
記住我


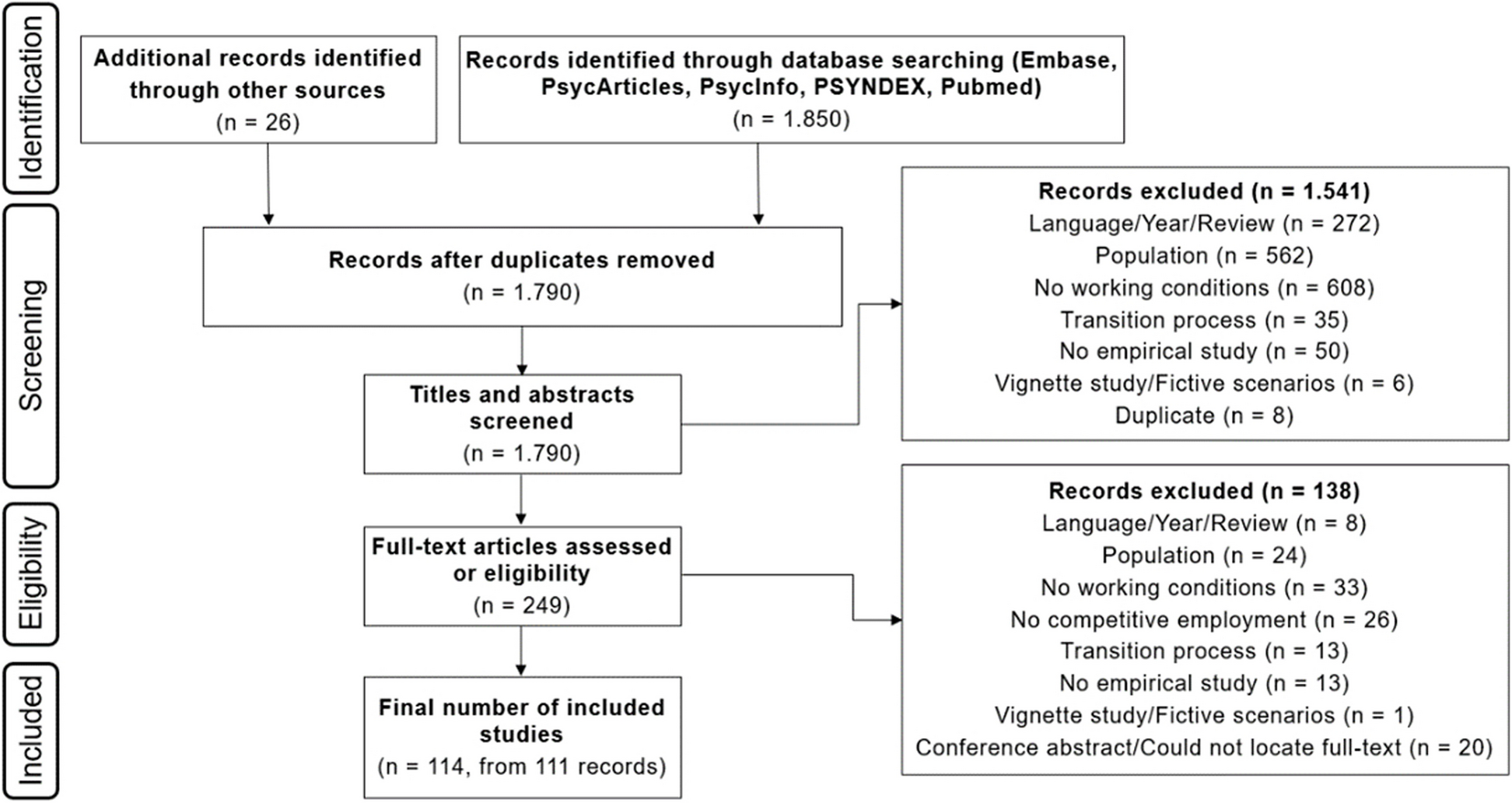


From n = 1105 articles returned from database screening, n = 20 studies were deemed relevant to include in the final synthesis. The flow of articles through the screening steps is illustrated in Fig. 2. Extracted data is presented in Table 3. The table and synthesis are organised as follows: studies with biological measures (n = 3), longitudinal survey studies with analyses (n = 5), cross-sectional survey studies with analyses (n = 2), and cross-sectional survey studies with descriptive statistics (n = 10). In our synthesis, we do not stratify by recency, animal species, or country for the following reasons: All articles were published since 2002. Thirteen of these were published within the last 4 years. All studies involved dogs except for one study that involved cats [27]. All settings were located in the USA, Australia, and Europe.
Fig. 2
PRISMA Flow Diagram. WoS: Web of science, T: Titles, A: Abstract
Table 3 Overview of included studies (all studies involve dogs except for one involving cats which is labelled)Healthcare settings were mostly hospitals or medical centres, seven of which involved children’s hospitals or paediatric wards (one of which was a psychiatric ward for adolescents) [31, 33, 36, 37, 41, 43, 46]. Two studies specify community care/hospice [40, 42]. Apart from the two latter studies, all studies at least implied assessment of nurses and physicians (thirteen explicitly mentioned this). Some studies also considered allied and ancillary healthcare staff [30,31,32,33,34,35,36,37,38,39,40,41, 43, 44]. In total, ~ 1,000 members of healthcare staff participated across the twenty studies.
Regarding exposure/intervention, n = 6 studies considered reaction to staff AAA, n = 11 studies considered reaction to patient AAA, n = 3 studies considered reaction to communal animals [27, 42, 44]. Regarding outcomes, perceptions, attitudes, concerns, emotional well-being, fatigue, burnout, physical discomfort and pain, cortisol, noradrenaline, adrenaline and IgA were assessed.
Biological measuresThree studies assessed cortisol in serum or saliva [28,29,30]. Machova et al. (2019), using a within subjects design, observed decreased cortisol in some staff after taking a break with the dog but not after taking a break without the dog or after no break (Fig. 3) [29]. Baseline cortisol was measured at the same time every day (10:00am) and 50 min later (within which the break occurred). The reduction was observed in n = 9 nurses working at the department of internal medicine and long-term care but not in n = 11 nurses working in physical medicine; the authors put forward as explanation that these participants started with already low cortisol values. Barker et al. (2005) assessed cortisol at several time points following 5 min rest with dog, 20 min rest with dog, 20 min rest without dog with the interventions starting at either 1:00 pm or 3:00 pm. They observed decreased cortisol after at least 45 min in all three groups but no changes in noradrenaline, adrenaline, salivary IgA, or lymphocyte proliferation [30]. Decreased cortisol was observed at 15 min post intervention for both 20 min rest with and without dog but not 5 min with dog. Of course, the time since beginning of intervention is different for these measurements (e.g., 20 min + 15 min vs 5 min + 15 min); thus, conclusions about group differences cannot be made. Kline et al. (2020) assessed cortisol across a work shift that included either 5 min with dog (n = 43), 5 min colouring a mandala (n = 40), or no intervention (n = 39) [28]. Using a mixed methods repeated measured ANOVA, they observed time x group interactions suggesting greater decrease in cortisol at the end of shift in the 5 min with dog group compared to other groups. Of note, differential effects for subjective stress (and compared to cortisol) were observed insofar as there was no clear effect on subjective stress as measured with the modified Perceived Stress Scale but there was when using a visual analogue scale. Also of interest, a potential rise in subjective stress associated with colouring was observed, possibly attributable to the frequently expressed disappointment when assigned to colouring rather than the dog intervention.
Fig. 3
Healthcare staff interactions with support animals that were investigated. A Designated time alone with dog (with handler present) [28, 29]; B Designated time with dog (with handler and possibly others present) [30,31,32,33,34,35]; C Working alongside facility (full-time) animals including dogs and cats [27, 36, 42]; D Working alongside dogs visiting patients
Longitudinal studies with survey analysesAll five studies used a pre- vs post- design. Two studies assessed responses to AAA for staff [31, 32] and three studies to AAA for patients [33,34,35]. Regarding staff-specific dogs, Gerson et al. (2023) examined the effect of a “Medical Dog Office Hours Program” of maximum 10 × 1-h sessions over 1–2 months and Etingen et al. (2020) adopted a similar procedure with a maximum of 20 × 1-h sessions over 3 months [31, 32]. In both cases frequency and duration of participation differed by participant availability. Also in both cases, the impact of staff AAA was considered beneficial with improved mood and decreased tiredness. In the latter study, there was no clear effect on perception of burnout except for less exhaustion when dealing with patients [32]. The latter program was also rated as positive (not asked in the former) [32].
Regarding responses to AAA for patients, all three studies observed improved mood in staff in different adult units compared to baseline [33,34,35]. Ginex et al. (2018) also observed decreased feeling of stress but no change in feelings of burnout or compassion in an oncology unit [34]. Marcus et al. (2012) also observed improvements in feelings of stress and fatigue in a chronic pain unit [35]. In contrast to their findings on an adult psychiatric unit, Brown et al. (2020) did not observe a change in mood on an adolescent psychiatric unit [33]. Ginex et al. (2018) took post-measurements at least six weeks after full implementation of an AAA program that involved visits on four days per week [34]. Marcus et al. (2012) conducted a 2-month long study of AAA visits to their waiting room for 2-h on 2 days per week [35]. Brown et al. (2020) conducted a 4-month long study of weekly dog visits. In all cases, it is unclear how much interaction staff had with the dogs prior to starting the study or exact the time difference between pre- and post- measurements for each member of staff [33]. In the study by Marcus et al. [35], all staff reported enjoying dog visits.
Cross-sectional surveys—analysesTwo studies conducted cross-sectional survey analyses. Moody et al. (2002) compared expectation vs experience of AAA for patients and Jensen et al. (2021) compared working with vs without a facility dog for patients [36, 37]. Both studies were conducted at a children’s hospital. Moody et al. (2002) found that the work environment and program acceptance was rated higher by those who experienced AAA for patients (measured 12 weeks after program start; unclear how long staff actually experienced AAA) [37]. Jensen et al. [36] found that those staff working with a facility dog had higher perceived personal accomplishment and job satisfaction and better mood. There were no differences in feelings of fatigue or perceptions of co-workers, workplace support, or anxiety [36].
Cross-sectional surveys—descriptiveComprising ten studies, this was the most common study design. One study concerned AAA for staff [38]. Two studies included communal animals (psychiatric ward with cats and community care for mentally ill with dog) [27, 42]. The remaining seven studies concerned responses to patient AAA [39,40,41, 43,44,45,46]. All studies indicate positive perception or experience of AAA. In particular, and irrespective of whether AAA was primarily directed towards staff or patients, there was agreement that AAA was beneficial against stress [38,39,40, 42,43,44]. In some studies, staff members expressed excitement about the opportunity to interact with dogs [39, 44]. As examples of widespread agreeableness with AAA: Caton et al. (2021) find over 90% of staff participants acknowledged a positive impact on staff morale, program satisfaction, and stress reduction and 96% expressed a desire for the program to continue [38]; Pruskowski et al. (2020) find 95% of rehabilitation staff consider their mood is better [39]; Machova et al. (2020) find 92% of staff participants consider that the dogs provide them with emotional support [40]; Wagner et al. (2019) find 100% of staff participants had positive feelings about the cats and 84% reported a positive impact on their work satisfaction [27]; Uglow et al. (2019) find 100% of staff participants consider AAA to be very worthwhile [41]. The lowest observed agreement or benefit of AAA was still 54% in the study by Caprilli et al. (2006) [46]. Indeed, in one study, staff even also reported missing the dog when it was not present [44]!
There were few negatives and in only a few studies. Specifically, some individual expressed concerns regarding fear of dogs, potential dog bites, cleanliness issues, disease transmission, and added stress [42, 44,45,46]. Caprilli et al. (2006) reported that 16% of staff expressed fear of dog biting or disease transmission, but there was no change in infection rates after the introduction of dogs, and no reports of biting or other problems with the dogs [46]. This is not to say that these are the only studies that asked about negative experiences or concerns. For instance, Machova et al. (2020) found no concerns regarding contamination of beds or rooms and this study was conducted in a nursing/retirement home and home hospices following AAA visits [40].
留言 (0)