
記住我



To investigate the feasibility of aPNL, we first utilized 20 porcine kidneys to establish 20 F percutaneous renal tracts through the dorsal mid calyces. Next, we used flexible cystoscope and flexible ureteroscope to visualize the upper, middle, and lower calyces of the kidney, respectively, and compared the proportion of these calyces that could be visualized by cystoscope or ureteroscope. The experimental procedures are presented in the accompanying video (Supplementary Video S1). In addition, we modeled the kidney in equal proportions to the normal kidney structure. Subsequently, the renal calyces were observed by flexible ureteroscope and flexible cystoscope, respectively (Supplementary Video S2). The results of model experiment were used to assess potential strengths and efficacy of flexible ureteroscope.
Study design and populationTo test the efficacy of sPNL and aPNL procedures, a single-center prospective randomized controlled study was conducted in the Second Hospital of Tianjin Medical University. This trial has been registered at www.chictr.org.cn as ChiCTR2300073822. All surgery procedures were performed by an experienced surgeon with over 500 retrograde intrarenal surgery (RIRS) and PNL cases. The study was approved by the Institutional Ethics Committee of the Second Hospital of Tianjin Medical University (IEC: 43/2020), and informed consent was obtained from each patient upon admission. The study was conducted in accordance with the Declaration of Helsinki.
The primary endpoint was the SFR, and the secondary endpoints included staged surgery rate, operative time, percutaneous tract number, hemoglobin drop, postoperative hospitalization, and postoperative complication. The sample size was determined based on our historical data of the SFR after sPNL and aPNL for staghorn stone (45.7% and 68.3%, respectively). The sample size of 72 per group was calculated using PASS software, with 80% power (1 − β) and a type-1 error (α) of 0.05. However, the sample size was increased to 80 per group to account for a 10% dropout rate.
From October 2020 to October 2022, a total of 160 patients were recruited at the hospital for the clinical trial. Inclusion criteria were as follows: (1) aged 18-year-old or above; (2) presence of staghorn stone confirmed by non-contrast computed tomography (CT) examination; (3) American Society of Anesthesiology scores of 1–2. Exclusion criteria were as follows: (1) patients with solitary kidney, congenital anomalies (such as horseshoe kidney and ectopic kidney); (2) patients with severe preoperative pyelonephritis; (3) patients with intention towards a specific treatment approach. Eligible patients were randomly assigned to the sPNL or aPNL group with a 1:1 ratio using a computer-generated random table. Preoperatively, all patients underwent urine culture and sensitivity. Patients with urinary tract infections were treated with culture-specific antibiotics until the repeat urine culture was negative, and patients with negative urine cultures received second-generation intravenous cephalosporins during anesthesia.
Surgical procedureMore detailed routine surgical steps were described in our previous reports [21, 22]. In the present study, all procedures were performed under general anesthesia. After retrograde insertion of a 5 F ureteral catheter into the renal pelvis, the patient was changed to a prone position. Then, a 17.5-gauge coaxial needle (uroVision GmbH) was inserted into the targeted calyx with the guidance of ultrasound. The tract was dilated stepwise up to 18 F or 24 F using a serial fascial dilator (uroVision GmbH) and a same-sized peel-away sheath was then placed. Stone fragmentation and clearance were performed using pneumatic, holmium: YAG laser, ultrasonic, or combined lithotripsy equipment under the supervision of an 8/9.8 F rigid ureteroscope or 20.8 F nephroscope (Richard Wolf).
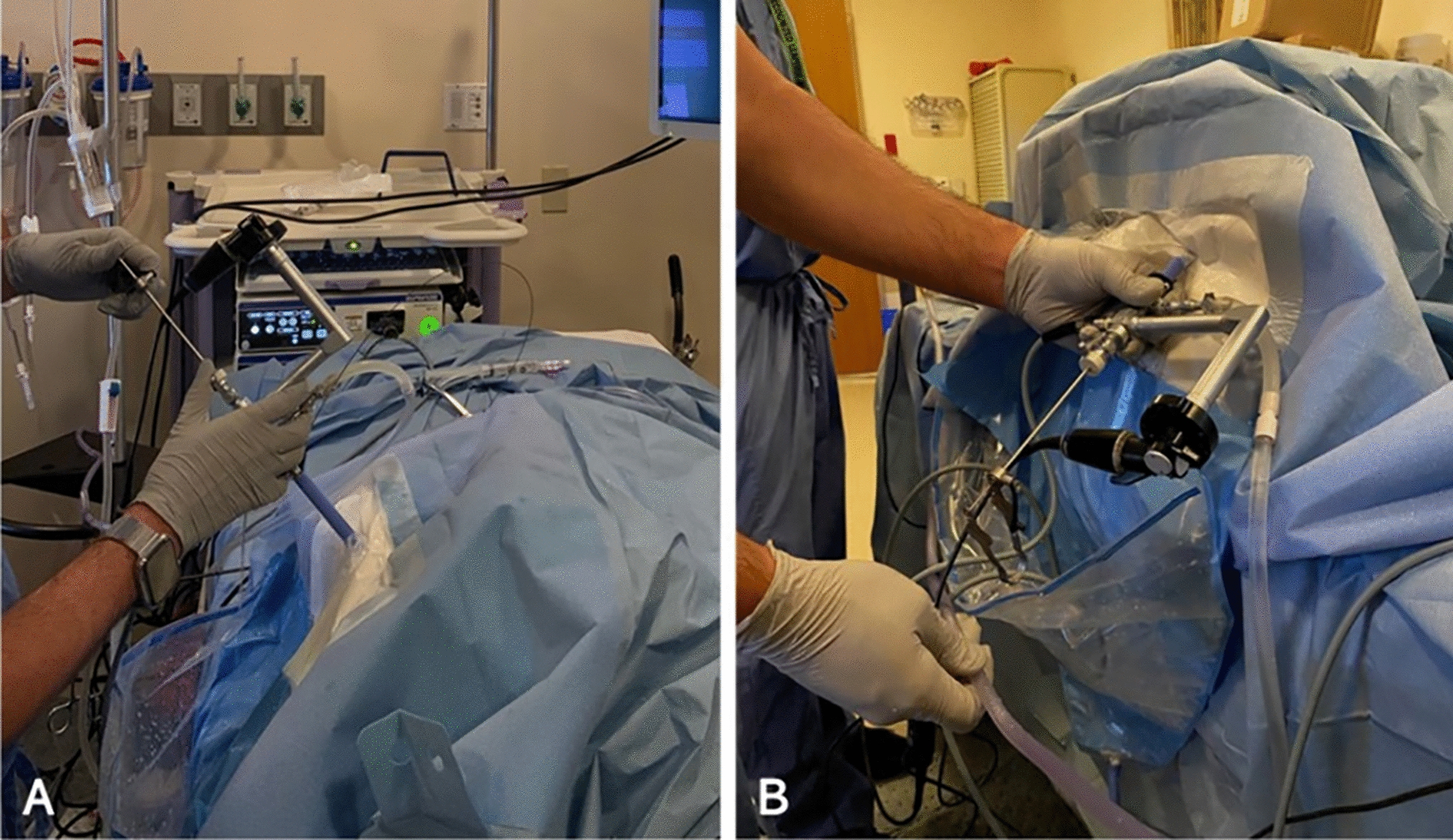
Ultrasound was routinely used to check for residual stones at the later stage of the procedure. For sPNL, additional assisted percutaneous renal tracts were established using a similar method if residual stones could not be reached through the initial percutaneous tract. For aPNL, we firstly attempted to use the flexible ureteroscope (AnQIng® Innovex) through the initial middle tract to disintegrate the residual stones into fragments under direct visualization. The high energy setting of the holmium laser was applied to fragment residual stones as far as possible. The stone fragments were then removed by stone basket or washed out through the sheath by irrigation directly. For the residual stone located in the lower calyx or difficult to be fragmented directly, a stone basket was used to translocate into the renal pelvis, where the rigid ureteroscope could reach. If routine ultrasound during the procedure still revealed residual stones, which neither rigid ureteroscope nor flexible ureteroscope could reach, then the second assisted tract was established to remove the stones. In order to further improve the SFR and avoid missing observation of any calyx, we designed the Tianjin Institute of Urology (TJIU) technique, in which the surgeon observed each calyx in a specific order, namely the upper (Fig. 1A), lower (Fig. 1B), parallel calyx (Fig. 1C, D) and the whole ureter (Fig. 1E) using flexible ureteroscope. When flexible ureteroscopy still revealed residual stones, we would disintegrate the stones through the initial or second tract firstly. If the flexible ureteroscope could not reach the residual stones through the initial or second tract, the third assisted tract would be established. We then used the established tracts to disintegrate the residual stones and repeated the above surgical procedures until no residual stone was identified. Additional assisted tracts would be established if needed.
Fig. 1
Flexible ureteroscopy and management of residual stones using Tianjin Institute of Urology (TJIU) technique at the end of the lithotripsy procedure: A Flexible ureteroscopy of upper calyx. B Flexible ureteroscopy of lower calyx. C, D Flexible ureteroscopy of parallel calyx and management of residual stones. E Flexible ureteroscopy of ureter and bladder
Finally, in addition to residual stones, we would routinely check for any blood clots or bleeding after lithotripsy. Then, a 6 F double-J stent was placed antegrade into the ureter, and one or more 14 F nephrostomy tubes were inserted in all patients.
The surgical procedures are presented in the accompanying video (Supplementary Video S3).
EvaluationUrological CT is typically performed on the second postoperative day to evaluate the SFR (stone-free rate with no residual fragments larger than 4 mm). Operative time is defined as the time from the beginning of the puncture to the completion of the last nephrostomy tube placement. Hemoglobin decrease was calculated as the difference between the preoperative level and the level 24 h postoperatively. Postoperative complications were classified according to the Clavien–Dindo grading system. Fever was defined as a body temperature higher than 38.5 ℃. In addition, patient and stone characteristics, the number of intraoperative percutaneous tracts, and the proportion of staged surgery were recorded for both groups.
Indication and methods of staged surgeryPatients with residual fragments larger than 4 mm would be suggested to undergo additional procedures to attain stone-free status. In consultation with the patient’s preferences, the staged surgery methods consisted of PNL (combined with antegrade flexible ureteroscopy when required) using the same percutaneous renal tract in the primary surgery, retrograde intrarenal surgery (RIRS), or SWL, determined by the stone size and location.
Subgroup analysisOur previous study [21] demonstrated that when the number of stone branches was five or more, there was an increased probability of multiple percutaneous tracts, staged surgery, and longer postoperative hospital stays, while the stone-free rate (SFR) decreased. Therefore, we divided patients into Group 1 (stone branch number < 5) and Group 2 (stone branch number ≥ 5) and further analyzed the differences between the two subgroups.
Statistical analysisStatistical analysis was conducted using R × 64 4.1.2 statistical software. Continuous variables are presented as mean ± standard deviation (SD), while categorical variables are presented as numbers or percentages. Student’s t-test, Chi-square tests, and Fisher’s exact tests were used as necessary. P value less than 0.05 was considered statistically significant.
留言 (0)