
記住我
In patients with ischemia and no obstructive coronary artery disease (INOCA), the underlying pathological substrate is considered to be coronary microvascular dysfunction (CMD) and/or epicardial coronary spasm.1,2 Both of these vascular dysfunction mechanisms may co-exist and contribute to INOCA.
The two aspects of CMD that are most responsible for microvascular angina symptoms with their ischemia-generating potential are structural remodeling implying an increase in wall-to-lumen ratio and/or reduced capillary density (rarefaction).3 The hemodynamic correlates of these changes are reflected in impaired response to an endothelium-independent vasodilator (e.g. adenosine), and increased microvascular resistance; and functional arteriolar dysregulation that implies the existence of endothelial dysfunction, which is associated with decreased vasodilation and also paradoxical vasoconstriction.4 Hyperventilation (HYP), smoking, emotional stress, cold exposure, and exercise (EXE) count among triggering stimuli for provoking epicardial and/or microvascular spasms. Symptoms of vasospastic angina (VSA) can be caused by dysfunction at the level of both vascular smooth muscle and/or endothelial cells.2,3
Distinguishing the prevalence of these INOCA endotypes is important in order to tailor an appropriate therapy that would ensure better clinical outcomes in these patients. Currently, for the complete diagnostic assessment of patients with INOCA, the European Society of Cardiology (ESC) Guidelines endorse invasive coronary functional testing. Acetylcholine (ACH) testing is supported by IIb recommendation5 for assessing endothelial-dependent vasoreactivity and vasospasm in epicardial coronary vessels and microcirculation, while a IIa recommendation5 supports adenosine-induced hyperemia for the evaluation of endothelium-independent CMD addressed by two standard indexes: coronary flow reserve (CFR) and index of microvascular resistance (IMR).5
Up to 70% of patients (more frequently women) with chest pain and stress testing positive for myocardial ischemia undergoing invasive coronary angiography (CAG) do not have obstructive coronary artery disease (CAD), and are therefore being recognized under the clinical entity of INOCA.6 These patients represent a significant financial burden for the healthcare system considering high estimated lifetime costs that tend to equal those of an obstructive CAD, as they have high rates of recurrent symptoms and repeated diagnostic procedures together with an impaired quality of life.7 Furthermore, this points out the need for having noninvasive, easily available, and versatile diagnostic tools that would increase the yield of specific diagnosis in patients with INOCA and elucidate INOCA endotypes.
Previous studies suggest that HYP is a clinically useful provocative test, as this test has been shown by angiography to induce coronary artery spasm in susceptible patients.8 The role of transthoracic echocardiography (TTE) with Doppler for assessing coronary flow velocity reserve (CFVR) in the left anterior descending artery (LAD) during provocative tests in patients with chest pain and INOCA was also acknowledged in the new Guidelines of the American College of Cardiology/American Heart Association for Evaluation and Diagnosis of chest pain, receiving recommendation IIb.9
The aim of our study was to assess the feasibility and potential value of noninvasive assessment of dynamic CMD in INOCA patients in order to identify different endotypes of coronary vasomotor dysfunction in patients with angina and suspected coronary vasospasm. The noninvasive assessment was based on stress echocardiography and CFV-LAD evaluation after vasoconstrictive and vasodilator stimuli. As vasoconstrictive stimuli targeting the dysfunctional endothelium, we used HYP followed by semi-supine exercise (EXE), whereas adenosine (ADO) was the vasodilatory stimulus, acting through a mainly endothelium-independent mechanism and vascular smooth muscle cell relaxation.
Materials and methods Study populationInitially, we have prospectively enrolled 46 patients with a history of angina like chest pain occurring during rest, early in the morning or during the night, on cold exposure or on effort.
CAD has previously (<1 year) been excluded in all patients by CAG or multidetector computed tomography (MDCT) scan of coronary arteries. CAG was performed in 24 (60%) patients because of positive stress ECG test, 7 (17%) patients had previous myocardial infarction with no obstructive epicardial disease, and 9 (23%) had persistent complaints indicative of angina. Clinical data, medical history, presence of cardiovascular risk factors as well as symptom characteristics were obtained. Concerning the risk factors, patients were evaluated for the presence of both traditional risk factors (e.g. hypertension, dyslipidemia, diabetes mellitus, smoking habits) and nontraditional risk variables associated with vasomotor dysfunction (e.g. rheumatic disorders, menopause).
Patients included in the study had to have the ability to perform a physical test, as well as an optimal acoustic window that would enable accurate wall motion assessment and best possible Doppler signal tracing of diastolic coronary flow.
Study exclusion criteria were severe form of chronic obstructive pulmonary disease, atrial fibrillation, history of epilepsy, bundle branch block, severe valvular heart disease, presence of cardiomyopathies, and left ventricular ejection fraction (LVEF) less than 55%.
Six patients were excluded from analysis: four because of suboptimal signal of spectral Doppler and two because of obstructive chronic pulmonary disease.
All patients had to discontinue the use of their medications 24 h prior to testing and also to restrain from beverages containing caffeine 12 h before the tests.
The study protocol was approved by the Medical Ethics Committee of Clinical Center of Serbia. All patients were informed about the procedure and provided consent.
Study protocolEchocardiographic examination, HYP+EXE SE tests, and CFV measurements (before and during provocation with HYP, EXE, and ADO) were conducted in all 40 patients.
Study protocol is presented in Fig. 1.
 Fig. 1:
Fig. 1: Study protocol.
Echocardiographic and coronary flow velocity assessmentStandard TTE stress echocardiography and CFV measurements were performed using a commercially available (GE Vingmed Ultrasound AS, Horten, Norway) equipped with a 1.3–4.0 Mhz transducer (GE Vivid M5S probe, GE Healthcare). All standard echocardiographic views, 2D, M-mode, and Doppler measurements were obtained according to recent guidelines.10 Wall Motion Score Index (WMSI) was evaluated with a 17-segment model of the left ventricle; each segment scored from 1 = normal/hyperkinetic to 4 = dyskinetic.10 Acquisitions were reviewed by an investigator unaware of the primary analysis results. Interobserver agreement was 90%.
TDE evaluation of coronary flow velocityAfter the standard echocardiographic examination Coronary flow velocity was performed using the GE Vivid M5S probe 1.3–4 MHz with settings dedicated for coronary flow measurements. Doppler signal for the distal segment of the LAD artery was acquired. Color Doppler flow mapping was performed by decreasing the Nyquist limit to 16–24 cm/s. A sample volume (3–5 mm wide) was positioned on the color flow signal and pulsed Doppler tracings of peak diastolic flow velocities were obtained. With the patient positioned in the left lateral decubitus, the acoustic window was searched for with the transducer placed in the midclavicular line at the level of the fourth and fifth intercostal space in order to obtain a modified three-chamber view.11 CFV recordings were performed with the transducer placed in a stable position during rest, at the end of hyperventilation, at peak exercise, and during maximal hyperemia induced with ADO.
Abnormal response to HYP was defined as CFV ratio (stress/rest) less than 1.0 (vasoconstrictor response). CFVR at peak HYP+EXE was expected to be at least 2 as an indicator of preserved endothelial-dependent vasodilatation, while CFVR less than 2 was considered a blunted response.
The endothelium-independent mechanism of vasodilatation was assessed with intravenous (i.v.) ADO administration (140 μg/kg over 1 min). CFVR measurements were completed off-line, using the integrated software package of the ultrasound system. TTE CFVR for LAD was calculated as the ratio of peak hyperemic to basal diastolic flow velocities. An average of the measurements in three cardiac cycles was obtained. On the basis of previously defined diagnostic and prognostic cut-off values, CFVR less than 2.0 was considered abnormal, indicating a blunted vasodilatory response.12
Hyperventilation and supine bicycle stress echocardiographic protocolHyperventilation testing has long been used for the detection of epicardial artery vasospasm in susceptible patients.13 Respiratory alkalosis induced by hyperventilation causes a reduction in the concentration of hydrogen ions, which under physiological conditions compete with calcium ions for active transmembrane transport to enter the smooth muscle cell of the coronary artery. This alkalotic state tips the balance in favor of an increased intracellular calcium influx, with more calcium entering the cell and reaching the regulatory troponin site, thus causing vasoconstriction.14,15 EXE test was performed immediately after HYP, in order to test the endothelium-dependent ability for vasodilation after spasm provocation.16,17
Following the echocardiographic examination and CFV measurements under resting conditions, the patient would hyperventilate for 5 min, at a respiratory rate of at least 25 breaths per minute. The time frame in which the test was expected to be positive was at the end of hyperventilation, when CFV was measured again.
If negative for ischemia based on wall motion criteria, or with RWMA in three segments or less, supine bicycle EXE test was performed immediately after to test flow-mediated endothelial-dependent vasodilatation.
Every 3 min, 25 W load increments (starting from 50 W) were performed until maximal heart rate was reached, or new or worsening wall motion abnormality, significant ECG changes, or symptoms occurred. At peak stress, all standard acoustic windows and CFV measurements were obtained.
Twelve-lead ECG, blood pressure, as well as the occurrence of symptoms were continuously monitored during the protocol. TDE CFV of LAD was measured at rest, at the end of hyperventilation, and at peak exercise.
The entire duration of testing from preparation to written response was always less than 1 h.
Adenosine protocolAll patients underwent ADO stress echocardiography testing in order to test adenosine-mediated vasodilation. TTE Doppler CFVR for LAD was performed 2 h after the HYP+EXE test, under the previously described protocol.
Statistical analysisAll data were entered into the database and then processed using the statistical program SPSS 21 (SPSS, Chicago, Illinois, USA). Quantitative variables were expressed as mean value ± standard deviation (SD). Comparison of quantitative variables was done according to the two-tailed Student's t-test (paired for repeated measurements). Dichotomous variables were compared using χ2 statistics and Wilcoxon signed-rank test. Statistical correlation between echocardiographic variables was examined using Pearson's linear correlation coefficient. A P-value less than 0.05 was considered statistically significant.
ResultsForty patients were enrolled in the study. Their demographic and clinical characteristics are presented in Table 1.
Table 1 - Patient characteristics Patients N = 40 Percentage % Female 32 80 Age (years) 56.3 ± 13.11 BMI (kg/m2) 25.95 ± 3.39 Obese (BMI ≥ 25) 23 57.5 Hypertension 31 77.5 Dyslipidemia 28 70 Diabetes mellitus 6 15 Current/former smoker 13 32.5 Menopause 23 57.5 Rheumatic disorders 10 25 Therapy Beta blockers 23 57.5 Calcium antagonists 9 22.5 Nitrates 3 7.5 ACEi/ARB 19 47.5 Angina characteristics Resting 18 45 During exercise 29 72.5 Cold exposure 12 30 Between 4 and 6 a.m. 9 22.5 Emotion/stress 14 35 Dyspnea 15 37.5 MINOCA 6 15ACEi, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; MINOCA, patients who previously had myocardial infarction with non-obstructive coronary arteries.
Patients were predominantly women, while the most prevalent cardiovascular risk factors were hypertension and hyperlipidemia (77.5 and 70%, respectively).
The most frequent onset of angina was during exercise but also combined with emotional stress or cold exposure, followed by angina occurring under the resting conditions. There was no clear distinction between the types of anginal pain experienced by each patient.
Feasibility of the HYP+EXE test was 100%, because all patients performed the test according to the study protocol, and reached their maximal predicted heart rate or physical limitation. No serious side effects occurred during test performance and there was no need for applying nitrates i.v.
Hyperventilation test result – vasospasm stimuliHYP test was performed for vasospasm provocation. Significant increase in heart rate and double product were observed during HYP (Table 2).
Table 2 - Hemodynamic parameters during hyperventilation/exercise test N = 40 REST HYP HYP+EXE P ∗ P ∗∗ Heart rate (bpm) 78.32 ± 13.95 97.23 ± 19.74 136.70 ± 17.81 <0.001 <0.001 SBP (mmHg) 130.62 ± 16.69 136.03 ± 20.33 170.62 ± 30.56 0.015 <0.001 DBP (mmHg) 79.00 ± 11.11 83.08 ± 14.36 93.50 ± 15.49 0.033 <0.001 DP (mmHg∗bpm) 10 244.50 ± 2353.50 13 214.74 ± 3266.64 23 460.37 ± 5569.76 <0.001 <0.001bpm, beats per minute; DP, double product; EXE, exercise; HYP, hyperventilation; REST, resting conditions.∗means multiply by.P∗ statistical difference between REST and HYP, P∗∗ statistical difference between HYP and HYP+EXE.
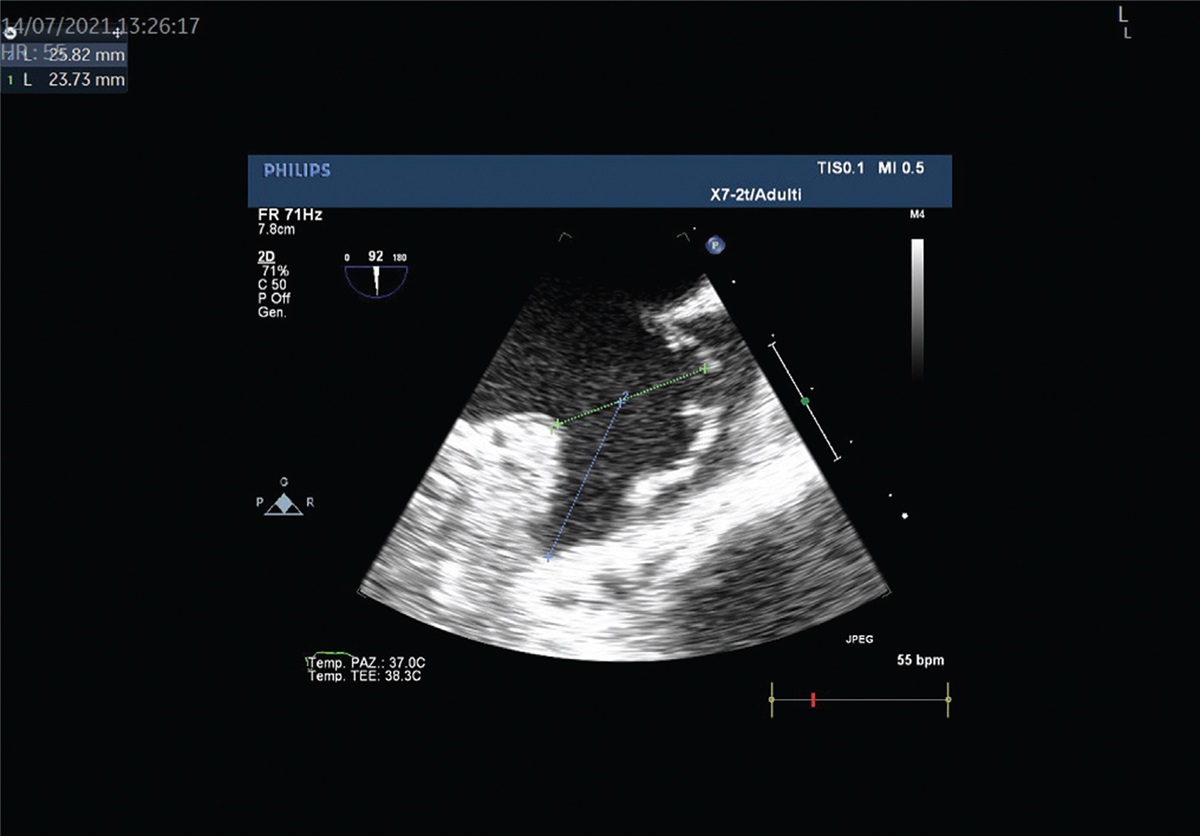
During the HYP test, occurrence of chest pain was variable and mild in intensity, and it did not preclude continuation of the protocol. The most common perception during the test was dizziness, without any serious side effects reported. Typical CFV flow pattern in vasospastic response at rest and peak HYP is presented in Fig. 2.
 Fig. 2:
Fig. 2: Coronary flow Doppler at the end of each test stage. CFV, coronary flow velocity; CFVR, coronary flow velocity reserve.
In six patients (15%) with RWMA, rest WMSI = 1 increased to WMSI = 1.14 after HYP (P < 0.001).
In the whole study group during HYP, no significant changes in mean CFV were observed despite an increase in DP. At individual patient analysis, a vasoconstrictor response CFV (HYP< rest) was present in half of the patients (21 patients, 52%) during HYP.
Exercise test results: endothelium-dependent reactivityHemodynamic data during HYP+EXE test are presented in Table 2, showing a rise in double product more than on HYP alone. During EXE test, 18 patients (45%) reached the predicted heart rate, while 22 (55%) patients complained of fatigue and had to stop before reaching the target heart rate. This represents a clinical situation that is characteristic for INOCA patients. HYP alone was less effective than HYP+EXE in inducing anginal pain (6/40, 15% vs. 10/40, 25%, P = 0.046), ST segment changes (6/40, 15% vs. 24/40, 60%, P < 0.001), and RWMA (6/40, 15% vs. 13/40, 32.5%, P = 0.008) (Fig. 3). In 13 patients with RWMA, rest WMSI = 1 increased to WMSI = 1.20 after HYP+EXE (P < 0.001).
 Fig. 3:
Fig. 3: Histogram showing the prevalence of different ischemia markers during HYP and HYP+EXE.
Adenosine test results: endothelium-independent vasodilatationADO test was performed in order to test adenosine-mediated (mostly endothelium-independent) vasodilation reactivity expressed as CFVR. Feasibility of ADO testing was 100%, with CFVR after ADO preserved in all patients. CFVR was 2.56 ± 0.39, and no patient showed a CFVR of 2.0 or less. No patient showed RWMA (rest WMSI = ADO WMSI = 1.0).
DiscussionIn this study, we have assessed the impairment of microvascular function by TTE Doppler measurements of CFV during combined HYP+EXE and ADO stress echocardiography tests in patients with INOCA. Our main findings are that dynamic CMD was frequently provoked with HYP and reflected as a decrease in CFV despite an increase in double product in the majority of patients; during EXE (after HYP), inducible ischemia was substantially more frequent than after HYP alone; ADO-mediated (endothelium-independent) vasodilation was preserved in all patients excluding significant structural CMD; and without any serious adverse events occurring, combined HYP+EXE test proved to be well tolerated and feasible with stress echocardiography.
This is the first study to our knowledge wherein microvascular functional testing was conducted entirely by noninvasive TTE Doppler CFV measurement methods.
Current diagnostic criteria for VSA imply the presence of clinical symptoms, signs of transient ischemia on ECG during chest pain episode, and the evidence of spontaneous or provoked coronary vasospasm. Although Japanese Circulation Society guidelines endorse invasive provocation testing using intracoronary acetylcholine as the current gold standard in patients with suspected VSA and ECG changes, they also recommend hyperventilation and exercise tests as valid nonpharmacological methods for provocative testing.14 The COVADIS guidelines have extended the number of indications for coronary provocation testing including clinical conditions such as INOCA, while also recommending hyperventilation as a noninvasive diagnostic tool for such testing.18
Normal CAG finding in patients with documented anginal symptoms and evidence of ischemia should initiate additional diagnostic testing in order to increase the yield of specific diagnosis in patients with INOCA as well as to elucidate INOCA endotypes, which could help to personalize treatment and prognosis.7
Given the availability, low cost, and safety of noninvasive provocative tests, they should be included in the diagnostic workup for INOCA, especially for patients who do not have access to invasive coronary diagnostic testing.
Considering the variable sensitivity of the hyperventilation ECG test (8--61.7%) in diagnosing VSA, more potent combinations of the stressors have been introduced.19
The effectiveness of accelerated exercise following mild hyperventilation testing has been shown to be equivalent to acetylcholine testing, a current gold standard.20 However, in order to introduce a noninvasive method to test coronary reactivity, more sensitive indicators of ischemia should be used. The utility of stress echocardiography was reported by Hirano et al.13 who used a combined hyperventilation-cold pressor echocardiography test with sensitivity of 91% and specificity of 90%. Extended research from the same group of authors further confirmed that severity and even the region of coronary spasm provoked by hyperventilation and cold pressor tests are identical to those induced by intracoronary injection of acetylcholine during CAG.8 Recently, the large study by Om et al.21 has demonstrated the safety and prognostic value of ergonovine echocardiography in the large group of 14 012 patients. The overall frequency of positive results was 15.3% (n = 2144) and most of these patients (99.6%) showed RWMAs.21 Moderate or severe dyssynergy was also present in 23% of INOCA patients in the Ciao Ischemia study.22 In our study, RWMA as an echocardiographic sign of ischemia was present in 15% of patients during HYP and in 32.5% during HYP+EXE. Subtle ECG changes were present in 15 and 60% of the patients during HYP and HYP+EXE, respectively.
Evaluation of microvascular impairment in coronary syndrome X patients was previously done by Galiuto et al.23 who found markedly lower TDE CFVR LAD values in women with syndrome X in comparison with controls, while our group has previously reported impairment of CFVR and global longitudinal strain values in women with cardiac syndrome X and slow coronary flow.11 Lower values of CFR measured invasively were also found in a cohort of INOCA patients.24 We studied microvascular function noninvasively by TDE, starting with hyperventilation testing for coronary and microvascular spasm provocation. CMD was further challenged with EXE for measurement of flow-dependent functional vasodilatation.16,17,19,20 We have examined CFV as the first sign in ischemic cascade and a sensitive marker of microvascular dysfunction.5 Earlier, Chauhan et al.25 have shown that in patients with syndrome X, both hyperventilation and mental stress associated with chest pain cause a significant reduction in coronary blood flow velocity in the absence of any significant changes in the diameter of the LAD. They have suggested that an increased oxygen demand in the presence of an impaired CFR resulting from a dynamic transient increased constriction of the microvasculature causes myocardial ischemia in these patients.25–27 Akasaka et al.28 reported significantly lower averaged peak coronary flow velocity values measured by thermodilution during hyperemia in patients with diffuse ergonovine induced vasospasm in comparison with cases of focal vasospasm. Micro-vessel impairment in patients with diffuse vasoconstriction could explain this reduced CFR. Our results are consistent with previously published data. Half of our patients (52%) had vasoconstrictive reaction on hyperventilation with reduced CFV. As all our patients had normal CAG, reduced CFV during HYP and later HYP+EXE is considered to be related to microvascular functional dysfunction. The employed approach does not separate an epicardial from a microvascular origin of coronary vasospasm in positive tests. However, none of our patients showed inducible ST segment elevation or multi segment or severe RWMA, which are more suggestive of transmural ischemia and epicardial artery vasospasm. Both forms of vasospastic phenotype have similar therapeutic implications. However, when differentiation between epicardial and microvascular vasospasm is deemed clinically important, referral to cardiac catheterization may be warranted.
Interestingly, CFVR values obtained during adenosine infusion were preserved in all patients, reflecting normal mostly endothelial-independent vasodilatation, thereby excluding significant structural changes. Patient populations with angina with no obstructive CAD are very heterogeneous, and results of functional testing need to be put in the framework of clinically available information.29 In the present study, we included only patients with strong (Class 1) indication for vasospasm testing according to the recent guidelines and recommendations.6,14 The normal response to adenosine outlines the importance of vasospasm testing in patients without a diagnosis after standard assessment of coronary flow velocity reserve as suggested by current guidelines. These patients still remain without a positive diagnosis, since a normal CFR cannot exclude a functional vasospastic coronary disease.
Clinical implicationsDoppler TTE as a technique could not be considered as a substitute for invasive dedicated techniques that can directly assess microvascular function, flow, and resistance in all coronary arteries, but could be useful in providing additional information about coronary pathophysiology, considering the broad availability and low cost, feasibility, and safety of the method.
With this simple test, we can reproduce usual situations that provoke anginal pain and discomfort in INOCA patients and have insight into the possible mechanism responsible for it. Dynamic CMD is a frequent endotype and a potential actionable therapeutic target in these patients, but the clinical recognition remains difficult if only invasive means are used.
Study limitationIn order to assess microvascular function, we have used noninvasive Doppler echocardiographic measurements. We did not compare them with the ‘gold standard’ invasive measurements of CFV with acetylcholine provocation. The lack of invasive validation is an important limitation, but the hyperventilation-exercise test has already been compared with an acetylcholine test. Hirano et al.13 evaluated 43 patients with suspected VSA with hyperventilation stress echocardiography and found a 91% sensitivity of hyperventilation echocardiography for the detection of coronary vasospasm against intracoronary acetylcholine testing with CAG. Our findings are consistent with previous validation studies showing that hyperventilation is an efficient test for coronary vasospasm, regional wall motion is clearly more sensitive than ECG changes, and exercise can further enhance the sensitivity of hyperventilation alone.
The timing of positivity is in the 5’ after the end of HYP, but for practical reasons EXE was started at 1’ after the end of HYP, and therefore the HYP+EXE positivity could still be due to the delayed vasoconstrictive effects of HYP rather than to EXE.30 Epicardial coronary vasospasm is a localized phenomenon and 2D echo monitoring allows the detection of regional changes in all coronary territories. However, coronary microcirculatory abnormalities are more diffuse, and LAD can serve as an index vessel reflecting the condition of the entire microcirculation, in the same way as it is recommended for LAD in structural (not functional) coronary microcirculatory disease. Coronary spasm of coronary microcirculation is a diffuse phenomenon, affecting equally LAD and non-LAD territory, as previously shown.31
Several parameters might be measured from the Doppler tracing of coronary flow. We have used peak/basal diastolic flow as the easiest to be obtained, the most reproducible and with the closest correlation to coronary perfusion reserve measured with PET.32
Small sample size is an important limitation of this study. This is a pilot study, and needs a prospective confirmation with a large-scale study. SESPASM (acronym for Stress Echo for coronary vasoSPASM detection) is one of the 12 protocols on the large international, multicenter, prospective, stress echo 2030 platform that covers a broad spectrum of cardiovascular disease. The projected sample size in the SESPASM project of stress echo 2030 protocol is 513 patients collected on a multicenter basis and followed up for 5 years.33 We hope that this and further large-scale studies will confirm our observations.
ConclusionIn patients with INOCA and clinical suspicion of coronary vasospasm, HYP+EXE is a more powerful ischemia inducer than HYP alone. A reduction of CFV is elicited by HYP in about one in two patients, in absence of a reduction of CFVR after ADO. A dynamic CMD is frequent in INOCA patients, and can be appropriately unmasked noninvasively with stress echocardiography, when RWMA and CFV are combined with vasoconstrictive stressors such as HYP and EXE.
AcknowledgementsThis study was partially supported by the grant of the Ministry of Education and Science of the Republic of Serbia (grant number 41022).
Conflicts of interestThere are no conflicts of interest.
References 1. Camici PG, D’Amati G, Rimoldi O. Coronary microvascular dysfunction: mechanisms and functional assessment. Nat Rev Cardiol 2015; 12:48–62. 2. Noel Bairey Merz C, Pepine CJ, Walsh MN, Fleg JL. Ischemia and no obstructive coronary artery disease (INOCA): developing evidence-based therapies and research agenda for the next decade. Circulation 2017; 135:1075–1092. 3. Pries AR, Badimon L, Bugiardini R, et al. Coronary vascular regulation, remodelling, and collateralization: mechanisms and clinical implications on behalf of the working group on coronary pathophysiology and microcirculation. Eur Heart J 2015; 36:3134–3146. 4. Sorop O, Merkus D, De Beer VJ, et al. Functional and structural adaptations of coronary microvessels distal to a chronic coronary artery stenosis. Circ Res 2008; 102:795–803. 5. Knuuti J, Wijns W, Saraste A, et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Hear J 2020; 41:407–477. 6. Kunadian V, Chieffo A, Camici PG, et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International. Eur Heart J 2020; 41:3504–3520. 7. AlBadri A, Bairey Merz CN, Johnson BD, et al. Impact of abnormal coronary reactivity on long-term clinical outcomes in women. J Am Coll Cardiol 2019; 73:684–693. 8. Hirano Y, Uehara H, Nakamura H, et al. Diagnosis of vasospastic angina: comparison of hyperventilation and cold-pressor stress echocardiography, hyperventilation and cold-pressor stress coronary angiography, and coronary angiography with intracoronary injection of acetylcholine. Int J Cardiol 2007; 116:331–337. 9. Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021; 78:e187–e285. 10. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging 2015; 16:233–271. 11. Jovanovic I, Tesic M, Giga V, et al. Impairment of coronary flow velocity reserve and global longitudinal strain in women with cardiac syndrome X and slow coronary flow. J Cardiol 2020; 76:1–8. 12. Cortigiani L, Ciampi Q, Lombardo A, Rigo F, Bovenzi F, Picano E. Age- and gender-specific prognostic cutoff values of coronary flow velocity reserve in vasodilator stress echocardiography. J Am Soc Echocardiogr 2019; 32:1307–1317. 13. Hirano Y, Ozasa Y, Yamamoto T, et al. Hyperventilation and cold-pressor stress echocardiography for noninvasive diagnosis of coronary artery spasm. J Am Soc Echocardiogr 2001; 14:626–633. 14. Intervention C. Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ J 2014; 78:2779–2801. 15. Yasue H, Nagao M, Omote S, et al. Variant form of angina induced by hyperventilation and Tris-buffer infusion. Circulation 1978; 58:56–62. 16. Kapilevich LV, Kologrivova VV, Zakharova AN, Mourot L. Postexercise endothelium-dependent vasodilation is dependent on training status. Front Physiol 2020; 11:1–8. 17. Rehan R, Weaver J, Yong A. Coronary vasospastic angina: a review of the pathogenesis, diagnosis, and management. Life (Basel) 2022; 12:1124. 18. Ong P, Camici PG, Beltrame JF, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol 2018; 250:16–20. 19. Nakao K, Ohgushi M, Yoshimura M, et al. Hyperventilation as a specific test for diagnosis of coronary artery spasm. Am J Cardiol 1997; 80:545–549. 20. Sueda S, Fukuda H, Watanabe K, et al. Usefulness of accelerated exercise following mild hyperventilation for the induction of coronary artery spasm: comparison with an acetylcholine test. Chest 2001; 119:155–162. 21. Om SY, Yoo SY, Cho GY, et al. Diagnostic and prognostic value of ergonovine echocardiography for noninvasive diagnosis of coronary vasospasm. JACC Cardiovasc Imaging 2020; 13:1875–1887. 22. Reynolds HR, Picard MH, Spertus JA, et al. Natural history of patients with ischemia and no obstructive coronary artery disease: the CIAO-ISCHEMIA Study. Circulation 2021; 144:1008–1023. 23. Galiuto L, Sestito A, Barchetta S, et al. Noninvasive evaluation of flow reserve in the left anterior descending coronary artery in patients with cardiac syndrome X. Am J Cardiol 2007; 99:1378–1383. 24. Ford TJ, Yii E, Sidik N, et al. Ischemia and no obstructive coronary artery disease: prevalence and correlates of coronary vasomotion disorders. Circ Cardiovasc Interv 2019; 12:e008126. 25. Chauhan A, Mullins PA, Taylor G, Petch MC, Schofield PM. Effect of hyperventilation and mental stress on coronary blood flow in syndrome X. Br Heart J 1993; 69:516–524. 26. Kaski JC, Crea F, Nihoyannopoulos P, Hackett D, Maseri A. Transient myocardial ischemia during daily life in patients with syndrome X. Am J Cardiol 1986; 58:1242–1247. 27. Kaski JC, Maseri A, Vejar M, Crea F, Hackett D, Halson P. Spontaneous coronary artery spasm in variant angina is caused by a local hyperreactivity to a generalized constrictor stimulus. J Am Coll Cardiol 1989; 14:1456–1463. 28. Akasaka T, Yoshida K, Hozumi T, et al. Comparison of coronary flow reserve between focal and diffuse vasoconstriction induced by ergonovine in patients with vasospastic angina. Am J Cardiol 1997; 80:705–710. 29. Foa A, Canton L, Bodega F, et al. Myocardial infarction with nonobstructive coronary arteries: from pathophysiology to therapeutic strategies. J Cardiovasc Med 2023; 24: (suppl 2): e134–e146. 30. Morales MA, Reisenhofer B, Rovai D, Moscarelli E, Distante A, L’abbate A. Hyperventilation-echocardiography test for the diagnosis of myocardial ischaemia at rest. Eur Heart J 1993; 14:1088–1093. 31. Sun H, Fukumoto Y, Ito A, Shimokawa H, Sunagawa K. Coronary microvascular dysfunction in patients with microvascular angina: analysis by TIMI frame count. J Cardiovasc Pharmacol 2005; 46:622–626. 32. Saraste M, Koskenvuo JW, Knuuti J, et al. Coronary flow reserve: measurement with transthoracic Doppler echocardiography is reproducible and comparable with positron emission tomography. Clin Physiol 2001; 21:114–122. 33. Picano E, Ciampi F, Cortigiani L, et al. The Stress Echo 2030 Study Group of the Italian Society of Echocardiography and Cardiovascular Imaging (SIECVI). Stress Echo 2030: the Novel ABCDE-(FGLPR) Protocol to Define the Future of Imaging J. Clin Med 2021; 10:3641.
留言 (0)