
記住我

The incidence of stridor, which typically indicates airway obstruction, is especially concerning after emergence from anesthesia. Upper airway obstruction can result from various causes, including a drug allergy, residual muscle paralysis, secretions, blood, and surgical complications. One such cause of stridor, which has been reported in several case studies, is paradoxical vocal cord motion disorder (PVCMD).1–9 PVCMD is an upper airway obstruction associated with the paradoxical adduction or closure of the vocal folds primarily during inhalation but sometimes during exhalation. All previously reported cases described single events.
Written authorization for us to publish the case was obtained from the patient in accordance with the Health Insurance Portability and Accountability Act.
CASE REPORTEpisode 1: A 62-year-old woman was scheduled to undergo a left arthroscopic distal clavicle resection and subacromial decompression for a partial tear in her left shoulder rotator cuff. The patient had a history of diabetes mellitus type 2, hypertension, hyperlipidemia, acquired hypothyroidism, gastroesophageal reflux disease (GERD), and obstructive sleep apnea. The patient weighed 76 kg and had a body mass index of 30.1 kg/m2. In the preoperative area, a left interscalene block was performed with 20 mL of 0.5% ropivacaine. After the induction of general anesthesia, using 4 mg midazolam, 100 µg fentanyl, 100 mg lidocaine, 180 mg propofol, and 50 mg rocuronium, intubation was performed using a 7.0 standard endotracheal tube. Desflurane was used for maintenance. Rocuronium was reversed using 200 mg sugammadex, and the train of 4 improved from 2/4 to 4/4. Other details, such as her mental status, or whether the airway was suctioned, were not documented in the chart. The patient was brought to the postanesthesia care unit (PACU) but developed stridor 50 minutes after extubation with saturation of peripheral oxygen (Spo2) of 99%. Reintubation was performed in a few minutes. No upper airway abnormality was detected during reintubation, and the patient was subsequently transferred to the intensive care unit (ICU). The patient was extubated the following morning. However, expiratory stridor recurred. An otolaryngological examination revealed minor ecchymosis of the nasopharynx. A computed tomography (CT) of the neck, which was performed to rule out subglottic issues, revealed only lung consolidation, possibly due to aspiration pneumonia. Although the stridor disappeared the following day, the patient remained in the ICU for 5 days due to hypoxia of unknown origin.
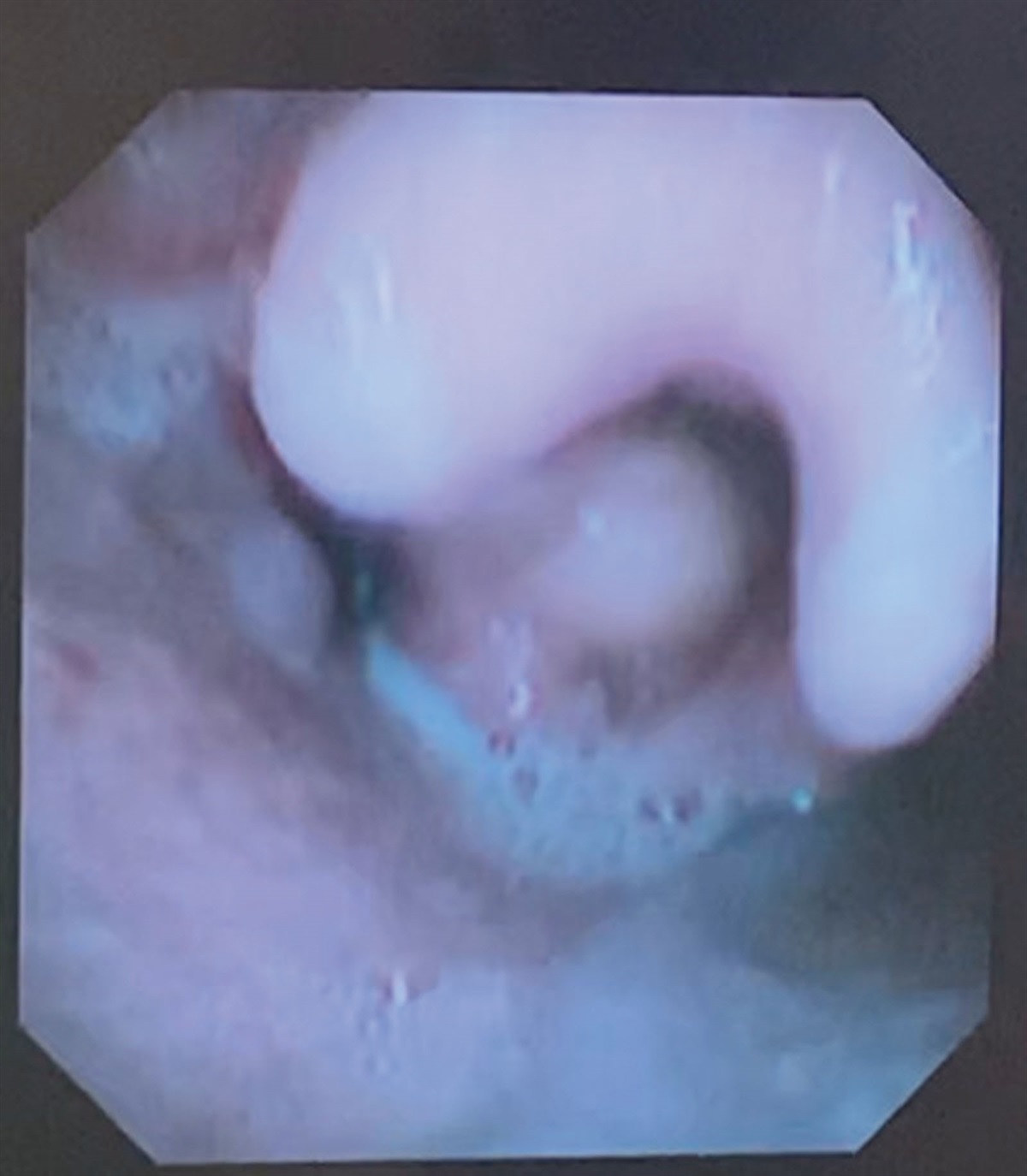
Episode 2: The patient underwent left ulnar nerve decompression for cubital tunnel syndrome 13 months after the first episode of PVCMD at a different hospital. After the induction of general anesthesia, using 2 mg midazolam, 50 µg fentanyl, 80 mg lidocaine, and 130 mg propofol, a supraglottic airway was placed to facilitate spontaneous breathing, which was removed after the surgery. However, the patient developed expiratory stridor a few minutes later with a blood pressure 180/75 mm Hg and heart rate 100–120 bpm. The Spo2 was maintained within a normal range, but the patient had profound perspiration and facial congestion. Although the patient appeared drowsy, she was able to follow verbal commands. A nasal laryngeal examination revealed no evidence of trauma, edema, secretions, or blood. Both vocal cords opened well during inspiration but closed completely at the end of expiration (Video). An otolaryngologist suggested the diagnosis of PVCMD after reviewing the video. Since the patient was almost completely conscious and oxygenation was maintained, no further treatment was recommended other than reassuring the patient. The patient was assured that there were no anatomical issues and that the stridor would disappear as she became more alert. In the PACU, the patient began to breathe normally after 20 minutes. The patient requested to be observed overnight in the hospital and was discharged the next morning after an uneventful night.
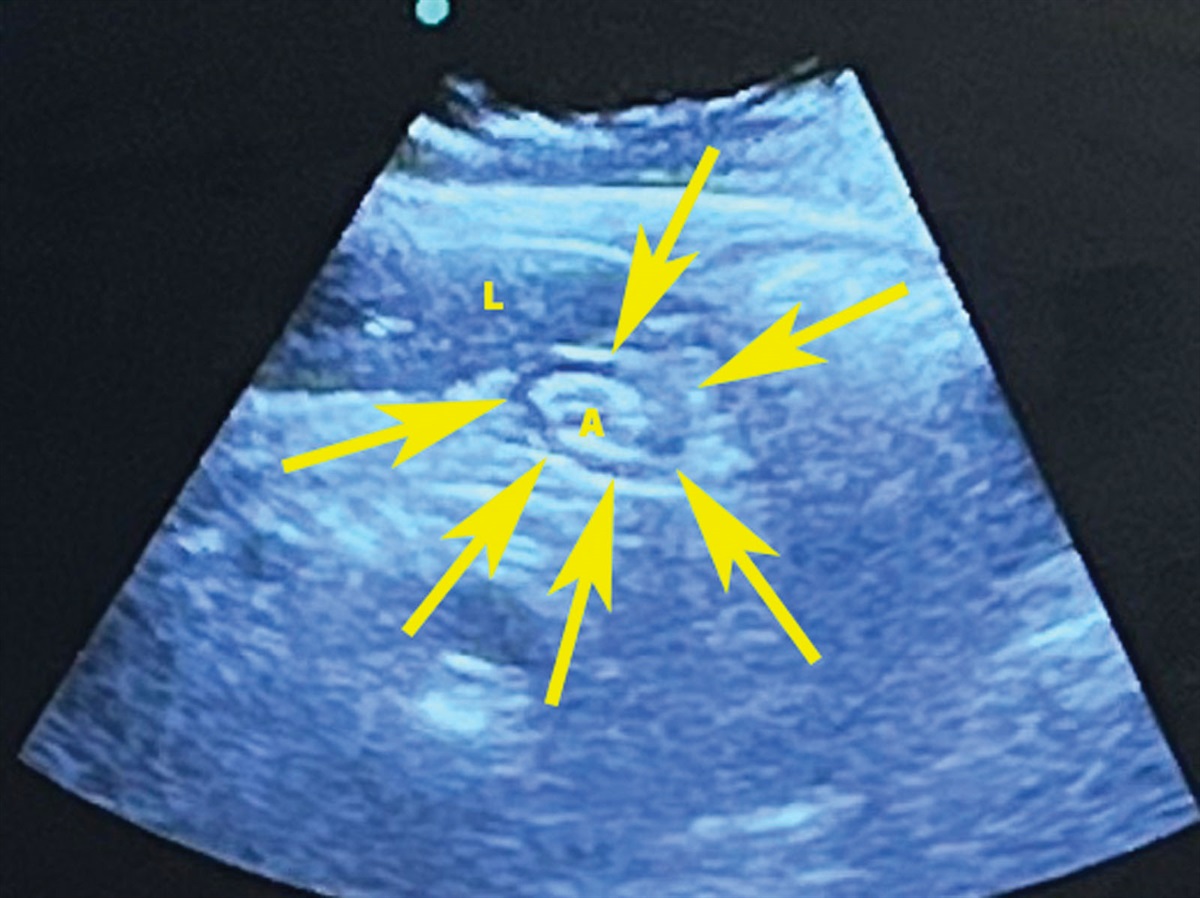
,,]}Episode 3: Twenty months after the first surgery, the patient underwent a C3–4 anterior cervical discectomy with central and foraminal decompression plus C3–4 anterior interbody fusion at the first hospital. Before the surgery, the anesthesia and surgical teams were informed of the patient’s history of PVCMD. General anesthesia was induced using 2 mg midazolam, 60 mg lidocaine, 100 µg fentanyl, 200 mg propofol, and 80 mg rocuronium, and the airway was secured using a 7.0 endotracheal tube. The surgery lasted 2.5 hours. The patient was extubated shortly after 200 mg sugammadex was administered. The train of four was 4/4. Mental status before extubation was not documented. However, ventilatory distress was noted 30 minutes after extubation in the PACU with Spo2 of 97%. The surgical team ruled out a cervical hematoma. Although no audible stridor was detected, 0.5 mg lorazepam, 50 µg fentanyl, and 16 µg dexmedetomidine were administered by an anesthesia provider. The patient appeared comfortable 45 minutes after the treatment and was transferred to the ward as the patient was breathing normally. At 5:05 am on postoperative day (POD) 1 the patient woke up with shortness of breath (SOB), a red face, systolic blood pressure of 160 mm Hg, and Spo2 of 100%. The rapid response team (RRT) observed that the patient was making a “choking noise” and epinephrine, dexamethasone, and diphenhydramine were administered to treat a suspected allergic reaction. The patient did not respond to the treatment and became obtunded and completely unresponsive 30 minutes after the treatment. The Spo2 was maintained above 97%. The patient was intubated using a video laryngoscope after administration of propofol. No airway abnormality was noticed. Given the patient’s known history of PVCMD and a negative neck CT scan, which was done at 6:47 am on POD 1, she was extubated later that morning. A postextubation laryngoscopy by an otolaryngology consultant revealed paradoxical vocal fold movement. POD 2 was unremarkable. However, the patient experienced SOB and stridor at 3:20 am on POD 3, prompting another visit from the RRT. Racemic epinephrine and a mixture of helium and oxygenation were administered, and an otolaryngology examination revealed the paradoxical movement of the vocal cords. Another CT was performed at 12:53 pm on POD 3, revealing prevertebral edema from C2 to C5, measuring 22 mm at the maximum level (Figure). The patient was transferred to the ICU and Spo2 remained >90% with inhalation of a mixture of helium and oxygen via a facemask. The helium and oxygen mixture was weaned off on POD 4 despite occasional SOB. The patient was discharged from the ICU on POD 5.
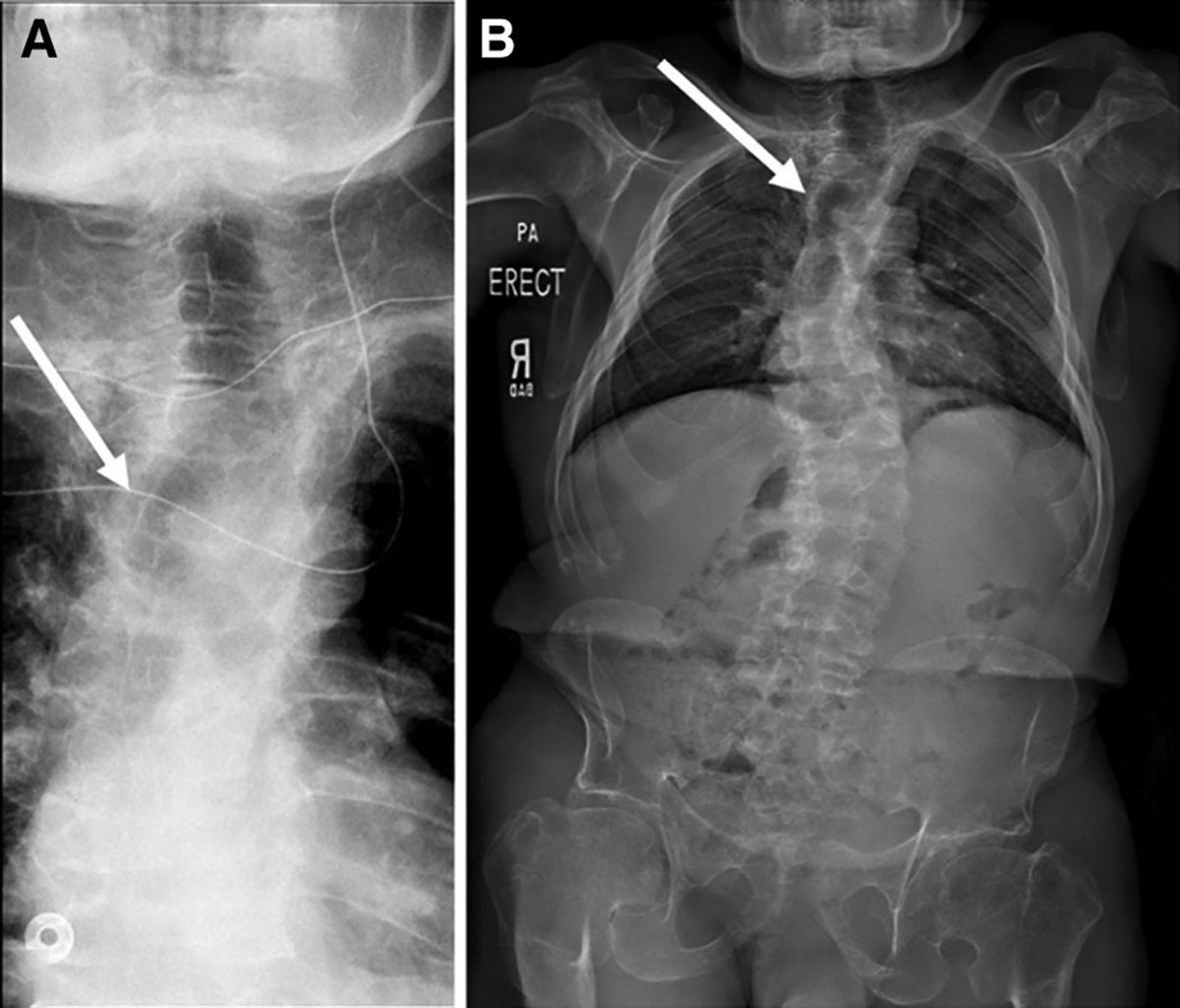
 Figure.:
Figure.: Neck computed tomography obtained on postoperative day 3. The arrow indicates prevertebral edema and fluid from the C2 through C5 level, measuring 22 mm in maximum thickness at the supraglottic level.
DISCUSSIONAirway obstruction occurs after emergence from general anesthesia. There are many causes of obstruction. A laryngoscopic examination must be performed to clearly attribute the cause of airway obstruction to PVCMD. PVCMD is characterized by the adduction of the vocal cords during inhalation and sometimes during exhalation. Awareness of PVCMD among anesthesia providers and other emergency medical professionals remains low. For instance, PVCMD was not mentioned as a “functional” obstruction in a recent paper on the management of difficult airways.10 The incidence of PVCMD after anesthesia remains unknown, partly due to the invasive nature of laryngoscopic examination, and partly due to its low awareness among providers. This lack of awareness among care providers may lead to failure in recognizing PVCMD, which can result in unnecessary treatments. Hicks et al11 reported that there is a paucity of knowledge and experience to establish guidelines for PVCMD evaluation and management.
Expiratory stridor due to PVCMD mimics the clinical picture of bronchospasm. However, bronchial dilators will not effectively treat PVCMD. The etiology of PVCMD is believed to be a combination of psychologic, neurologic, and physiologic components.11 The potential risk factors, such as GERD, anxiety, emotional distress, asthma, airway infection, and environmental irritants, must be noted. Our case report suggests that episodes of PVCMD in the past may predict recurrence. PVCMD can be managed conservatively. Unlike laryngospasm, which typically results in intense and constant upper airway obstruction, PVCMD is an intermittent upper airway obstruction with a rapid onset, and oxygenation is usually maintained. It has been reported that sedation using midazolam7 or treatment of pain using fentanyl8 may be helpful. No specific treatment other than basic airway support is required in most cases. Our patient originally responded well to a combination of midazolam, fentanyl, and dexmedetomidine. However, if PVCMD is not recognized, concern about airway obstruction, as suggested by the stridor, may lead to reintubation or tracheostomy. In the surgery setting, recognition and management of PVCMD can be very challenging. Multiple risk factors for airway obstruction, such as an anaphylactic reaction, hematoma, or edema, can coexist with PVCMD. Therefore, intubating patients with known PVCMD may sometimes be reasonable and necessary. However, extubation should be actively pursued when PVCMD is deemed to be the primary reason for airway obstruction, and other possibilities are ruled out.
Our patient experienced refractory PVCMD after cervical fusion. Therefore, it was necessary to rule out life-threatening causes, such as a hematoma after surgery. Careful monitoring of oxygenation is critical, and endotracheal reintubation should be considered if oxygenation is compromised. We hypothesize that continual administration of antianxiolytics may prevent the recurrence of refractory PVCMD.
In summary, awareness of PVCMD in daily practice remains limited among anesthesia professionals. Identification and management of perioperative PVCMD remain extremely challenging.
DISCLOSURESName: Xianren Wu, MD.
Contribution: This author helped in data collection, literature review, and article preparation.
Name: Xiaopeng Zhang, MD.
Contribution: This author helped in literature review and article preparation.
This manuscript was handled by: BobbieJean Sweitzer, MD, FACP.
ACKNOWLEDGEMENTSWe thank Mr Bradley Watts, CRNA in Geisinger Medical Center, Danville, PA, for helping us with patient care and data collection. We also thank Editage (www.editage.com) for English language editing.
REFERENCES 1. Hammer G, Schwinn D, Wollman H. Postoperative complications due to paradoxical vocal cord motion. Anesthesiology. 1987;66:686–687. 2. Michelsen LG, Vanderspek AF. An unexpected functional cause of upper airway obstruction. Anaesthesia. 1988;43:1028–1030. 3. Tousignant G, Kleiman SJ. Functional stridor diagnosed by the anaesthetist. Can J Anaesth. 1992;39:286–289. 4. Sukhani R, Barclay J, Chow J. Paradoxical vocal cord motion: an unusual cause of stridor in the recovery room. Anesthesiology. 1993;79:177–180. 5. Arndt GA, Voth BR. Paradoxical vocal cord motion in the recovery room: a masquerader of pulmonary dysfunction. Can J Anaesth. 1996;43:1249–1251. 6. Kleiman S, Tousignant G. Paradoxical vocal cord motion. Can J Anaesth. 1997;44:785–786. 7. Robert KW, Crnkovic A, Steiniger J. Post-anesthesia paradoxical vocal cord motion successfully treated with midazolam. Anesthesiology. 1998;89:517–519. 8. Neustein SM, Taitt-Wynter LM, Rosenblatt MA. Treating stridor with opioids: a challenging case of paradoxical vocal cord movement. J Clin Anesth. 2010;22:130–131. 9. Farley JD, Cheney M, Eckmann MS, Wallisch B. Paradoxical vocal fold motion disorder in the postanesthesia care unit. Anesthesiology. 2021;134:626–627. 10. Heidegger T. Management of the difficult airway. N Engl J Med. 2021;384:1836–1847. 11. Hicks M, Brugman SM, Katial R. Vocal cord dysfunction/paradoxical vocal fold motion. Prim Care. 2008;35:81–103.
留言 (0)