In this study we have readdressed the long-term results after surgical BCC excision in the periocular region. Today surgical BCC excision and in particular MMS is considered the gold standard in BCC treatment, despite a plethora of alternative treatments available, such as cryotherapy, chemotherapy and radiotherapy [2, 9]. Considering an increasing life-expectancy [18] over the last decades associated with increasing numbers of eyelid BCC with increased age, this research question is still topical.
Patient and BCC characteristics are in accordance with our previous report [10]. The majority of patients were between 60 and 80 years old, with a mean age of 72.5 ± 12.8 years. The two most common locations were the lower eyelid and the medial canthus, which is also in line with the literature [19,20,21,22,23,24,25,26]. Greatest linear diameter of the BCC was 5–9 mm in 37.4% or as defined by the AJCC 7 classification 45.5% reached stage T2a. Greatest linear diameter is also in accordance with our previous report where the majority (40.9%) was 5–9 mm in size at initial presentation [10].
The number of nodular BCCs increased from 73% to 86%, whereas sclerosing BCCs decreased from 14% to 9%, yet the frequency distribution did not change compared to our previous report [10]. Hence, a 60–80 year old patient with 5–9 mm lesion at the lower eyelid or medial canthus, with a nodular or sclerosing appearance should lead to a high suspicion for BCC.
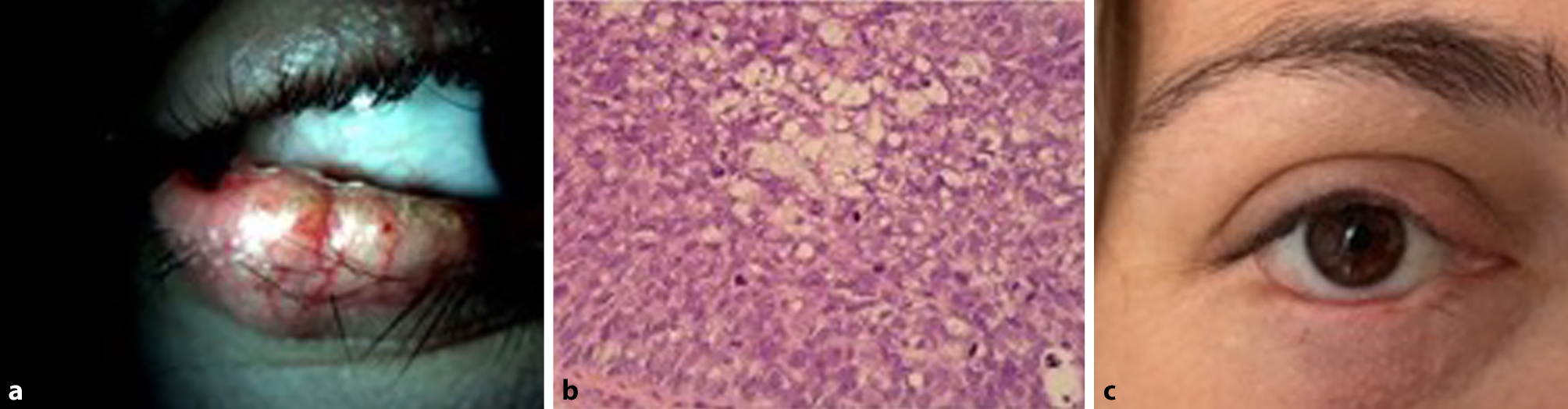
A recurrence rate of 5.0% was observed after a mean follow-up of 3 ± 2 years for the 398 patients whose primary BCC resection was performed at our department. The recurrence rate increases with each additional operation needed. In this study recurrence rates were 9.5% and 42.9% for the third and fourth operation needed, respectively. It is further evident that with every additional operation needed, the distribution regarding BCC location changes from lower eyelid to medial canthus (see Fig. 1a) as the most common site of recurrence. Also, histological types change from nodular to sclerosing BCC as the most common histological BCC type. The relatively high number of nodular BCCs at the timepoint of the first revision surgery may be explained by the number of referrals for excision surgery (see Fig. 1b: referred). Additionally, the number of BCCs with depth extensions increased from 7.3% at primary excision surgery to 19.2%, and 57.1% at the second and third operation, respectively. Finally, from the three patients undergoing a fourth operation, one (33.3%) showed depth extension. These findings are in line with previous reports regarding histological types and location, as well as recurrence rates ranging between 1.5% and 9.2% in the literature [19,20,21,22,23,24,25,26].
Caution is advised when comparing recurrence numbers as surgical techniques and follow-up periods differ vastly. As most BCCs recur within 3 years after treatment and up to one third after 5 years [25, 27], sufficient follow-up time is essential in clinical studies. Filtering studies for surgical approach and follow-up time shows that BCC recurrence rate after MMS is even lower, between 1.5% and 5%. [10, 23, 25, 26, 28,29,30]. Studies with longer follow-up periods (4 and 5 years, respectively) reported marginally higher numbers between 2% and 5% [30, 31] highlighting that 3 years of follow-up to be a valuable follow-up period, which also applies to this study.
The change in primary location of occurrence, histologic type and increase in numbers with depth extension with each consecutive operation performed, may be attributed to the anatomical structures comprising the canalicular system, medial canthal tendons as well as the insertions of the orbital septum, which may lead to cautious BCC and circumferential tissue excision. This has been confirmed in a multicenter study, where oculoplastic surgeons were more likely than plastic surgeons or dermatologists to incompletely excise BCCs, which was attributed to the more difficult case mix regarding location [32]. There is still debate on the ideal size of safety margins. It has been shown that an 8‑mm margin would completely remove 95% of high-risk BCCs [17], which is not possible in most periocular cases. This dilemma is further supported by the finding that in patients with BCCs the mean margin inside the H‑zone was significantly smaller than that outside the H‑zone [17]. Using different sets of instruments for the excision of the tumor, layered tissue segments and reconstruction regarding recurrence have been discussed previously [10] and should be considered a standard procedure. These principles are followed at our institution and may therefore be neglected in this discussion.
The AJCC 7 T stages and histological BCC types only show a very weak to no correlation, both at primary and secondary excision, and do not allow conclusions on suspected type based on size. We used the AJCC 7 T classification as it was available between 2009 and 2019. The current AJCC 8 was established in 2016 [33].
Limitations to be considered are the retrospective nature of this study, the use of AJCC 7 and the limited comparability to other studies due to various follow-up periods, as discussed above. Also, we cannot report the number of resections necessary to get negative margins retrospectively, as patient records are incomplete regarding this specific question.
Previously we have concluded that “In our opinion microscopic control of wound margins ought to become standard practice in the surgical treatment of BCC.” [10], today we can state that with the widespread use of MMS it has become a standard in BCC treatment, especially when it comes to retreatment, with abundant literature supporting its use [2].
In conclusion, we are facing the same challenges in surgical BCC treatment as 30 years ago. The distribution of periocular BCCs and histological subtypes to date mirror the literature und the general consensus. BCC excision at the medial canthus may be challenging, particularly in high-risk cases, such as recurrent sclerosing BCC with deep extensions. In such cases, centers of expertise should be consulted and additional treatment options such as radiation therapy or systemic therapy may be considered.





留言 (0)