
記住我

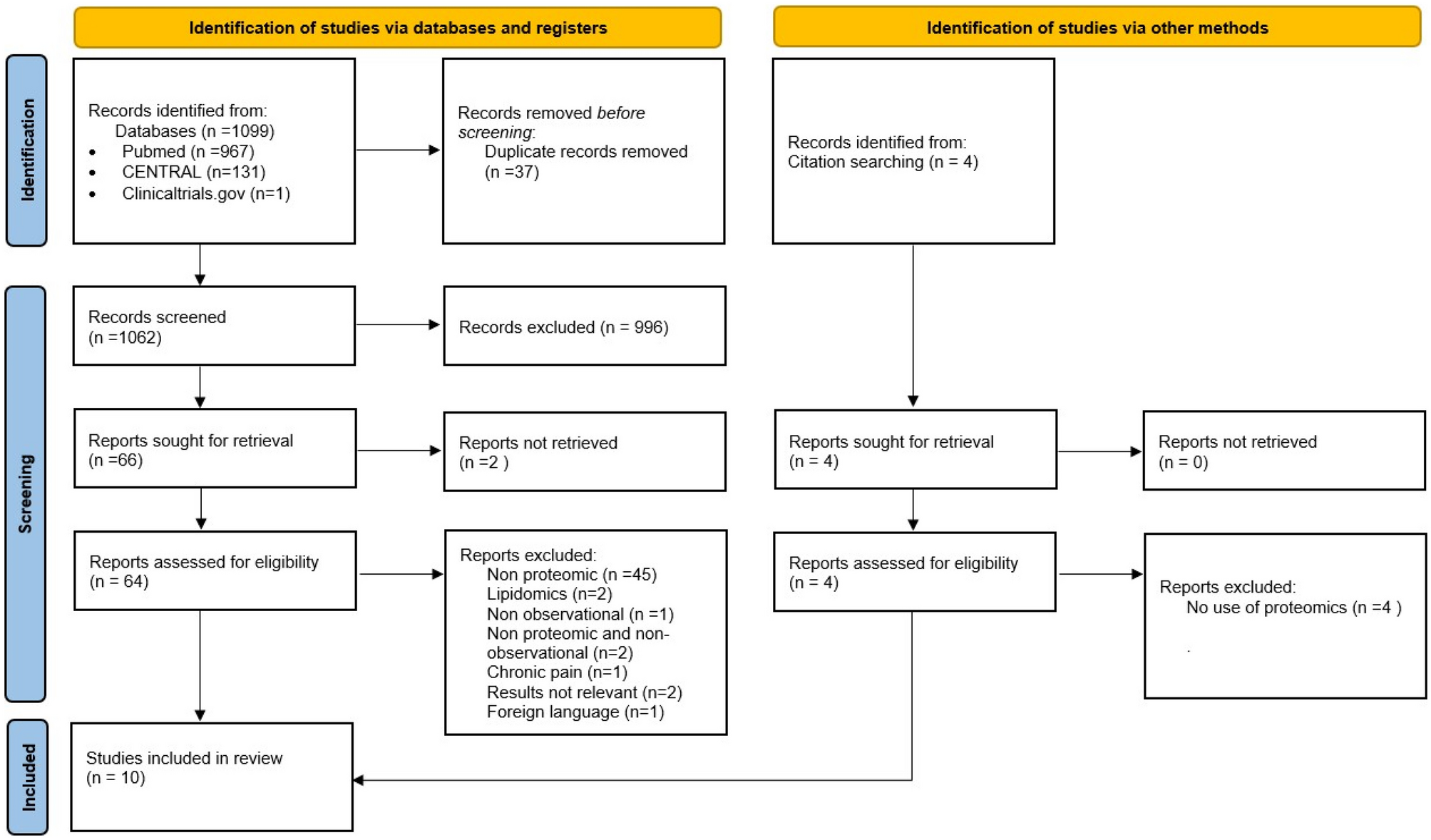
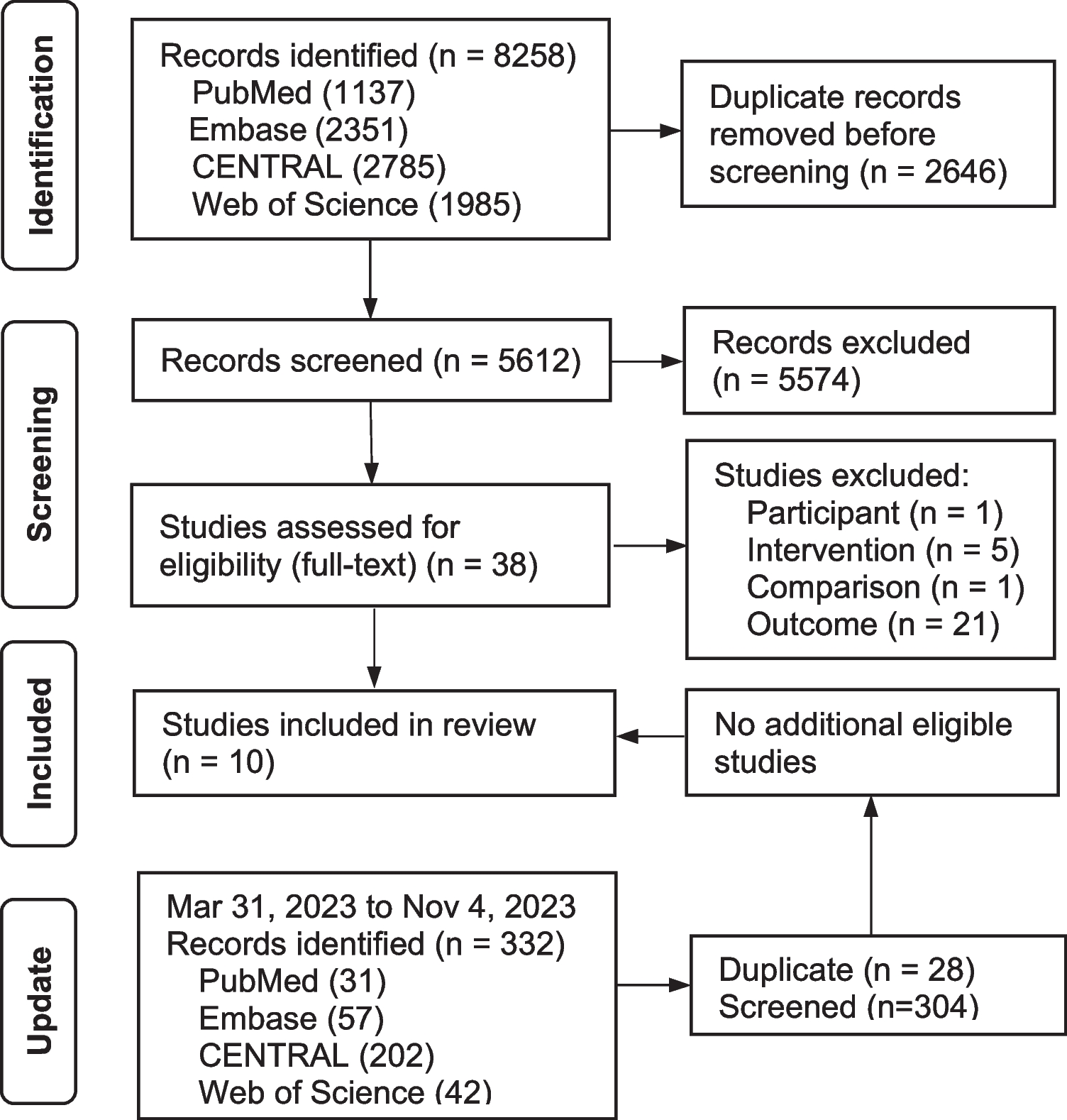
A total of 6 784 records were identified, and 14 studies [16,17,18,19,20,21,22,23,24,25,26,27,28,29] were included with 1263 participants in this review (Fig. 1). We contacted the authors of one study [16] via email to clarify information not adequately reported. After responding, we used the data as reported in this review. All 14 studies mentioned that there was no significant difference in general data between the observation group and the control group (P > 0.05), which was comparable.
Fig. 1
Article selection process
The intervention was classified to the different treatment method and acupuncture prescription. Based on the treatment classification, among the included 14 studies, nine studies [16, 20,21,22,23,24, 26, 28] selected distal acupoints combined with lumbar movement (referred to as motion-style acupuncture treatment). We categorized the included studies into four types and performed the subgroup analyses based on stimulating acupuncture points while simultaneously instructing patients to engage in specific movements (Table 3). Only one study used LROM as measurement [27] and two studies used the Schober test as measurement [19, 25]; we combined them into no movement group for analysis. Among the studies, common oral medication for acute/subacute NSLBP include NSAIDs (such as diclofenac sodium [17, 21, 26], ibuprofen [22, 23], loxoprofen [16], meloxicam [18, 20, 24, 25, 27, 28], nimesulide [29]) as well as muscle relaxants (eperisone) [19]. With studies, common distal acupuncture points included EX-UE 7 [16, 20, 23, 24, 28], GV 26 plus SI 3 [28, 29], SI 6 [26], and distal points of the meridian (SI 6, BL 2, GV 26) [21]. The remaining five studies selected different proximal points [19], distal points [17, 18], or proximal combined with distal points [22, 29] (Table 4).
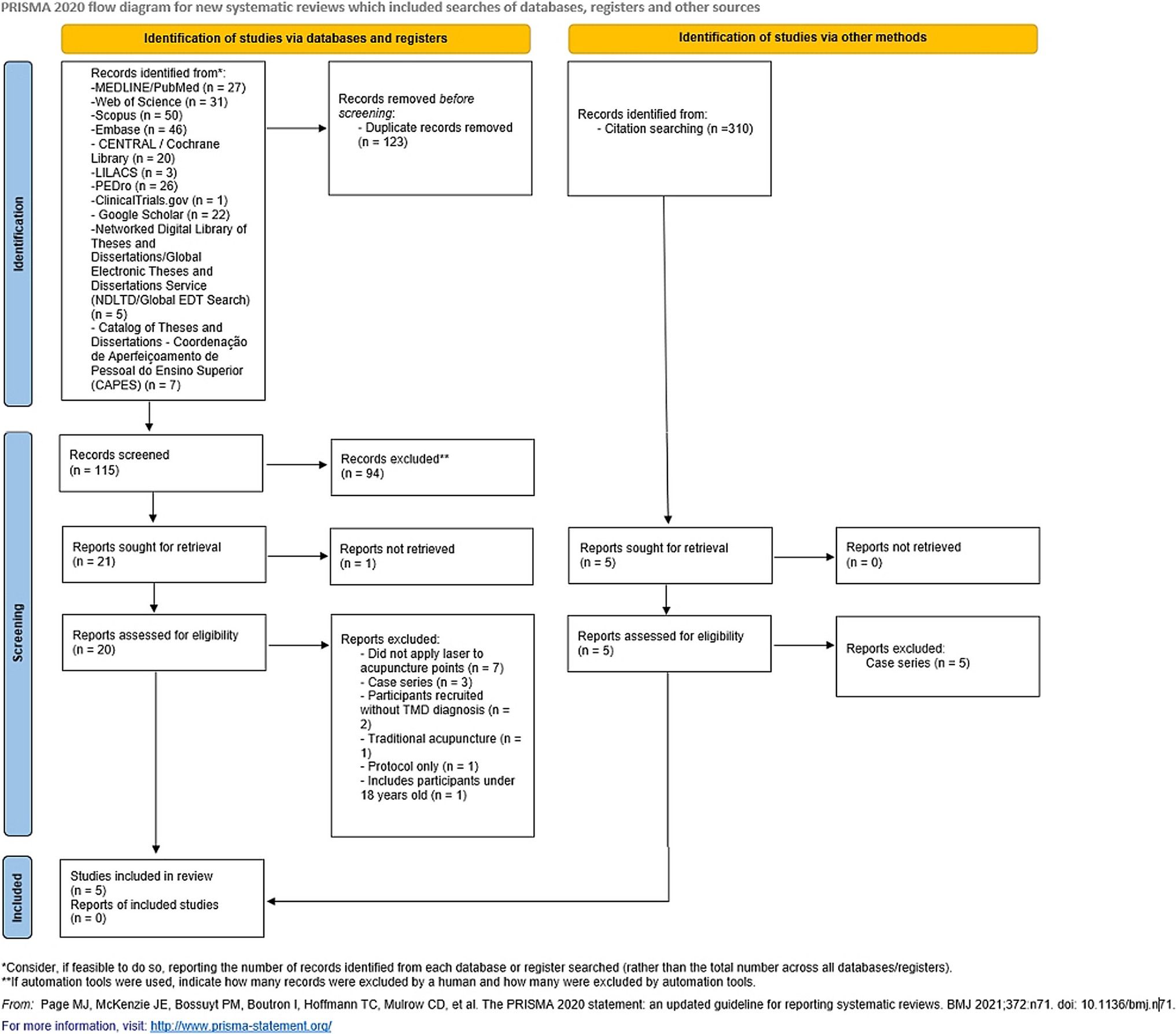
Table 3 Subgroup and Intervention methodTable 4 Characteristics of Included StudiesQuality of the Included StudiesAdequate methods for generating random sequences were reported in ten articles [16,17,18,19, 21,22,23,24,25,26] utilizing the random number table technique. In four studies [20, 27,28,29], the process of random sequence generation was not mentioned, leading us to evaluate them with an unclear risk of bias. Two studies provided detailed descriptions of allocation concealment methods [23, 26], whereas the remaining studies did not specify the use of allocation concealment, resulting in an assessment of unclear risk of bias. Blinding of acupuncture therapists was not feasible in any of the studies, leading to a high-risk bias rating. One study detailed the blinding of outcome evaluation and assessment procedures [17] resulting in a low-risk bias rating. Three studies [17, 18, 23] were deemed to have a high risk of attrition bias due to a significant number of subjects who dropped out of the studies. In the case of all remaining studies, the protocol was unavailable, resulting in an assessment of an unclear risk of reporting bias (Fig. 2).
Fig. 2
Quality of the included studies
Effects EstimatesPainThe results of the meta-analysis indicated that acupuncture therapy was slightly more effective than oral medication in improving pain (P < 0.00001, I2 = 92%, MD = −1.17, 95% CI [−1.61, −0.72]; 9 studies, 468 participants; moderate effect, very low-quality evidence).
Subgroup analysis results revealed that the movement group (involving multiple acupuncture sessions) (with acupuncture administered 3–6 times during lumbar movement) (P < 0.00001, I2 = 47%, MD = −2.42, 95% CI [−3.03, −1.80]; 3 studies, 151 participants; large effect, very low-quality evidence) exhibited better outcomes than the no movement group (involving only electroacupuncture at Ashi points) (P < 0.00001, I2 = 0%, MD = −0.42, 95% CI [−0.57, −0.27]; 2 studies, 127 participants; trivial effect, low-quality evidence) and the no movement group (acupoint selection of the physician’s personal clinical experience) (P = 0.61, I2=0%, MD = −1.10, 95% CI [−1.24, −0.97]; 3 studies, 133 participants; moderate effect, very low-quality evidence).
No significant difference was observed between the effects of the movement group (involving acupuncture administered only once) and the oral medication group (P = 0.36, Z = 0.92, MD = −0.32, 95% CI [−1.00, −0.36]; 1 study, 57 participants; trivial effect, low-quality evidence) (Table 5; Fig. 1 in the Supplementary Material).
Table 5 Result of meta-analysis and evidence gradeFunction 1.RMDQ
According to the results of the meta-analysis, acupuncture therapy exhibited a significant advantage over oral medication with a substantial effect (P < 0.00001, I2 = 90%, SMD = − 1.42, 95% CI [− 2.22, − 0.62]; 6 studies, 346 participants; large effect, very low-quality evidence).
Subgroup analysis results indicated that the movement group (involving multiple acupuncture sessions) (P < 0.00001, I2 = 90%, SMD = − 1.37, 95% CI [− 2.39, 0.35]; 3 studies, 205 participants; large effect, very low-quality evidence) and the no movement group (acupoint selection of the physician’s personal clinical experience) (P = 0.21, I2 = 37%, SMD = − 2.23, 95% CI [− 2.92, 1.54]; 2 studies, 93 participants; large effect, very low-quality evidence) were both superior to the oral medication group. However, no significant difference was observed between the no movement group (involving electroacupuncture at Ashi points only) (P < 0.00001, SMD = 0.00, 95% CI [− 0.60, 0.60]; 1 study, 48 participants; trivial effect, very low- quality evidence) and the oral medication group (Table 5; Fig. 2 in the Supplementary Material).
2.In terms of improving LROM in patients with acute/subacute NSLBP, there was no significant difference between acupuncture therapy and oral medication (P < 0.00001, I2 = 100%, MD = 33.92, 95% CI [−19.03, 86.86]; 1 study, 95 participants; trivial effect, very low-quality evidence) (Table 5; Fig. 3 in the Supplementary Material).
3.In terms of improving Schober test scores in patients with acute/subacute NSLBP, there was no significant difference between acupuncture therapy and oral medication (P = 0.009, I2 = 85%, MD = 1.27, 95% CI [−0.77,3.31]; 2 studies, 120 participants; trivial effect, very low-quality evidence) (Table 5; Fig. 4 in the Supplementary Material).
Improvement RateBased on the results of the meta-analysis, acupuncture therapy was associated with a 12% improvement rate compared to oral medication in patients with acute/subacute NSLBP (P < 0.0001, I2 = 54%, RR = 1.11, 95% CI [1.05, 1.18]; 14 studies, 1078/1028 participants; trivial effect, very low-quality evidence).
Subgroup analysis results revealed that the movement group (involving multiple acupuncture sessions) (P = 0.26, I2 = 22%, RR = 1.19, 95% CI [1.09, 1.30]; 7 studies, 385/448 participants; trivial effect, low-quality evidence) and the no movement group (acupoint selection of the physician’s personal clinical experience) (P = 0.03, I2 = 63%, RR = 1.09, 95% CI [0.99, 1.21]; 5 studies, 494/548 participants; trivial effect, very low-quality evidence) exhibited better outcomes than the oral medication group. However, there was no significant difference between the movement group (involving acupuncture administered only once) (P = 0.93, I2 = 0%, RR = 1.09, 95% CI [0.94, 1.27]; 2 studies, 76/85 participants; small effect, low-quality evidence), the no movement group (involving electroacupuncture at Ashi points only) (P = 0.43, I2 = 0%, RR = 1.02, 95% CI [0.96, 1.10]; 2 studies, 123/127 participants; trivial effect, low-quality evidence), and the oral medication group (Table 5; Fig. 5 in the Supplementary Material).
SafetyWith studies, among which ten did not mention adverse events or reactions while four studies provided descriptions of adverse reactions:
1.Fan and Wu [17]: The acupuncture group and the oral medication group each comprised 60 cases. No adverse reactions were reported in either group.
2.Xu [26]: The acupuncture group and the oral medication group each included 50 cases. In the oral medication group, 2 cases experienced upper abdominal pain and discomfort as adverse reactions; the acupuncture group did not report any adverse reactions.
3.Sun et al. [27]: There were a total of three groups: the BL 57 group with 32 cases, the Ashi point group with 31 cases, and the medication group with 32 cases. In the Ashi point group, one case experienced mild fainting during acupuncture. Following needle removal, the BL 57 group and the Ashi point group reported 3 and 5 cases of minor bleeding, respectively. The oral medication group did not provide reports of adverse reactions.
4.Huang [24]: Both the acupuncture group and the oral medication group had 30 cases. In the acupuncture group, 2 cases experienced fainting, and 1 case had a subcutaneous hematoma. The oral medication group did not report any adverse reactions.
Sensitivity AnalysisAfter sequentially excluding each trial from the meta-analysis, there were no substantial differences between the pre-sensitivity and postsensitivity pooled effects for the effective rate, motor dysfunction, and the lumbar range of motion-Schober.
留言 (0)