
記住我


A 32-year-old male was admitted under intubation for fulminant myocarditis. A transthoracic echocardiogram (TTE) revealed a left ventricular ejection fraction (LVEF) of 32% and an unexpected mass-like lesion in the ascending aorta on the parasternal long-axis (LAX) (Fig. 1A) and the parasternal short-axis (SAX) views (Fig. 1B) (Supplementary videos 1, 2). The mass-like lesion was approximately 20 mm and appeared to float along with the heartbeat. We performed an electrocardiography-gated contrast-enhanced computed tomography (CT) scan instead of transesophageal echocardiography to evaluate the mass and coronary arteries simultaneously. The CT showed no abnormal lesion in the ascending aorta (Fig. 1C) and no coronary artery stenosis, but remarkable fatty connective tissue between the ascending aorta and the right ventricle (Fig. 1D). Because the mass-like lesion reappeared on TTE after CT, it was diagnosed as an artifact. His cardiac function gradually recovered, and he was successfully extubated. His LVEF improved to 52% and he was discharged on day 18. Repeat TTE five months after discharge showed the mass-like lesion again with good cardiac function (Supplementary videos 3, 4).
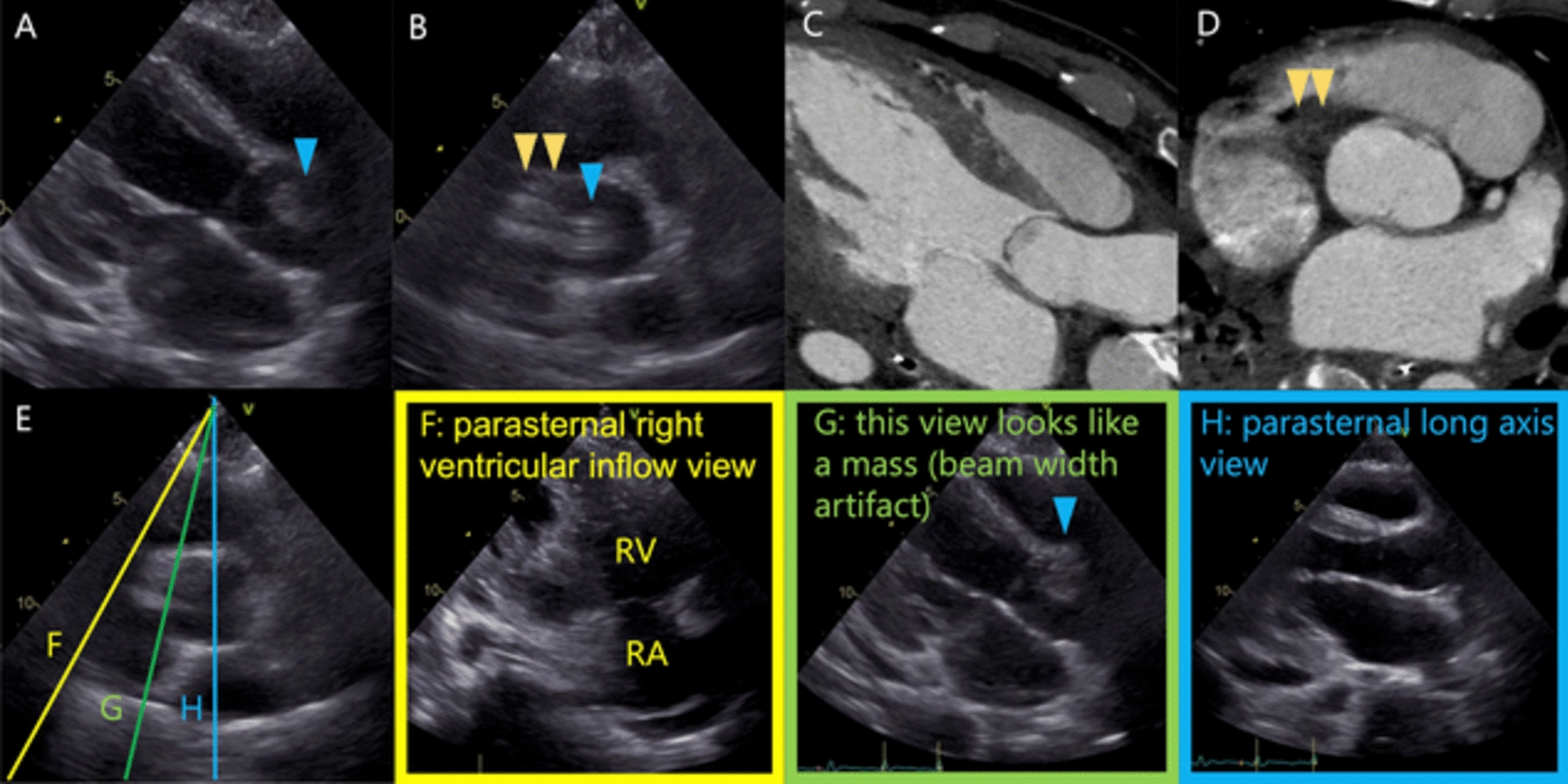
Fig. 1
The long-axis (A) and short-axis (B) views on transthoracic echocardiogram. Contrast-enhanced computed tomography revealing no abnormal lesion in the ascending aorta (C) but fatty connective tissue (D). E The short-axis view corresponding to F–H. F Parasternal right ventricular inflow view. G Beam width artifact. H The long-axis view. Blue and yellow arrowheads indicate mass-like lesion and fatty connective tissue, respectively. RA right atrium, RV right ventricle
Our case showed fatty connective tissues on CT, which was highly echoic on the echocardiogram. We considered this highly echoing connective tissue was reflected in the ascending aorta as a mass-like lesion by the side lobe artifact in the SAX view and the beam width artifact in the LAX view. Side lobe artifact occurs when the side lobe energy is reflected by a strong reflector in its path and these reflections are interpreted by the scanner as originating from the central beam. On the contrary, beam width artifact is the phenomenon whereby objects out of the imaging plane but within the elevation width of the beam are interpreted as being located in the imaging plane [1]. In our case, in the SAX view, the connective tissue outside the aorta and the intra-aortic mass-like lesion is continuous, suggesting a side lobe artifact. The lesion was also observed when the probe was tilted toward the right ventricle from the standard LAX view (Fig. 1E–H). When the probe was tilted further, the lesion was continuous with the connective tissue of the tricuspid valve attachment, and it was reflected as beam width artifact. If an artifact is suspected on TTE, observation in multiple views is recommended [2]. However, our patient was in the supine position due to intubation, and detailed examination was difficult. Furthermore, our case was noteworthy because the mass-like lesion was observed in multiple views by other types of artifacts. Physicians should be aware of the possibility of multiple artifacts, such as side lobe artifact and beam width artifact, occurring simultaneously.
留言 (0)