
記住我



The local ethics committee approved the study (Necmettin Erbakan University ethics committee 167/2023).
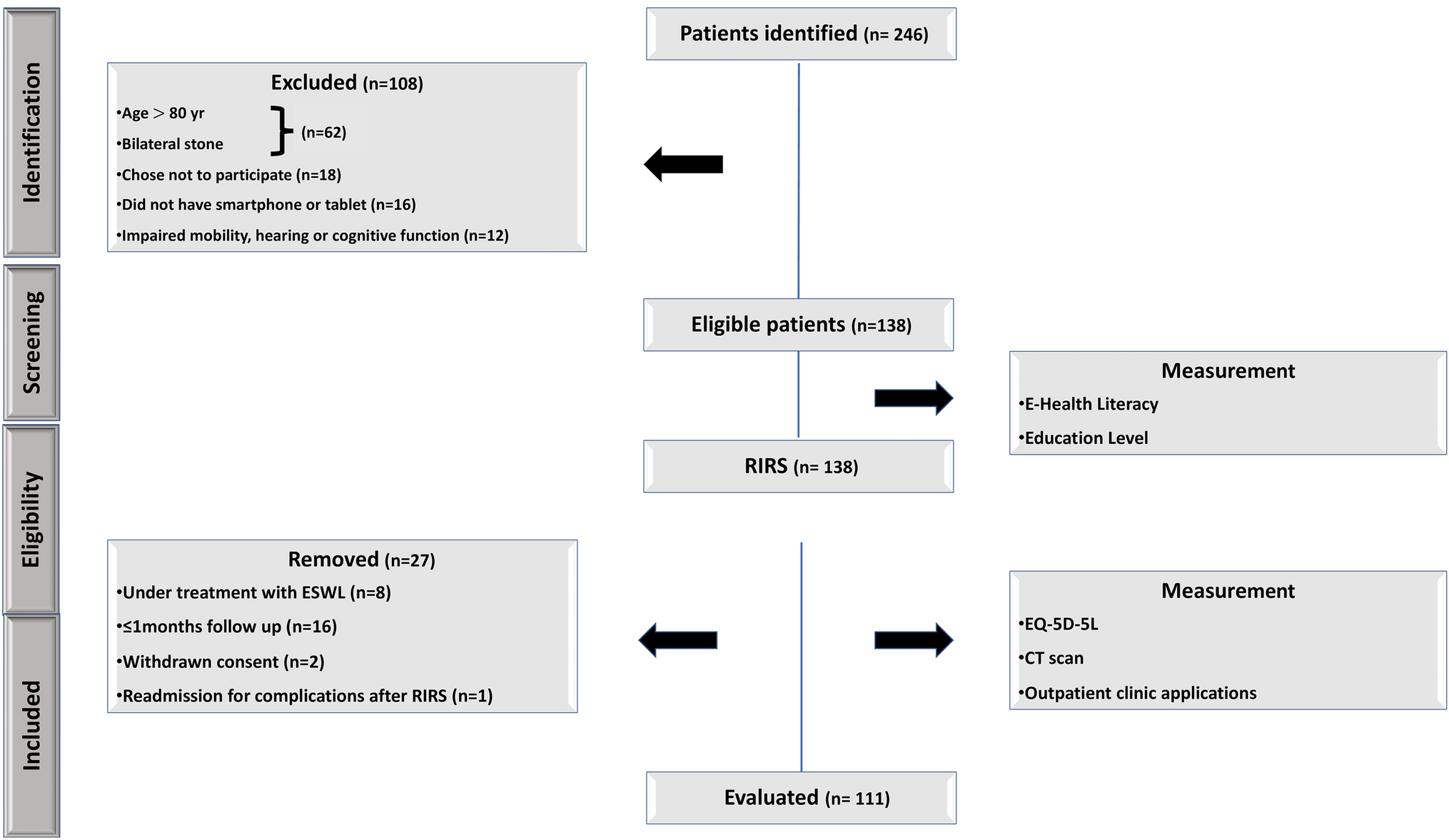
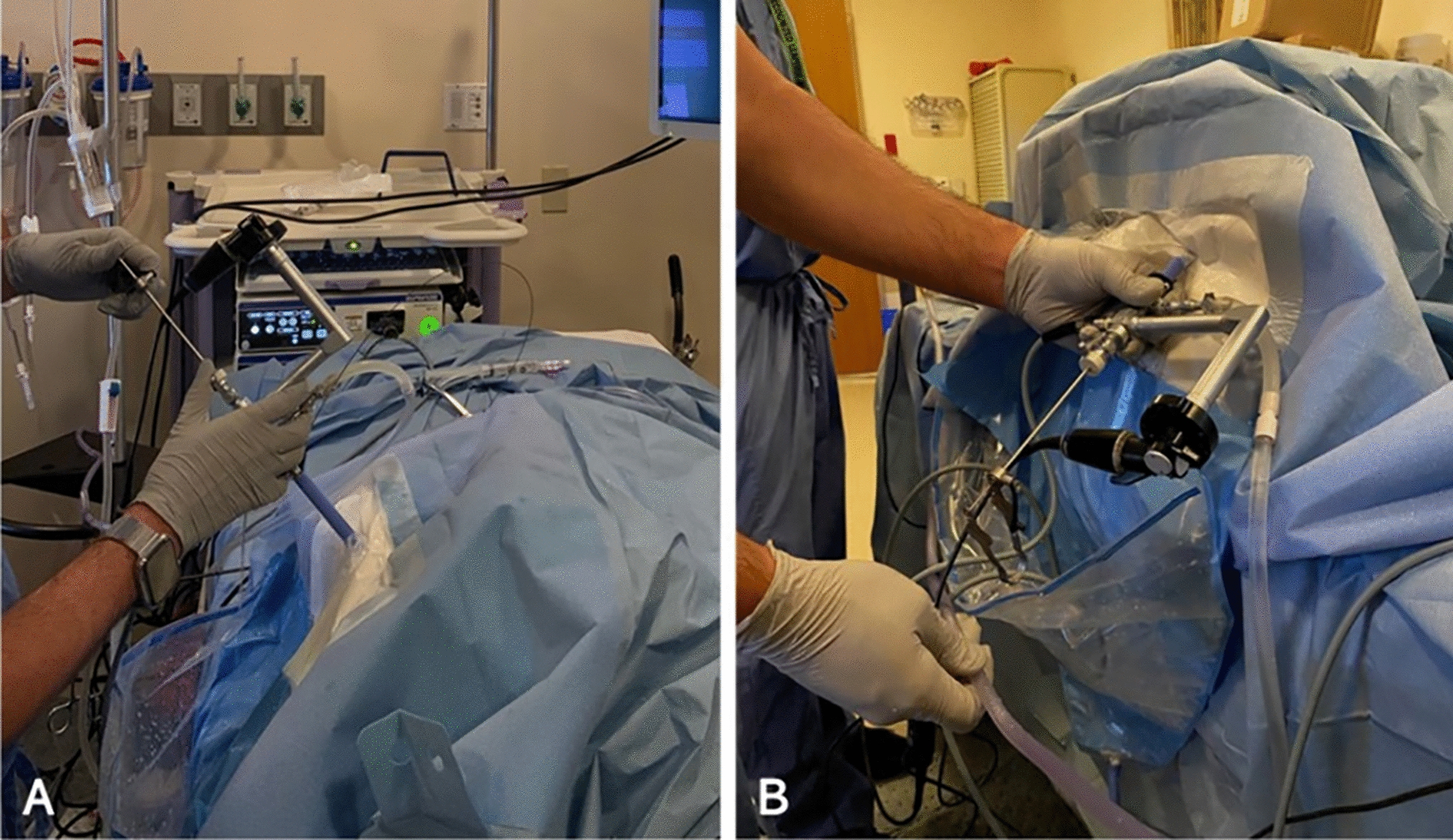
Type of studyThis is an observational, retrospective, comparative, multicentric study of prospectively organised database. A total of 217 patients who underwent RIRS for kidney stones smaller than 2 cm between 01 June 2021 and 1 September 2022 in 3 different centers were included in the study. The patients were divided into two groups; LPL used (Group1, n:121 patients) and HPL used (Group2, n:96). Propensity score matching was done in the data analysis part. After matching, a total of 192 patients, 96 patients in both groups, were evaluated (Fig. 1).
Fig. 1
Flowchart of patient selection
An informed consent form was obtained from all patients before the study. Stone characteristics, duration of surgery, Ho: YAG laser energy settings, postoperative complications, and stone-free status in preoperative non-contrast computed tomography (CT) imaging were recorded.
Inclusion exclusion criteriaPatients between the ages of 18–70 years, with kidney stones smaller than 2 cm and who underwent RIRS for kidney stones were included in the study. Patients younger than 18 years of age and older than 70 years of age, with anatomical anomalies, who had undergone ESWL before, who did not have a preoperative CT scan, whose urine culture was positive, and who did not come for follow-up at the fourth postoperative week were excluded from the study.
Devices and settingsFlex-Xc, Flex-X2s (Karl Storz, Germany) and HU-32 (Huge-med, China) flexible ureterorenoscope were used at the first Center; Flex-X2S (Karl Storz, Germany) and LithoVue (Boston Scientific, USA) in the second center; Flex-Xc, Flex-X2s (Karl Storz, Germany), Wiscope (OTU Medical) and LithoVue(Boston Scientific, USA)in the third center.
For LPL: 272 μ fiber with lasers, Dornier 30 W (Germany) in the first and second center; and 200 μ fiber with Lumenis VersaPuls P20H (Yokneam, Israel) was used in the third center. 272 μ fiber was used with HPL in the first and second center with Jenna Surgical 150 W (Germany); and 200 μ fiber with Quanta Litho Cyber Ho 150 W in the third center (Samarate, Italy).
Surgical tecnique and processAll surgical procedures were performed by experienced endourologists. The procedure was performed in the lithotomy position under general anesthesia. A safety guide wire was placed in the kidney under fluoroscopic guidance. All patients underwent ureterorenoscopy with a rigid ureterorenoscope. A second guidewire was placed during ureterorenoscopy.
In patients who used UAS, UAS was advanced over the second guide wire. In patients who did not use UAS, flexible URS was advanced directly to the kidney over the second guidewire. After reaching the stone, the stone was fragmented with the Holmium:YAG laser.
UAS was used according to the surgeon’s preference. The procedure was performed without sheath in patients whose UAS could not be placed. If the procedure could not be performed without UAS, a DJ stent was placed and tried again 1 month later. The procedure was performed after treatment in patients with a positive preoperative urine culture.
According to each departmental regulation, the Double J stent was removed 2–4 weeks after surgery. SFR was defined as the absence of fragments of any size in X-ray and USG performed at four weeks postoperatively.
Outcome measureThe primary outcome measure was stone-free rate determined by standard care imaging at three months. Intraoperative and postoperative complications, operative time, hospitalization time, and postoperative analgesia were secondary outcome measures. Amount of the energy Joule and frequency used for fragmentation during the procedure, operation time from the start to the end of the procedure in minutes, hospitalization time from the end of the procedure to the discharge in days, and fluoroscopy time (FT) from the beginning to the end of the procedure is stated in minutes as secondary outcome measures.
Statistical analysisStatistical analysis was performed with SPSS 25.0 (Statistical Package). Categorical variables are described by frequencies and percentages. Continuous variables are presented as mean and standard deviations. Independent T, Kruskal–Wallis and Chi-square (χ2) tests were used to compare the relationship between categorical and continuous variables subgroups. A P value below 0.05 was considered statistically significant. Propensity Score matching was used to homogenize the groups in the study.
留言 (0)