of the disease [25, 26]. Lower craniospinal elastance has also been shown in patients with SIH without imaging signs of compensation for CSF volume loss [22].
However, in compensated SIH, craniospinal elastance increases. Two contributing factors to increased craniospinal elastance include (1) a compensatory increase in venous volume via the Monro–Kellie hypothesis and (2) a decrease in transcranial venous outflow. In SIH, the primary mechanism for compensating for the loss of CSF volume within the enclosed craniospinal space is the macro-veins within the spinal epidural space, which distend and increase in volume as per the homeostatic principles of the Monro–Kellie hypothesis [22]. This new baseline of added volume within the epidural venous plexus subsequently increases craniospinal elastance; it compromises the craniospinal venous system’s ability to accommodate subsequent increases in volume without significant craniospinal pressure increases [22]. In normal physiology, the internal jugular veins collapse in an upright position to maintain intracranial pressure equilibrium [19, 20, 27]. Patients with compensated SIH have a disproportionate decrease in internal jugular vein (IJV) outflow to that of total cerebral blood flow (tCBF); the reduction in venous outflow is speculated to help divert flow to the epidural, vertebral, and cerebral veins and serve as another compensatory mechanism for intracranial hypotension [22]. Consequently, patients with compensated SIH with high intracranial elastance are also noted to have higher opening pressures than those without increased intracranial elastance [18]. Other studies show that opening pressure increases with the length of the symptom duration in patients with SIH, presumably due to compensatory mechanisms [26, 28].
Like in SIH, in IIH, cerebral venous sinuses initially distend. In the case of IIH, initial venous distension occurs to accommodate for increases in abdominal and central venous pressure due to obesity or other undefined processes [29]. Simultaneously, venous distension reduces CSF absorption across the subarachnoid-venous sinus gradient, resulting in CSF accumulation and, ultimately, intracranial hypertension. Eventually, increased intracranial pressure on a stressed venous system results in venous sinus collapse and stenosis at focal weak points such as the transverse sinuses [29]. Like in SIH, in IIH, the venous sinuses have hypothetically overcompensated, resulting in a state of high craniospinal elastance where small changes in volume result in disproportionate changes in pressure.
Studies support the hypothesis that a state of high craniospinal elastance exists in IIH. Studies measuring the opening and closing opening pressures after CSF volume removal in patients with IIH have shown that IIH is associated with increased craniospinal elastance and decreased PVI and that increased craniospinal elastance is linearly correlated with increased opening pressure [24, 30]. Conversely, to assess SIH, researchers augmented pressure in patients with SIH via intrathecal normal saline [23•]. Although elastance measures in this study were not compared directly to opening pressures, the analysis showed that opening pressures were often normal as opposed to low, as one would expect in SIH [23•, 25]. Higher opening pressures and higher average elastance were significantly associated with cerebral venous sinus distension, pachymeningeal enhancement (micro-venous distension), and the presence of subdural collections in MRI brain imaging but not with signs of caudal brain displacement, further linking compensatory increased intracranial vascular volume with increased elastance [23•].
How does this understanding of craniospinal elastance inform us about the pathophysiology of RIH? In both disorders of IIH and compensated SIH, there seems to be a state of increased craniospinal elastance. In the case of RIH, the symptoms likely stem from the existence of such a state, in which the addition of volume leads to a disintegrating increase in intracranial pressure and clinical symptoms suggestive of a high-pressure headache. Current evidence cannot yet answer the question of why only some patients with SIH develop RIH while others do not. Hypothetically, it is those patients with high craniospinal elastance, such as those with compensated SIH or underlying IIH, who would be predisposed to developing RIH. A study by Schievink et al. (2019) supports the link between changes in venous physiology and RIH, finding that transverse sinus narrowing is associated with a higher chance of RIH [3•]. Using MRV, the study found that a fourth of those with focal narrowing in one transverse sinus and half of those with a complete signal gap in one transverse sinus or any involvement of both transverse sinuses developed RIH [3•].
Variability in RIH onset could occur from variability in an individual’s reserve of the craniospinal elastance system as a whole, with symptoms occurring at the point in which volume shifts resulting from the procedure and/or subsequent healing process and ensuing fibrosis overwhelm an individual’s buffering reserve. Another explanation for variability in onset could be that the craniospinal elastance system is also affected by variations in the compliance of the dura itself, which affects CSF outflow resistance. Those with a high complaint dura and low CSF outflow resistance may not, or to a lesser degree, experience RIH. Others who have developed adhesions, scarring, and/or fibrosis as part of natural or induced dural healing, which results in decreased CSF compliance and increased CSF outflow resistance, may be more vulnerable to RIH [25].
Exploring RIH pathophysiology may also provide insight into the pathophysiology of other primary headache disorders. It is reasonable to theorize that increased craniospinal elastance, potentially mediated by changes in venous physiology, exists in other primary headache disorders [31]. A low reserve to compensate for changes in pressure or volume could explain some phenomena seen in primary headache disorders that otherwise do not have an anatomical explanation, such as primary headache disorders with pain resulting from increases in intrabdominal pressure through Valsalva maneuvers or cough, from increases in cardiovascular output (e.g., through exertion), and from barometric pressure changes.
留言 (0)