
記住我
The term “dacryolith” was first described by Cesoin in 1670 and refers to the concretions found within the lacrimal drainage system.1 They are commonly classified as infectious and noninfectious dacryoliths. The infectious are commonly noted within the canalicular system and are also called canaliculoliths, canalicular concretions, or simply infective concretions.2 The noninfectious dacryoliths are commonly isolated from the lacrimal sac and the nasolacrimal duct and are also called mucopeptide concretions.2 There are no definitive imaging features or clinical pointers in the preoperative period that can conclusively diagnose dacryoliths, although such cases have been documented when they get spontaneously extruded.3,4 More often, they are diagnosed incidentally during a dacryocystorhinostomy, and the reported incidence among all dacryocystorhinostomy surgeries is 5.7% to as high as 18%.1,5–7 Clinicopathological studies of 202 lacrimal sac biopsies revealed a prevalence of dacryoliths in 5% of the samples.8 The patients commonly present in the fifth and sixth decade, like those seen with cases of primary acquired nasolacrimal duct obstruction. The gender predisposition in dacryolithiasis is controversial, with recent studies challenging the earlier beliefs of a female preponderance.1 While several associations (gender, smoking, allergy, fungal colonization, altered hormonal status, foreign bodies, and cosmetics) are believed to contribute to the pathogenesis, they are, at best, speculative.1,7,9–11 This review aims to elucidate and reconstruct the possible sequence of events in the etiopathogenesis of noninfectious dacryolithiasis, drawing primarily on basic science work carried out over the last decade by the authors’ group, but also by other groups.5–30
ETIOPATHOGENESIS OF DACRYOLITHS Tear Biology EvidenceAlterations of the tear fluid dynamics and composition have long been considered as the trigger or initiating factor for dacryolithogenesis. The findings of partial or complete nasolacrimal duct obstruction are not uncommon in patients with dacryoliths.1,7,13 However, evidence is lacking that nasolacrimal duct obstruction directly initiates the process. In addition to tear fluid dynamics, tears from patients with dacryoliths were also analyzed and controversially discussed. Herzig and Hurwitz24 compared tear samples from 14 patients with dacryoliths and 7 healthy individuals for calcium, phosphorus, and uric acid concentrations and found no difference. In contrast, Lew et al.19 found decreased concentrations of lysozyme, potassium, and general proteins. The lower tear lysozymes can influence proteolysis, and this, combined with electrolyte imbalance (K+) and a relatively alkaline environment, may facilitate the aggregation of organic matter.19,20 The lower levels of tear lysozymes in chronic smokers have fueled the speculation of smoking as one of the contributing factors.9 On the other hand, it must also be mentioned that the epithelium of the lacrimal sac and nasolacrimal duct also produces lysozyme itself, along with many other antimicrobial peptides.26 However, it is unclear whether this is also altered in patients with dacryoliths. Besides, elevated mucins and trefoil family factor (TFF) peptides within the tear fluid would help lay down the amorphous matter.13,14 However, TFF peptides and mucins have also been studied within the dacryoliths and will be discussed in the following sections.
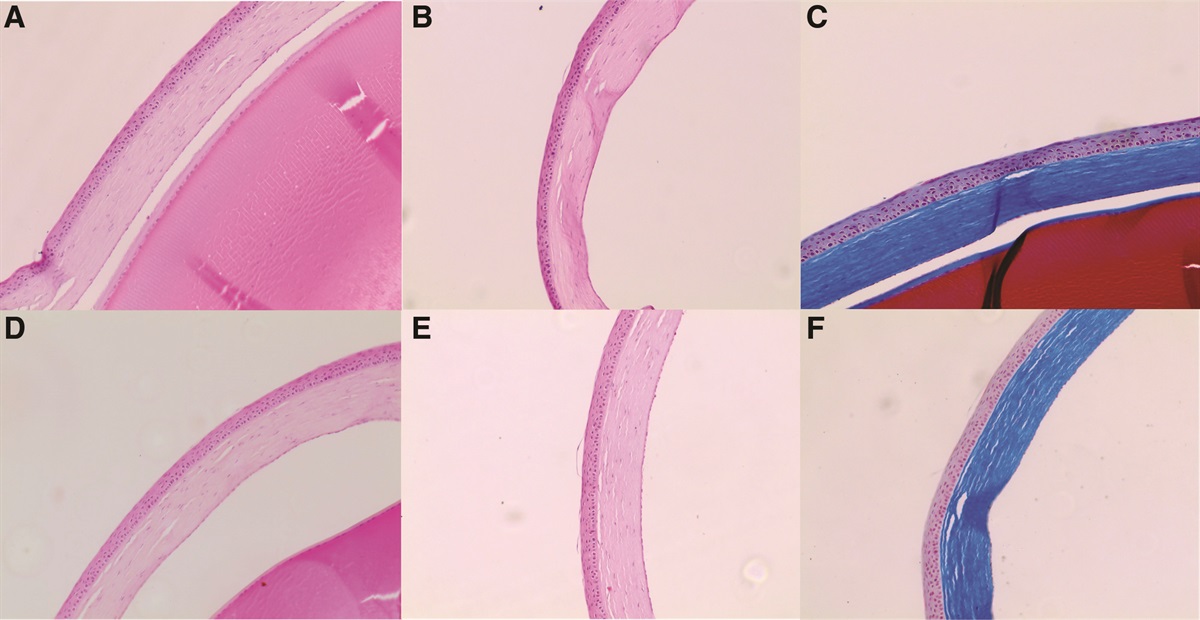
Histopathology and Immunohistochemistry EvidenceHistopathological examination of lacrimal sac dacryoliths or mucopeptide concretions has shown it to be composed of amorphous, intensely Periodic Acid Schiff-positive hyaline eosinophilic material that is laid in compact laminated layers.2,28 The surface irregularities can be stained eosinophilic or basophilic. The subsurface has vacuoles with minimal cellular content and bacteria.2,14 Occasionally, fissures can be observed within the substance of dacryoliths, and in general, analyses for calcium and iron are negative except for iron in the core (central innermost part of the dacryolith) although both deposits have also been reported.2,22–28
TFF peptides are secreted by mucin-secreting epithelial cells and bear a 3-loop trefoil domain. They line the lumina, stabilize mucins, and perform defense functions. Quantification of TFF peptides demonstrated that the production of all such peptides (TFF1, TFF2, and TFF3) is enhanced within dacryoliths.13 Several mucins like MUC1, MUC2, MUC5AC, MUC5B, MUC7, and MUC8 were demonstrated in significant proportions in dacryoliths. TFF peptides are known to influence rheological properties and are likely to contribute to the process of dacryolithogenesis.29 Certain alpha-defensins like DEF3 and secretory phospholipases were also detected in many tested dacryoliths.13
Immunohistochemistry assessment has demonstrated differential expression on the surface, periphery, and core areas of a dacryolith (Table).14 The central core showed heavy expression of von Willebrand factor and fibronectin. The core areas also demonstrated the presence of collagen III and human beta-defensins. The peripheral areas demonstrated the presence of lysozyme, collagen II, occasional cytokeratins, and S100-A9.14 The surface demonstrated a patchy presence of prolactin receptors. Mass spectroscopic analysis of dacryoliths has revealed the presence of several proteins, including hemoglobin, albumin, lysozyme, S-100A8, S-100A9, cathepsin, neutrophil elastase (NE), neutrophil gelatinase-associated lipocalin, myeloperoxidase, lactotransferrin, and prolactin-inducible protein showing that most core proteins of dacryoliths are involved in immune and inflammatory responses.21 These findings, when taken with electron microscopic features, provide new insights into the possible etiopathogenesis of dacryolith formation.
- Significant component expressions detected and their location within dacryoliths Significant component expressions in Dacryoliths 1.Trefoil factor peptides (TFF 1, TFF2, and TFF3)—widespread 2.Mucins (MUC1, MUC2, MUC4, MUC5AC, MUC5B, MUC7, and MUC8)—widespread 3.Alpha-defensins (DEF3)—patchy 4.Secretory phospholipase A2—diffuse 5.CD20 (B-lymphocytes)—focal and occasional 6.CD68 (Macrophages)—focal and occasional 7.von Willebrand factor—core of dacryolith 8.Fibronectin—core of dacryolith 9.Fibrinogen—core of dacryolith 10.Collagen (Coll I and Coll III)—diffuse 11.Beta defensin 2 (hBD2)—core of dacryolith 12.Beta defensin 3 (hBD3)—peripheral and patchy 13.Lysozyme—diffuse except core area. 14.Cytokeratin (CK1, CK2, CK4, and CK7)—patchy 15.Prolactin receptors (PRLR)—surface 16.S100 A9—core and periphery 17.Immunoglobulins IgG—patchy and on surface 18.Fetuin-A—surface and core 19.Aquaporin 9 (AQP9)—diffuse 20.Neutrophil elastase—diffuse 21.Myeloperoxidase—patchy and on surface 22.Peptidyl arginine deaminase (PAD4)—diffuse 23.Cathepsin G—patchy and on surface 24.Citrullinated histone (citH3)—surface and periphery 25.Resistin—surface and periphery 26.Azurocidin—surface and periphery 27.N-acetyl galactosamine (GalNAc)—surface and coreVery few studies looked at the electron microscopic features of dacryoliths.5,15,16,22,23 Orhan et al.22 studied a single dacryolith and found it to have an organic amorphous core composed of lobes and lobules. Komínek et al.5 additionally demonstrated the surfaces to be rough with ridges, occasional organic fibers within the substance of dacryoliths, and variable-sized spaces that were presumed to be gaseous products of metabolism. Lamanova and Bukharova23 studied several dacryoliths from a single patient and noted their shapes to be round or angular. The organic matrix was scaly and compact, likely due to mucins (as demonstrated earlier by Paulsen et al.13), and the inorganic component was found scattered on the surface and beneath a thin layer of the organic matrix.
Ali et al.16 studied scanning and transmission electron microscopic features of multiple dacryoliths obtained during the dacryocystorhinostomy of 10 patients. They noted that dacryoliths take the shape of the segment of the lacrimal drainage where they are housed. The external surfaces and full-thickness cut sections were mostly amorphous, with few intervening rough heterogeneous areas. Cellularity was comparatively less on the surface. The surface of the lacrimal sac dacryoliths showed rougher texture compared to those isolated from nasolacrimal ducts. The cut sections revealed 2 types of craters: one with noncontiguous perforations and blood cells and the other without them. Vacuoles and fissures were seen on scanning and transmission electron microscopy and appeared to result from cutting and drying artifacts rather than any metabolic process. A few scattered bacteria were noted, but there was no evidence of any biofilm formation. The core of the dacryolith was made up of an extensive network of fibrillary tangles (which the later immunohistochemistry studies14 showed to be composed of fibrinogen and fibronectin). Besides, the core also showed intervening red blood cells, granulocytes, epithelial cells, and intervening granular material. None of the several dacryoliths studied showed any fungal filament or organic fibers although fungal filaments were discovered in an earlier study.13
Evidence From Three-Dimensional Cinematic RenderingCinematic rendering techniques using Monte Carlo path tracing algorithms were utilized to study the surface and core of dacryoliths.17 The cinematic rendering techniques facilitated three-dimensional volume reconstruction of the dacryoliths along with variable color transfer display to depict textures and densities across the sample. Each dacryolith was then sliced and viewed at 100 microns intervals, and virtual camera images were obtained and further analyzed.17 The dacryoliths demonstrated uniform consistency with minimal heterogeneity from the surface to the core. However, the core was grossly different in texture and density and was identified as the “nidus” seen in earlier immunohistochemistry and electron microscopic studies.14–16 The location of the nidus was usually paracentral and rarely was there more than one nidus. The nidus was compact and dense, was well delineated, occupied <10% of the total dacryolith area, and showed a gradual reduction of density towards its periphery.
Neutrophil Extracellular Traps Drive DacryolithiasisNeutrophil extracellular traps (NETs), as the name suggests, are produced by the neutrophils which form the first line of defense. They are a network of extracellular DNA strings that limit the dissemination of microorganisms and facilitate their elimination. Recently, several techniques (microcomputed tomography, magnetic resonance imaging, immunofluorescence, mass spectrometry, and enzyme analysis) have been used together to assess the role of innate and adaptive immune mechanisms in the formation of dacryoliths.18 They confirmed the prior findings of immunohistochemistry, electron microscopy, and three-dimensional cinematic rendering studies. The structure of dacryoliths was found to be stratified with few and scattered electron-dense inclusion reflecting minimal calcification, if any. The presence of a few cytokeratins (CK2, CK9) reflects the presence of epithelial cells. Several proteins related to neutrophils were noted in the core of the dacryolith and included S100A9, cathepsin, citrullinated histone-3 (citH3) resistin, neutrophil defensin1, myeloperoxidase, lactoferrin, lysozyme, NE, and azurocidin.18 A considerable amount of NE activity was noted in all the dacryoliths studied. These and several other proteins could contribute to the structural aggregation of proteins in certain areas. The granular material noted in the earlier electron microscopy study16 could partly be these aggregated proteins. Estimation from fluorescent staining revealed high hemoglobin levels in the core areas and diffuse high expression of peptidyl arginine deaminase (PAD4), IgG, and N-acetyl galactosamine (GalNAc). Colocalization of specific neutrophil markers (NE, CitH3, and myeloperoxidase) and citrullination (citH3 and PAD4) was widely demonstrated. NETs stained by anti-NE and specific anti-DNA were found at 2 locations, in the core (anti-NE alone) and on the surface (colocalization of NE and DNA), reflecting the formation of NETs.18 This means that neutrophils in the nidus have a role in the early stages, and fully formed NETs play a role in the later stages following mucin deposits. NETs are believed to maintain a proinflammatory environment and may prevent clearance of amorphous dacryolith matter.18
RECONSTRUCTING THE POSSIBLE SEQUENCE OF EVENTS: THE STORY SO FARThe figure is a flowchart that sequentially reconstructs the possible sequence of events in dacryolithiasis in 4 broad stages: 1) stage of susceptibility, 2) stage of initiation/trigger, 3) stage of development, and 4) the stage of maintenance. The initial triggering event is the lacrimal sac or nasolacrimal duct epithelial breach secondary to a physical or chemical trauma in a susceptible individual. This susceptibility could be secondary to altered tear film dynamics or composition (quantitative and qualitative protein alterations and electrolyte imbalance) aided by several other factors (age, evolving nasolacrimal duct stenosis or obstruction, gender, smoking, allergy, altered hormonal status, cosmetics) whose role is not very clear at present. Once an epithelial breach happens, microleakage of blood with cellular components like red blood cells, neutrophils, and thrombocytes forms the nidus. The protective mechanisms like increased production of mucins and TFF peptides from the lacrimal sac and the tear film help in the sequentially laying of mucopeptides. The local lacrimal sac cellular debris washed cellular debris from the ocular surface, and possibly extraneous components like dirt in tear fluid partly contribute to the dacryolith mass. All these mechanisms involved in the sequential building of dacryoliths are facilitated by altered rheological properties of the tear film. If the sequential laying continues, the dacryolith takes the shape of the segment of the lacrimal sac or nasolacrimal duct that houses it. The surface of a formed dacryolith then develops NETs that maintain the proinflammatory environment and prevent clearing of the dacryolith mass by innate mechanisms.
CONCLUSIONDacryolithiasis is a complex process occurring within the lacrimal system, and current evidence suggests a multifactorial etiology. There have been focused efforts to understand the processes involved in the etiopathogenesis of dacryolithiasis. The sequence of events can be summarized broadly into 4 stages: stage of susceptibility, stage of initiation/trigger, stage of development, and stage of maintenance. The triggering event is the breach of the lacrimal sac or nasolacrimal duct epithelium, leading to microleakage of blood. The blood clots act as a nidus for subsequent sequential laying of mucopeptides, cellular debris present locally, debris washed from the ocular surface, and extraneous agents in tears. This process is aided by altered rheology and composition of the tear film. Following the formation of a dacryolith, NETs form on the surface and contribute to the maintenance (nonclearance) of dacryoliths. Although the existing findings make plausible the rough stages and sequence of events as we have elaborated here for the formation of dacryoliths, the explanations remain a hypothesis that needs to be further analyzed. More micro- and molecular mechanisms need to be deciphered to get a complete picture and understand the causal relationships. Further work is needed on the development of dacryolithiasis susceptibility, the evolution of internal craters, the exact progression following fibrinogenesis, the evolution of NETs in the core of dacryoliths, interactions between components of the nidus, and the evolution of protein aggregation and its structural contributions. In addition, epidemiological studies would be helpful and if one reads the literature carefully, what has been said here roughly applies to the formation of most stones, but there also seem to be individual stones that are formed in a different way and have a completely different stone composition.30 This also needs to be analyzed further. The focused lacrimal clinician-scientists across the globe are well set to understand further the complex processes involved in dacryolithiasis and, hopefully, apply the obtained knowledge to manage them better or prevent their formation.

Dacryolithogenesis flowchart—Reconstructed sequence of events. ATC, altered tear components; ATR, altered tear rheology; CECO, cellular component; CEDB, cellular debris; DS, dacryolith substance; Ep, epithelium; LS, lacrimal sac; NETs, neutrophil extracellular traps; NLD, nasolacrimal duct; OcS CEDB, ocular surface cellular debris; PI, proinflammatory; TFF, trefoil family factor peptides.
REFERENCES 1. Mishra K, Hu KY, Kamal S, et al. Dacryolithiasis: a review. Ophthalmic Plast Reconstr Surg. 2017;33:83–89. 2. Perry LJ, Jakobiec FA, Zakka FR. Bacterial and mucopeptide concretions of the lacrimal drainage system: an analysis of 30 cases. Ophthalmic Plast Reconstr Surg. 2012;28:126–133. 3. Rosen WJ, Rose GE. Intranasal passage of dacryoliths. Br J Ophthalmol. 2000;84:799–800. 4. Kaye-Wilson LG. Spontaneous passage of a dacryolith. Br J Ophthalmol. 1991;75:564. 5. Komínek P, Červenka S, Zeleník K, et al. Lacrimal sac dacryolith (76 cases): a predictive factor for successful endonasal dacryocystorhinostomy? Eur Arch Otorhinolaryngol. 2014;271:1595–1599. 6. Berlin AJ, Rath R, Rich L. Lacrimal system dacryoliths. Ophthalmic Surg. 1980;11:435–436. 7. Yazici B, Hammad AM, Meyer DR. Lacrimal sac dacryoliths: predictive factors and clinical characteristics. Ophthalmology. 2001;108:1308–1312. 8. Lee-Wing MW, Ashenhurst ME. Clinicopathologic analysis of 166 patients with primary acquired nasolacrimal duct obstruction. Ophthalmology. 2001;108:2038–2040. 9. Repp DJ, Burkat CN, Lucarelli MJ. Lacrimal excretory system concretions: canalicular and lacrimal sac. Ophthalmology. 2009;116:2230–2235. 10. Baratz KH, Bartley GB, Campbell RJ, et al. An eyelash nidus for dacryoliths of the lacrimal excretory and secretory systems. Am J Ophthalmol. 1991;111:624–627. 11. Nagendran ST, Ali MJ, Dogru M, et al. Complications and adverse effects of periocular aesthetic treatments. Surv Ophthalmol. 2022;67:741–757. 12. Paulsen F. The human nasolacrimal ducts. Adv Anat Embryol Cell Biol. 2003;170:III–XI, 1. 13. Paulsen FP, Schaudig U, Fabian A, et al. TFF peptides and mucins are major components of dacryoliths. Graefes Arch Clin Exp Ophthalmol. 2006;244:1160–1170. 14. Ali MJ, Heichel J, Paulsen F. Immunohistochemical analysis of the lacrimal sac mucopeptide concretions. Ophthalmic Plast Reconstr Surg. 2019;35:562–565. 15. Ali MJ, Paulsen F. Ultrastructure of the lacrimal drainage system in health and disease: a major review. Ann Anat. 2019;224:1–7. 16. Ali MJ, Schicht M, Heichel J, et al. Electron microscopic features of the lacrimal sac mucopeptide concretions. Graefes Arch Clin Exp Ophthalmol. 2018;256:1313–1318. 17. Ali MJ, Scholz M, Singh S, et al. Etiopathogenesis of lacrimal sac mucopeptide concretions: insights from cinematic rendering techniques. Graefes Arch Clin Exp Ophthalmol. 2020;258:2299–2303. 18. Zlatar L, Timm T, Lochnit G, et al. Neutrophil extracellular traps drive dacryolithiasis. Cells. 2023;12:1857. 19. Lew H, Lee SY, Yun YS. Measurement of pH, electrolytes and electrophoretic studies of tear proteins in tears of patients with dacryoliths: a novel concept for dacryoliths. Ophthalmologica. 2004;218:130–135. 20. Norn MS. Tear fluid pH in normals, contact lens wearers, and pathological cases. Acta Ophthalmol (Copenh). 1988;66:485–489. 21. Mano F, Takimoto H, Oe M, et al. Proteomic analysis of dacryoliths from patients with or without topical rebamipide treatment. Biomed Hub. 2018;3:1–11. 22. Orhan M, Onerci M, Dayanir V, et al. Lacrimal sac dacryolith: a study wit atomic absorption spectrophotometry and scanning electron microscopy. Eur J Ophthalmol. 1996;6:478–480. 23. Lamanova LM, Bukharova OV. Binding of metals in dacryoliths by means of biomineralization. Micron. 2019;124:102688. 24. Herzig S, Hurwitz JJ. Lacrimal sac calculi. Can J Ophthalmol. 1979;14:17–20. 25. Stein M, Bethmann D, Viestenz A, et al. Concrements of the lacrimal apparatus. Klin Monbl Augenheilkd. 2023;240:44–52. 26. Paulsen FP, Pufe T, Schaudig U, et al. Detection of natural peptide antibiotics in human nasolacrimal ducts. Invest Ophthalmol Vis Sci. 2001;42:2157–2163. 27. Iliadelis E, Karabatakis V, Sofoniou M. Dacryoliths in chronic dacryocystitis and their composition (spectrophotometric analysis). Eur J Ophthalmol. 1999;9:266–268. 28. Iliadelis ED, Karabatakis VE, Sofoniou MK. Dacryoliths in a series of dacryocystorhinostomies: histologic and chemical analysis. Eur J Ophthalmol. 2006;16:657–662. 29. Paulsen F, Corfield A, Hinz M, et al. Tear outflow Impact of mucins and TFF-peptides. Ophthalmologe. 2004;101:19–24. 30. Ozer S, Ozer PA, Ortarik Z, et al. Analysis of inorganic elements in a dacryolith using polarised X-ray fluorescence spectrometry: a case report. Eye (Lond). 2012;26:887.
留言 (0)