
記住我

Airway obstruction due to bleeding after ear, nose, throat (ENT), or maxillofacial surgery is an important cause of airway morbidity and mortality.1–4 The 4th National Audit Project (NAP4) study from 2011 by Cook et al4 identified several cases of anesthesia-related aspiration of blood, 1 of which was fatal due to a large blood clot causing a complete obstruction. Remaining occult blood in the nasopharynx posterior to the soft palate may cause fatal airway obstruction.5 Such clots are often referred to as “coroner’s clots” in ENT surgery, as it is often retrieved postmortem. Management includes meticulous suctioning under direct laryngoscope vision, performed with a neck flexion to shift the clot more anteriorly and aid removal.
We aim to illustrate how the detection and removal of a blood clot that obscures and obstructs the airway can pose challenges, potentially impede laryngoscopy, and that commonly accessible equipment might not suffice to solve the airway problem.
This case is reported according to the case report (CARE) guidelines6 and written informed consent from the patient is obtained for the publication of this case report.
CASE DESCRIPTIONThe patient is a 48-year-old woman, with a normal body mass index and a medical history of mild asthma. Two weeks prior, the patient underwent bilateral adenotonsillectomy, resection of the base of the tongue, neck dissection, and metastatic lymph node resection due to a squamous cell carcinoma. General anesthesia and airway management were uneventful. She was endotracheally intubated via direct laryngoscopy using a Macintosh blade size 3, with a reported Cormack-Lehane grade 1 (CL1).
She was readmitted for resection of residual pathological tonsillar tissue. The airway assessment revealed a normal neck and a Simplified Airway Risk Index score of 0. The patient underwent general anesthesia, with normal bag-valve-mask ventilation (BVM) and like at the previous surgery, she was endotracheally intubated via direct laryngoscopy using a Macintosh blade size 3, with a reported CL1. The surgery and extubation were uneventful.
One hour after termination of surgery the patient started bleeding from the mouth, causing dyspnea. She was first provided with ice cubes, then tranexamic acid, and dexamethasone was administered intravenously. Epinephrine inhalation was without effect, and she was brought back to the operating room for surgical hemostasis.
An awake intubation of the patient was considered initially. However, she was not cooperative and in severe respiratory distress. This resulted in the decision to utilize nasal oxygenation and to perform a rapid sequence induction. Before induction, the cricothyroid membrane was identified and the availability of specialized equipment and personnel for potential front-of-neck airway access was ensured.
Oxygen was administered at 10 L/min via a nasal cannula. General anesthesia was induced with propofol and succinylcholine, followed by an infusion of propofol and remifentanil. Laryngoscopy was performed using a McGrath Mac videolaryngoscope with a Macintosh blade size 3. There was no obvious ongoing bleeding, but no laryngeal structures could be identified. A senior anesthesiologist repeated the videolaryngoscopy, however with the same result. Intermittent BVM was successfully performed, which ensured adequate oxygenation throughout the airway management, and rocuronium was administered to ensure relaxation. The ENT surgeon then performed a direct laryngoscopy using an anterior commissure laryngoscope but could not identify any laryngeal structures either. An obstructing blood clot was suspected, and suction with a Yankauer-type rigid suction catheter with side holes was attempted unsuccessfully. Mechanical removal with forceps was also unsuccessful.
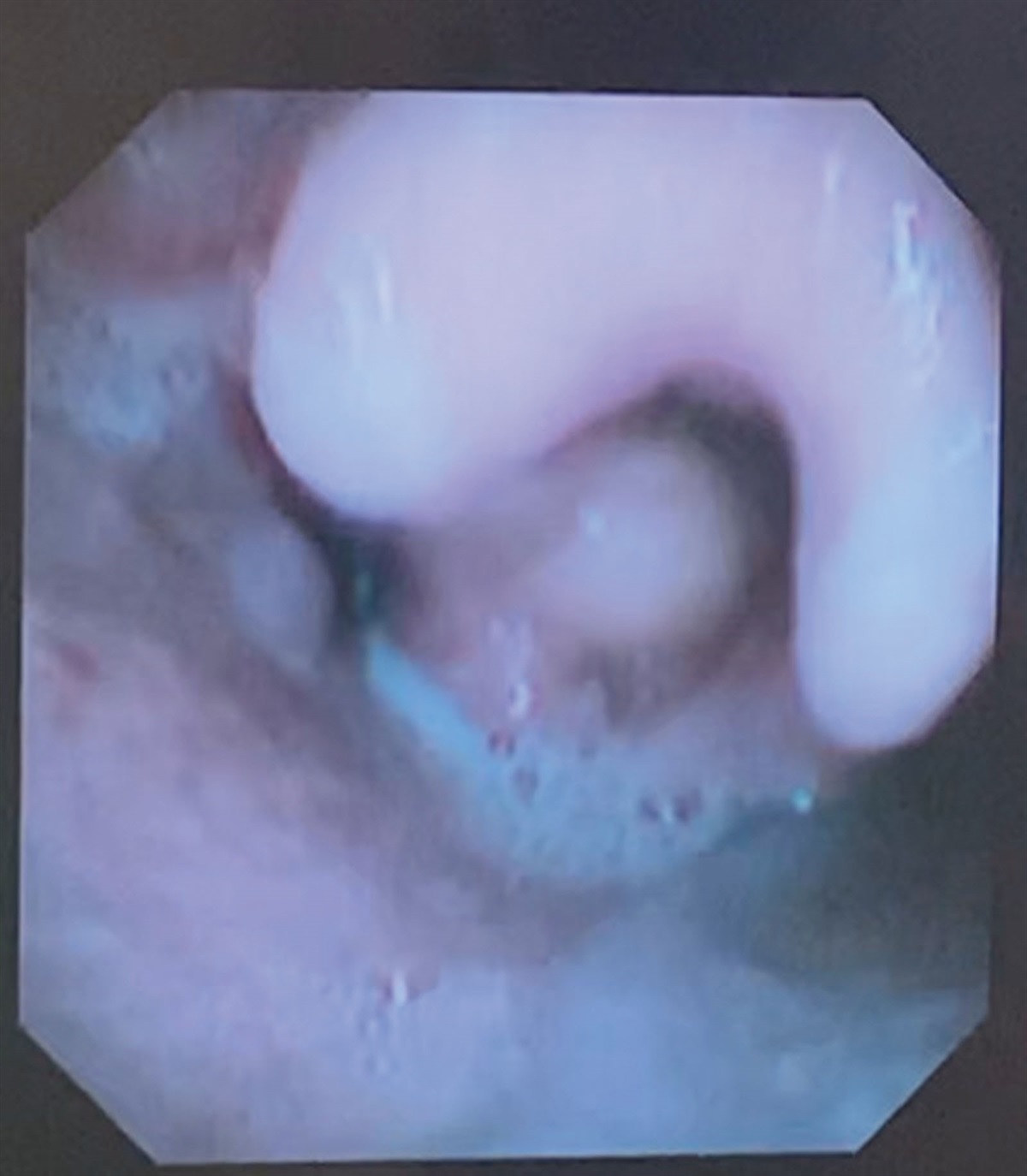
Finally, the surgeon passed a metal suction tube without side holes through the laryngoscope (Figure 1). The suction tube was withdrawn together with a 30-cm-long blood clot, resembling a cast of the esophagus, hypo-, oro-, and nasopharynx (Figure 2). An airway exchange catheter was passed through the laryngoscope, the laryngoscope was removed, and a size 6.0 mm endotracheal tube was passed over the catheter. Smaller blood clots were removed with suctioning and forceps.
 Figure 1.:
Figure 1.: The devices used in our case. From top to bottom: Kleinsasser anterior commissure laryngoscope (Model 8590 Karl Storz), a metal suction device without side holes and a Yankauer suction device.
 Figure 2.:
Figure 2.: The 30 cm blood clot removed from the airway, resembling a cast of the esophagus, hypo-, oro-, and nasopharynx.
Oxygen saturation measured by pulse oximetry was between 93% and 100% during the entire procedure. The end-tidal CO2 readings after the procedure were between 4.3 and 6.6 kPa. However, during the procedure, the capnography waveform exhibited irregularities, questioning the accuracy of the recorded end-tidal CO2 values.
After hemostasis was ensured, tracheal extubation was performed uneventfully and there were no coughing or signs of respiratory distress. Hours later, a routine nasal endoscopy showed no evidence of blood or clots in the larynx or subglottic area of the trachea. A bronchoscopy was not performed. Postoperative management proceeded uneventfully, and the patient was discharged in normal health.
DISCUSSIONSeveral well-established guidelines for managing difficult airways exist,7,8 and operating rooms are often equipped accordingly. This case demonstrates that commonly accessible equipment may prove ineffective for managing blood in the airways.1
Suction is a common technique to facilitate endotracheal intubation and may be critical for success in an airway contaminated with, eg, blood or vomitus. Various catheters are used, and some have safety holes on the sides to prevent damage to the airway.9 The suction pressure of these catheters may be impaired if the safety holes are left unoccluded. As much as 90% reduction has been reported.10,11 A suction catheter of this type––a Yankauer suction catheter––was initially attempted in our case.
Furthermore, guidelines recommend the use of forceps to remove solid material in a soiled airway.8 Hence, these are often readily available in many airway management kits. This was also attempted in this case, but proved ineffective, as only small pieces of the blood clot were torn off.
This case report demonstrates that large-bore suction devices may be required in everyday clinical practice and that the suction pressure is of critical importance. However, the increased suction pressure may be harmful to the airway mucosa,12 therefore an assessment of potential risks and benefits should be made in the individual clinical setting. In our case, the increased suction pressure enabled the resolution of the airway management problem.
Hospitals may not have large-bore suction catheters, which can be problematic, as the readily available equipment was ineffective in our case. As a result, alternative set-ups have been suggested.13 A regular endotracheal tube with the distal end cutoff and the proximal part connected to a surgical suctioning machine has been demonstrated to have superior suction pressure compared to commercial large-bore suction devices.11 In our case, once we identified a blood clot as the issue, we switched from the Yankauer suction catheter with side holes to a metal suction catheter without side holes. This change proved to be effective to solve the problem. If that had not been the case, our next step could have been using an endotracheal tube with a cutoff distal end.
The extracted blood clot in our case extended from the nasopharynx and deep into the esophagus, and the pharyngeal part of the clot obscured the laryngeal structures to such an extent that both the anesthesiologist and the surgeon initially struggled to identify any recognizable laryngeal structures. Nevertheless, the clot must have left an open passage to the trachea since BVM ventilation was possible and sustained oxygenation during the procedure.
In summary, we argue that this case illustrates the insidious nature of a slow but continuous bleeding in a postoperative patient who might be partially obtunded. A gradually forming blood clot may remain asymptomatic until it reaches a critical size, posing a threat to the airways by covering and compressing laryngeal structures. At this point, its size may prohibit the patient from either coughing it out or swallowing it, leading to potential airway compromise. Hence, in airway bleeding, there is a need for larger-bore suction devices with an increased suction pressure. When a blood clot is encountered it may additionally be necessary to use a catheter without side holes, and consequently both should be available in facilities where blood in the airways may occur. While we acknowledge that many anesthesiologists may have encountered similar scenarios, we consider this as an important reminder of the unpredicted formation of blood clots and its management.
DISCLOSURESName: Sandra Ellefsen, MD.
Contribution: This author helped draft the article, and read and accepted the final article.
Name: Michael S. Kristensen, MD.
Contribution: This author helped handle the clinical case, revised the article, and read and accepted the final article.
This manuscript was handled by: Markus M. Luedi, MD, MBA.
REFERENCES 1. Kristensen MS, McGuire B. Managing and securing the bleeding upper airway: a narrative review. Can J Anaesth. 2020;67:128–140. 2. Cook TM, Woodall N, Frerk C; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. Br J Anaesth. 2011;106:617–631. 3. Cook TM, MacDougall-Davis SR. Complications and failure of airway management. Br J Anaesth. 2012;109(suppl 1):i68–i85. 4. Cook TM, Woodall N, Frerk C, editors. Aspiration of gastric contents and of blood. In: 4th National Audit Project (NAP4). The Royal College of Anaesthetists; 2011:155–164. 5. Bangera A. Anaesthesia for adenotonsillectomy: an update. Indian J Anaesth. 2017;61:103–109. 6. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; CARE Group*. The CARE guidelines: consensus-based clinical case reporting guideline development. Glob Adv Health Med. 2013;2:38–43. 7. Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022;136:31–81. 8. Frerk C, Mitchell VS, McNarry AF, et al.; Difficult Airway Society intubation guidelines working group. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015;115:827–848. 9. Lomholt N. Design and function of tracheal suction catheters. Acta Anaesthesiol Scand. 1982;26:1–3. 10. Cox R, Andreae M, Shy B, DuCanto J, Strayer R. Yankauer suction catheters with “safety” vent holes may impair safety in emergent airway management. Am J Emerg Med. 2017;35:1762–1763. 11. Nikolla DA, King B, Heslin A, Carlson JN. Comparison of suction rates between a standard Yankauer, a commercial large-bore suction device, and a makeshift large-bore suction device. J Emerg Med. 2021;61:265–270. 12. Sinha V, Semien G, Fitzgerald BM. Surgical airway suctioning. In: StatPearls. StatPearls Publishing; 2023. Accessed December 8, 2023. http://www.ncbi.nlm.nih.gov/books/NBK448077/. 13. Weingart SD, Bhagwan SD. A novel set-up to allow suctioning during direct endotracheal and fiberoptic intubation. J Clin Anesth. 2011;23:518–519.
留言 (0)