In urolithiasis, calcium-containing stones predominate, mainly including calcium oxalate stones and calcium phosphate stones, accounting for more than 70% of all urinary stones; the rest also include uric acid stones, magnesium ammonium phosphate stones, cystine stones and mixed stones, etc. [14]. Previous studies have concluded that knowledge of stone composition is fundamental to the prevention and treatment of urinary tract stones.
Early studies have found that stones can be categorized on the basis of urography (KUB) and computed tomography (CT) imaging findings, varying according to mineral composition [15]. However, this is a rough and vague categorization and the accuracy of the results needs to be improved. The ability of electron computed tomography (CT) to predict stone composition has been studied for decades, and some controversy still exists. Some studies have shown that monoenergetic and dual-energetic computed tomography (CT) possess better discriminatory ability [16]; Takashi Kawahara et al. found that non-contrast computed tomography improved the predictive value of differentiating stone composition from Heinz units (Hu) obtained from CT scans. The HUs in calcium oxalate were significantly higher than those in uric acid (p < 0.01) and struvite (p < 0.01). Those in monohydrate stones were significantly higher, compared with dehydrate stones (p < 0.05). However, a number of factors also tend to influence Hu measurements on non-enhanced computed tomography (NCCT), such as stone size and mixed stone composition, making the prediction inaccurate [17]. Weronika Sofińska-Chmiel et al. demonstrate the utilization of infrared spectroscopy (FTIR), X-ray diffraction (XRD), and electron microscopy with an EDX detector to identify components associated with urinary stones [18]. as well as the rising trend in recent years of building predictive models through deep learning in computers to predict stone composition [19, 20], Many primary care hospitals do not have these conditions and its applicability is still very limited. So we tried a new method, column line drawing, to predict calcium oxalate stones in patients with pre-treatment urinary tract stones.
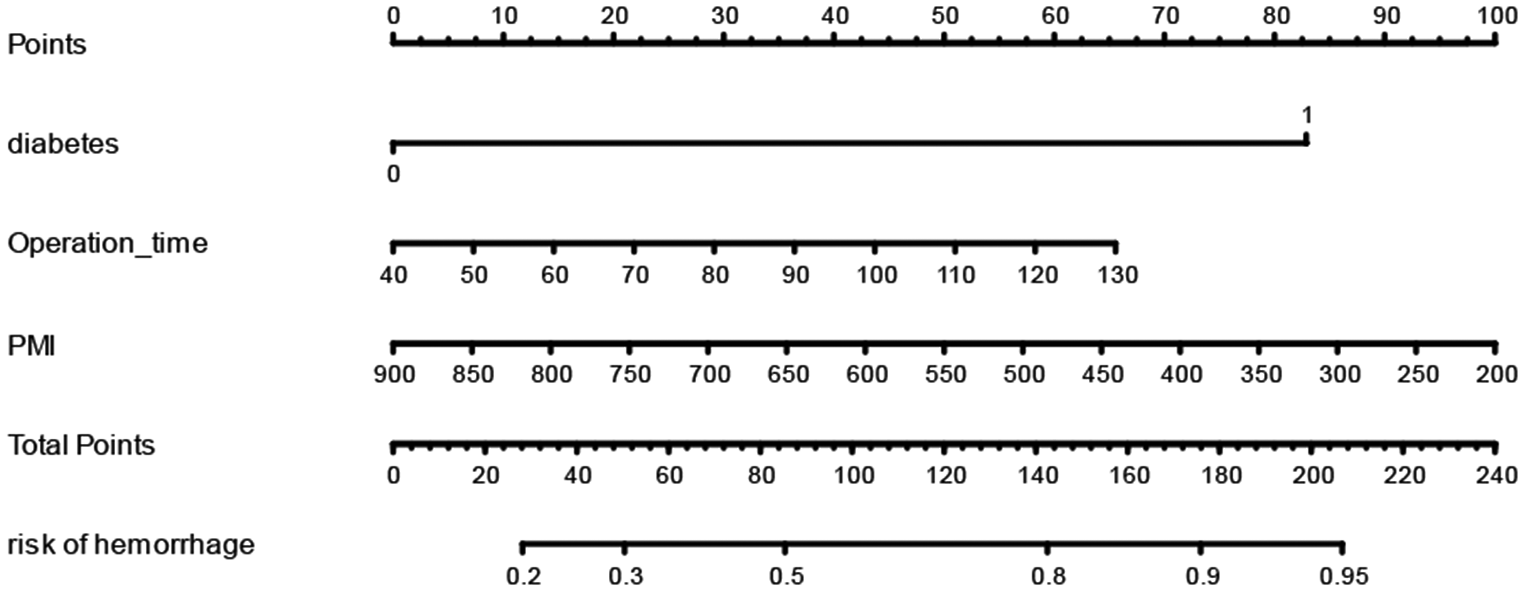
In this study, compared to the traditional serum and 24 h urine tests [21], We conducted a study analyzing the urinary ionic composition of patients pre-surgery, investigating factors such as gender, age, cystatin C, triglycerides, creatine kinase, ionized calcium Ca, ionized magnesium Mg, and citrate ion C6H6O7 that may influence the results. Several nomograms based on urinary calcium, oxalate citrate, and magnesium have been developed in the past by previous authors. However, we have utilized the latest statistical methods relative to previous studies, while adding new variables. This graph effectively distinguishes calcium oxalate stones from other types. The nomogram can help clinicians identify patients at high risk of calcium oxalate stones early on, and involves patients in the diagnosis and treatment decision-making process. Additionally, the nomogram graph can be used in both outpatient and inpatient settings, benefiting resource-limited rural areas in China. It also serves as a simple and effective diagnostic and treatment tool for patients unable to undergo surgery (Fig. 5).
First, similar to previous studies, men were associated with a higher risk, suggesting that men were more likely to develop calcium oxalate stones [22]. This may be related to the nature of men’s occupation: men tend to perform more physical labor and sweat more, leading to supersaturation and precipitation of crystals in the urine. Ahmed M Elshal et al. found that the expression of ARs and miRNA-185-5p was significantly higher in SFGs than in the healthy population by comparing 74 patients with CaOx stones (SFGs) with 40 healthy individuals. However, CSF-1 expression was significantly lower in the stone group than in the healthy subjects. Wei Zhu et al. showed that inhibition of androgen receptor (AR) expression in renal tubular epithelial cells increased macrophage recruitment/M2 polarization, which resulted in enhanced phagocytosis of CaOx crystals in the kidney, confirming that estrogens inhibit the formation of stones more than androgens do in the human body [23, 24].
Secondly, age is another important factor in the formation of urinary stones, especially calcium-containing stones, and the reasons for this are still controversial. Perinpam et al. showed that calcium excretion declines with age [25]. However, the cohort evaluated in this study consisted primarily of non-stone-formers. Triet Vincent M. Tran et al. concluded that calcium excretion in patients with CaOx stones was significantly reduced with decreasing creatinine clearance (CrCl), with a generalized relationship to advancing age [26]. Some studies suggest that stones can take decades to develop. This immediately implies that the stone burden will increase with age.
In addition, this study found that cystatin C, triglycerides, ionized calcium Ca, and citrate ion C6H6O7 could also be important factors as new predictors of calcium oxalate stones.
Mao et al. [27] showed that cystatin C was positively correlated with the degree of hydronephrosis caused by kidney stones. Hyperlipidemia is associated with decreased urinary pH and increased urate excretion, and acidic urine may lead to uric acid stone formation. Elevated uric acid excretion is a risk factor not only for uric acid stone formation but also for CaOx stone formation [28, 29]. Stone formation occurs due to the urine being oversaturated with calcium oxalate and brushite. The level of oversaturation is linked to fluid intake and the quantity of citrate and calcium in the urine. Urinary calcium levels exceeding 200 mg/day elevate the risk of stones and frequently result in a negative calcium balance. Reduced calcium reabsorption by the kidneys is a factor in idiopathic hypercalciuria [30].




留言 (0)