
記住我










Background&Aims The role of antibody-mediated rejection (ABMR) after liver transplantation (LT) remains controversial. Chronic ABMR (cABMR) is often subclinical and potentially missed without surveillance biopsies (svLbx) which are not established in most LT centers. Transcriptome analysis previously characterized molecular changes in T cell-mediated rejection (TCMR) after solid organ transplantation. We aimed to identify molecular cABMR signatures after LT for a more comprehensive understanding of cABMR.
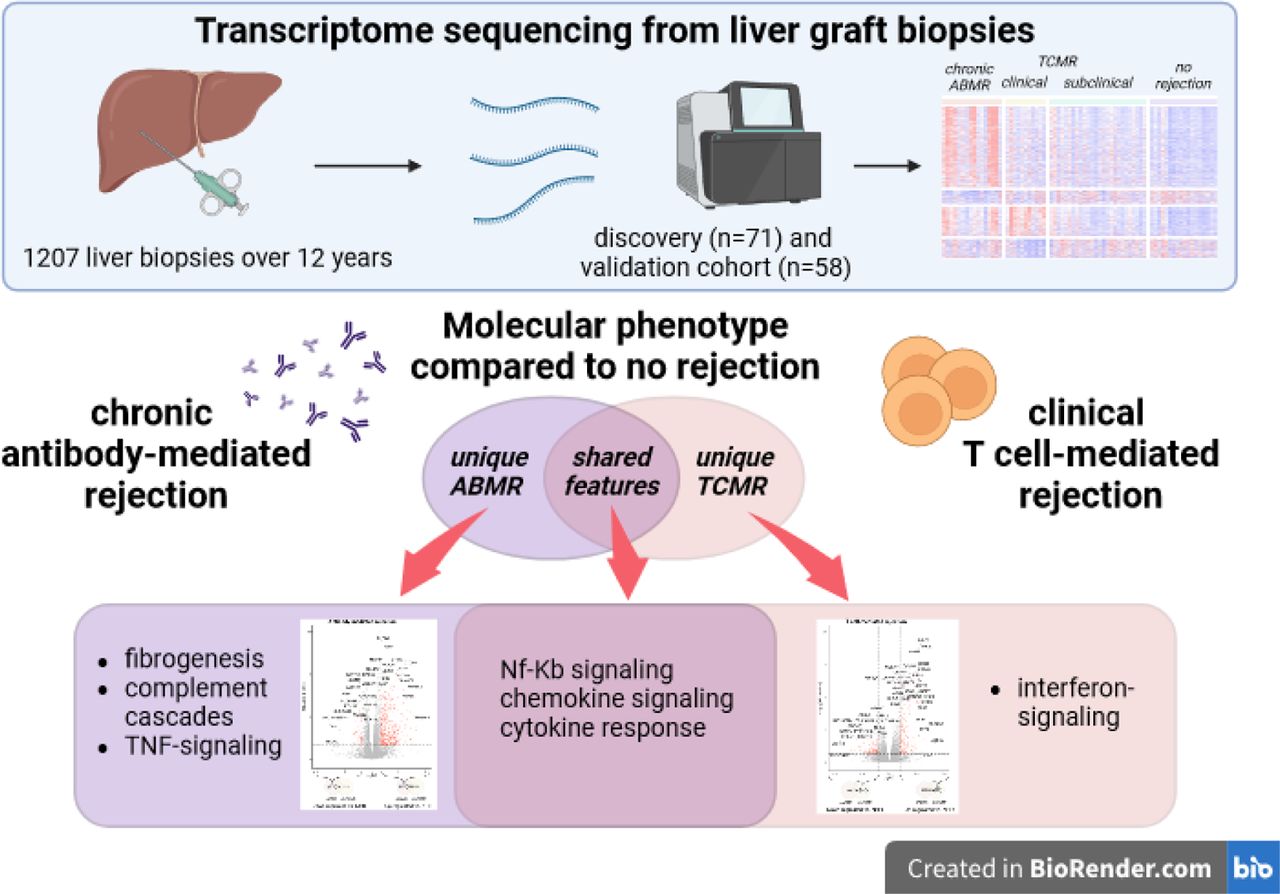
Methods We retrospectively identified indication and svLbx from our prospective institutional biorepository (n=1207 over 12 years). We performed RNA-sequencing on liver biopsies (discovery cohort: n=71; validation cohort: n=58). Downstream analyses explored the unique and common molecular features of cABMR, clinical (clinTCMR) and subclinical TCMR (subTCMR) compared to no histological rejection (NHR).
Results Nineteen percent of LT recipients with donor-specific antibodies had cABMR. Eighty-one percent of patients with cABMR had ALT and AST ≤2x the upper limit of normal, only being recognized by svLbx. The cABMR group displayed differentially expressed genes (DEGs) uniquely enriched in fibrogenesis-, complement activation- and TNFα-signaling-related pathways. ClinTCMR showed DEGs uniquely enriched in antigen presentation-, interferon-signaling-, and T cell receptor-signaling-related pathways. Common cABMR and clinTCMR DEGs were enriched in chemokine-signaling- and cytokine response-related pathways. Gene set enrichment scores of interferon-signaling and extracellular matrix remodeling pathways discriminated cABMR and clinTCMR. Molecular signatures of clinTCMR correlated with histological TCMR-patterns. Molecular cABMR-signatures correlated with lobular graft injury and liver fibrosis scores. The validation cohort consistently showed patterns of DEGs associating cABMR with fibrogenesis- and NF-κB-signaling-related pathways and clinTCMR with interferon-signaling- and adaptive immunity-related pathways. SubTCMR was molecularly almost indistinguishable from NHR.
Conclusions We report transcriptome-unique features of cABMR that is a unique molecular identity associated with inflammation and fibrogenesis.
Impact and Implications
– Antibody-mediated rejection (ABMR) is a recognized relevant cause of graft injury and unfavorable patient outcomes after kidney, heart and lung transplantation but the role of ABMR after liver transplantation (LT) remains controversial. Hence, we aimed to characterize chronic ABMR after LT on a molecular basis to identify unique features.
– Our findings highlight chronic ABMR to be a distinct clinical phenotype of rejection after LT. Furthermore, we demonstrate chronic ABMR to present mostly with normal liver enzymes, therefore only being detected if protocol biopsies are performed for graft monitoring.
– Therefore, our work emphasizes the usage of protocol graft biopsies for the detection of a fibrosis associated phenotype of cABMR. Pending external validation, the molecular signature may be used in the future to discriminate cABMR from graft injury of other causes.
Highlights
– Chronic ABMR was present in up to 1/5 of DSA-positive biopsies and 1/5 of biopsies with advanced fibrosis
– Chronic ABMR and clinically overt TCMR have largely distinct transcriptome patterns with common up-regulated DEGs enriched in pro-inflammatory pathways
– Clinical TCMR is characterized by up-regulated interferon-signaling at the transcriptome level
– Chronic ABMR signatures include up-regulated DEGs enriched in pathways of fibrogenesis, complement cascades, and TNF-signaling
– Common signatures of TCMR and ABMR are enriched in pathways including NF-κB signaling, chemokine signaling and cytokine responses
Competing Interest StatementThe authors have declared no competing interest.
Funding StatementThe work was supported by grants from the German Research Foundation (SFB738 project Z2 to EJ)), the Transplantation Center Project 19 02 and HiLF II from Hannover Medical School (RT) and the Transplantation Center Project ZN3369 from Hannover Medical School/The Ministry of Science and Culture of the State of Lower Saxony (BE). RT was supported by the Core 100 advanced clinician scientist program from Hannover Medical School. BE was supported by the PRACTIS Clinician Scientist program of Hannover Medical School, funded by the German Research Foundation (DFG, ME 3696/3). ACM was supported by the DAAD Research Grants One year grants for doctoral Candidates, 2023/2024 (57645447). KC was supported by the Else Kroener Fresenius Stiftung (KlinStrucMed programme). This work was supported by the Radboud University Medical Centre Hypatia Grant, an ERC Starting Grant, grant agreement 948207 (ModVaccine), the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany's Excellence Strategy EXC 2155 project number 390874280, and the Lower Saxony Center for AI and Causal Methods in Medicine (CAIMed) grant funded by the Ministry of Science and Culture of Lower Saxony with funds from the program zukunft.niedersachsen of the VolkswagenStiftung (all to YL).
Author DeclarationsI confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The study was approved by the local Ethics Committee (protocol number 933 for project Z2 of the comprehensive research center 738; MHH Ethikkommission, Hannover, Germany).
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Yes
Footnotes↵* authors share first authorship
↵+ authors share last authorship
↵11 Biomedical Research in End-stage and Obstructive Lung Disease Hannover (BREATH) of the German Center for Lung Research (DZL), Hannover, Germany
Financial support: The work was supported by grants from the German Research Foundation (SFB738 project Z2; EJ)), the Transplantation Center Project 19_02 and HiLF II from Hannover Medical School (RT) and the Transplantation Center Project ZN3369 from Hannover Medical School/The Ministry of Science and Culture of the State of Lower Saxony (BE). RT was supported by the Core 100 advanced clinician scientist program from Hannover Medical School. BE was supported by the PRACTIS – Clinician Scientist program of Hannover Medical School, funded by the German Research Foundation (DFG, ME 3696/3). ACM was supported by the DAAD Research Grants – One-year grants for doctoral Candidates, 2023/2024 (57645447). KC was supported by the Else Kröner-Fresenius Stiftung (KlinStrucMed programme). This work was supported by the Radboud University Medical Centre Hypatia Grant, an ERC Starting Grant, grant agreement 948207 (ModVaccine), the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany’s Excellence Strategy - EXC 2155 - project number 390874280, and the Lower Saxony Center for AI and Causal Methods in Medicine (CAIMed) grant funded by the Ministry of Science and Culture of Lower Saxony with funds from the program zukunft.niedersachsen of the VolkswagenStiftung (all to YL).
Conflict of interest: Nothing to declare with regard to this manuscript.
Data availability statement: The data that support the plots within this paper and other findings of this study are available from the corresponding author upon reasonable request. The raw gene expression data, including a sample-data relationship file, as well as the count tables are stored conformant with the MINSEQE reporting standard (Version 1.0, June 2012, accessible at https://zenodo.org/doi/10.5281/zenodo.5706411) at MHH RepoMed repository, https://doi.org/10.26068/mhhrpm/20240207-000.
Data AvailabilityThe data that support the plots within this paper and other findings of this study are available from the corresponding author upon reasonable request. The raw gene expression data, including a sample-data relationship file, as well as the count tables are stored conformant with the MINSEQE reporting standard (Version 1.0, June 2012, accessible at https://zenodo.org/doi/10.5281/zenodo.5706411) at MHH RepoMed repository https://doi.org/10.26068/mhhrpm/20240207-000.
AbbreviationsABMRantibody-mediated rejectioncABMRchronic antibody-mediated rejectionCsAcyclosporine AclinTCMRclinically overt T cell-mediated rejectionDEGsdifferentially expressed genesDSAdonor-specific anti-HLA antibodiesFDRfalse-discovery rateFFPEformalin-fixed paraffin-embeddedKTkidney transplantationLAFliver allograft fibrosisLBxliver graft biopsyLTliver transplantationLTRliver transplant recipientNHRno histological rejectionmHAImodified histological activity indexRAIrejection activity indexRINRNA integrity numberSOTsolid organ transplantationsubTCMRsubclinical T cell-mediated rejectionsvLBxsurveillance liver graft biopsiesTACtacrolimusTCMRT cell-mediated rejectionULNupper limit of normalx ULNtimes the upper limit of normal.
留言 (0)