
記住我

What is known about the topic?
Early detection of PSD can diminish the length of stay in hospitals, improve quality of life, and reduce disability and mortality rates. There is still a large gap between evidence and clinical practice for PSD screening, prevention, and management, which requires improvement in hospitals. It is important to enhance nurses’ understanding, knowledge, and skills in PSD management to provide the best care for patients.What does this article add?
Nurses’ training concerning best practice compliance for the prevention, screening, and management of PSD should be continuous. Lack of knowledge and attitudes toward PSD among nurses were the most relevant barriers to evidence-based practice for screening, prevention, and management of PSD in our hospital. This study provides an example of effective strategies to improve evidence-based practice and nursing care quality through tailored, multifaceted strategies for PSD, including training and audit and feedback interventions, which can be implemented in more hospitals in the future. IntroductionA stroke occurs when the blood supply to the brain is blocked or a blood vessel ruptures causing bleeding, and is classified as ischemic or hemorrhagic (respectively) depending on the nature of the insult to blood vessels.1 Stroke is the second leading cause of death globally after ischemic heart disease, but it has been the leading cause of death in China in recent years.2 The China Stroke Statistics 2019 report estimated that China's mortality rate of cerebrovascular diseases was 149.49 per 100 000, with 1.57 million deaths in 2018, constituting nearly one-third of all stroke deaths worldwide. Stroke has imposed a huge burden of disease on China's health care system.3
The most common emotional disorder after a stroke is depression, especially after acute ischemic stroke. About one-third of stroke survivors may suffer from depression at any stage, leading to increased morbidity and mortality, as well as restricting rehabilitation, reducing the quality of life, and possibly prolonging the duration of stay in hospital.4 Common symptoms of poststroke depression (PSD) are loss of interest, restlessness, an increase or decrease in sleep time, behavioral changes, feeling useless, distraction, and suicidal thoughts.5 If not recognized and treated in a timely manner, these conditions can lead to worse long-term outcomes.6
Relevant data show that the prevalence of depression in stroke survivors is higher than that in the general population, but the mechanisms of PSD are not fully understood. In addition, clinical medical staff often lack knowledge surrounding the symptoms and treatment of PSD. As a result, misdiagnosis, delayed treatment, and lack of treatment of PSD are common in clinical settings.7 The ability to recognize patients at high risk of PSD would enable the detection of depression symptoms early, notably in the first few months when the majority of neurological and functional recovery occurs.8 The reported risk factors for PSD include being female, age, living alone, prior history of stroke, presence of cognitive impairment, functional dependence, and history of depression before stroke.9–11 The most significant risk factors for PSD may be physical disability and having a history of depression.12 In China, the nursing management of PSD often depends on the nurses’ level of experience and subjective judgment rather than the prevention and management of PSD through the use of evidence-based strategies. Therefore, it is a priority to develop and implement evidence-based approaches to improve the screening, prevention, and management of PSD.
Currently, several guidelines and JBI evidence summaries have been developed to assist nurses in the screening, prevention, and management of PSD in patients with stroke.4,12–14 The 2019 update of the Canadian Stroke Best Practice Recommendations (CSBPR) states that all people who have experienced a stroke should be screened for PSD, particularly given the high prevalence and lack of timely treatment of PSD.12 Various screening tools are available to operationally detect PSD. The JBI evidence summary on PSD screening recommends that poststroke patients are screened for depression using the Center of Epidemiological Studies Depression Scale, the Hamilton Depression Rating Scale (HDRS), and the Patient Health Questionnaire-9.15 These instruments have high sensitivity and specificity,4 and the HDRS is commonly used. Due to the large stroke population in China, a consensus of Chinese experts recommends the use of simple questionnaires initially to screen for depression, such as the four questions in 90 seconds. For this method, if the patient's answers to all four questions are positive, the depressive symptom assessment scale is used to further evaluate the severity of depression.16
Early prevention and intervention may decrease the incidence of PSD, improve the quality of life of patients, and reduce disease recurrence.17 For example, antidepressants, specifically selective serotonin re-uptake inhibitors, can effectively decrease the occurrence of PSD and promote the recovery of neurological function.10,18 However, the 2019 update of the CSBPR does not recommend the use of antidepressants for prevention in all people who have suffered a stroke, as the ratio of benefits to risks is uncertain. Psychotherapy, such as cognitive behavioral or problem-solving therapy, as monotherapy and first-line therapies are also appropriate in the prevention and treatment of PSD.12 In addition, a JBI evidence summary on exercise for PSD recommended that an individualized exercise program, emphasizing low-to-moderate aerobic exercise and progressive resistance exercise, be developed for poststroke patients who have no exercise contraindications.19 Other recommended interventions include music, deep breathing, and motivational interviews. However, these strategies lack sufficient evidence and need further research.12,20
PSD is a serious but easily overlooked problem for stroke survivors and its valid management is significant to improve their quality of life. Nurses should enhance their understanding, knowledge, and skills in PSD management to provide the best care for patients. The aim of this project was to undertake an evidence implementation project to improve the screening, prevention, and management of PSD in a neurology ward of the Fifth Affiliated Hospital of Zunyi Medical University, China. The audit was based on the JBI Practical Application of Clinical Evidence System (PACES) software and the Getting Research into Practice (GRiP) tools.14 If successful, this project will be extended to patients with stroke in more hospitals across China.
Aims and objectivesThe objective of this study was to improve adherence to evidence-based practice for the screening, prevention, and management of patients with PSD admitted to the neurology ward of the Fifth Affiliated Hospital of Zunyi Medical University, China.
Specifically, the aims of the study were to:
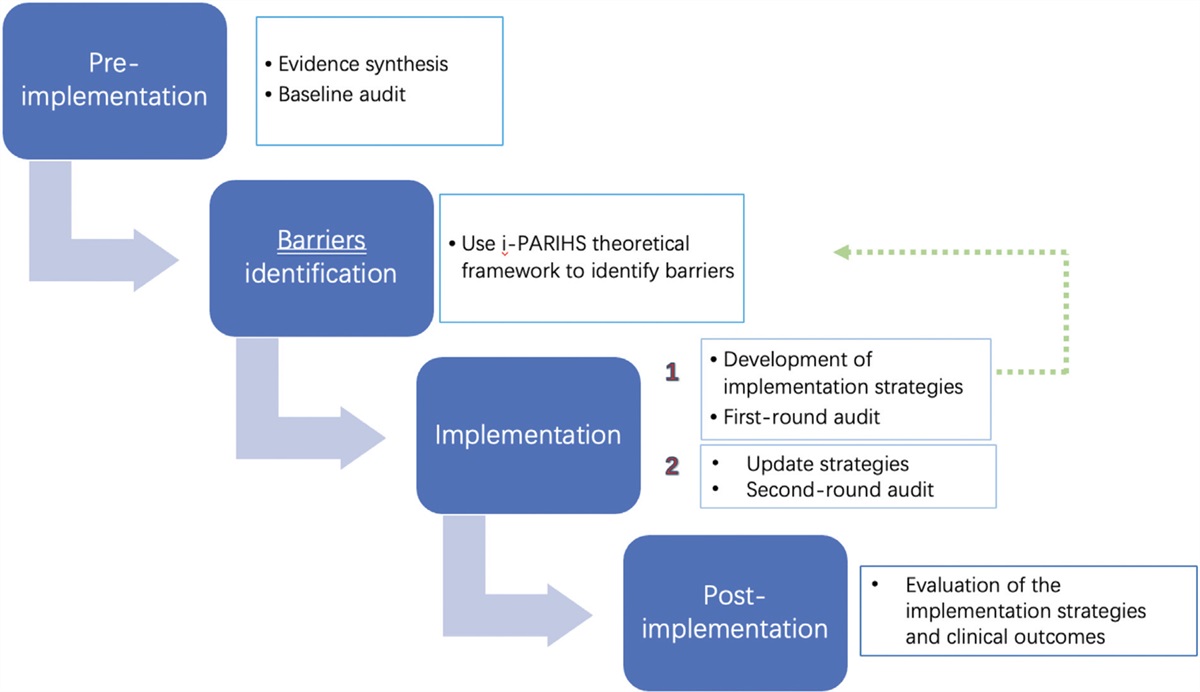
i) To design and conduct a clinical audit of PSD screening, prevention, and management practices. ii) To identify barriers and facilitators to improving compliance and develop strategies to address areas of noncompliance. iii) To raise clinical awareness and improve compliance with the best practice recommendations for screening, prevention, and management of PSD. iv) To evaluate the feasibility and potential effectiveness of the implementation project on compliance with the best practice recommendations for the screening, prevention, and management of PSD. MethodsThe project was based on the JBI Evidence Implementation Framework,14 which consists of seven stages, including first, identification of practice area for change; second, engaging change agents; third, assessment of context and readiness to change; fourth, review of practice against evidence-based audit criteria (baseline audit); fifth, implementation of changes to practice; sixth, reassessment of practice (follow-up audit); and seventh, consideration of the sustainability of practice changes. The project utilized the JBI PACES software and its GRiP audit and feedback tools. The project was undertaken in three phases from January to June 2021:
i) Phase 1: Establish a team for the project and conduct a baseline audit based on criteria informed by the evidence. ii) Phase 2: Analyze the results of the baseline audit and develop and implement strategies to address issues concerning noncompliance that were identified during the baseline audit. iii) Phase 3: Complete a subsequent audit to evaluate the results of interventions implemented to improve practice and identify future practice problems to be solved in follow-up audits. SettingThe current evidence implementation project was undertaken in a 56-bed neurology ward of the Fifth Affiliated Hospital of Zunyi Medical University, Zhuhai, China. The hospital is run by 17 nurses and nine doctors and receives approximately 1000 people with stroke every year, with over 800 admissions in the neurology ward where this study was undertaken.
Phase 1: Team establishment and baseline auditAll relevant stakeholders, including patients and project team members, were engaged in this project. From January 1 to February 28, 2021, we established a project team, determined the setting and sample size, and then conducted a baseline audit. The project team consisted of six members, including a project leader (a professor from the School of Nursing of Zunyi Medical University and a senior leader at the Evidence-based Practice in Nanfang Nursing Centre), a nursing director, a head nurse and a professional nurse (both from the neurology ward), and two postgraduate students. Each team member had their own roles and responsibilities. The project leader (N.L.) was involved in designing and planning the project. The director of nursing provided corresponding policy and organizational support during the implementation of the project. The head nurse and a professional nurse ensured the smooth implementation and supervision of the project in the neurology ward. Lastly, the two postgraduate students (J.T. and B.D.) were involved in data collection.
The audit criteria used in this project are based on three JBI evidence summaries15,19,21 and two guidelines.10,12 The audit design team conducted a meeting prior to the implementation of the project and devised the sample size and methods to measure compliance with best practices for each audit criterion (shown in Table 1).
Table 1 - Audit criteria and methodsa Audit criterion Sample The method used to measure % compliance with best practice recommendations (1) All patients who have suffered a stroke are screened for depression upon admission by using a validated depression scale. Baseline: 87 patientsPSD, poststroke depression.
aIf there was no evidence of documentation or if the information was unknown, then the response defaulted to ‘No’.
The baseline audit included 87 patients who met the diagnostic standards defined by the 4th National Colloquium on Cerebrovascular Diseases, had a stroke diagnosis confirmed by CT or MRI of the brain, were older than 18 years, and met the diagnostic criteria for stroke. Out of 17 nurses who typically worked in the neurology ward, 14 nurses participated in the study audits and training (82%). The three nurses who did not participate were away during this period due to maternity leave or studying abroad. The nurses were briefed on the program overview and signed an informed consent form. To measure compliance with each audit criterion, baseline data were collected by reviewing nursing records and/or interviewing/surveying patients/caregivers and/or reviewing nursing training attendee lists.
Phase 2: Design and implementation of strategies to improve practice (Getting Research into Practice)Phase 2 of this project was conducted from March 1 to April 30, 2021. The baseline audit results were reviewed and discussed with nurses using the JBI GRiP framework approach.14 A brief brainstorming meeting was convened with all working group members to identify barriers to the implementation of each criterion. Based on the identified barriers, the project team determined appropriate strategies and actions to increase compliance. Finally, the project team was involved in developing an implementation strategy to overcome the identified barriers.
Phase 3: Follow-up audit post implementation of change strategyThe purpose of the follow-up audit was to assess whether there was improvement in compliance with best practices and to determine what areas needed to be improved in the future. A follow-up audit was conducted using the same criteria and methods as for the baseline audit from May 1 to June 30, 2021. The sample consisted of 75 patients with stroke and 14 nurses in the neurology ward during this period.
AnalysisResults data on changes in compliance were measured using descriptive statistics embedded in JBI PACES in the form of percentage changes from baseline.
Ethical considerationsEthical approval for this study was acquired from the Fifth Affiliated Hospital of Zunyi Medical University Ethics Committee [approval number (2021) 2021ZH0104].
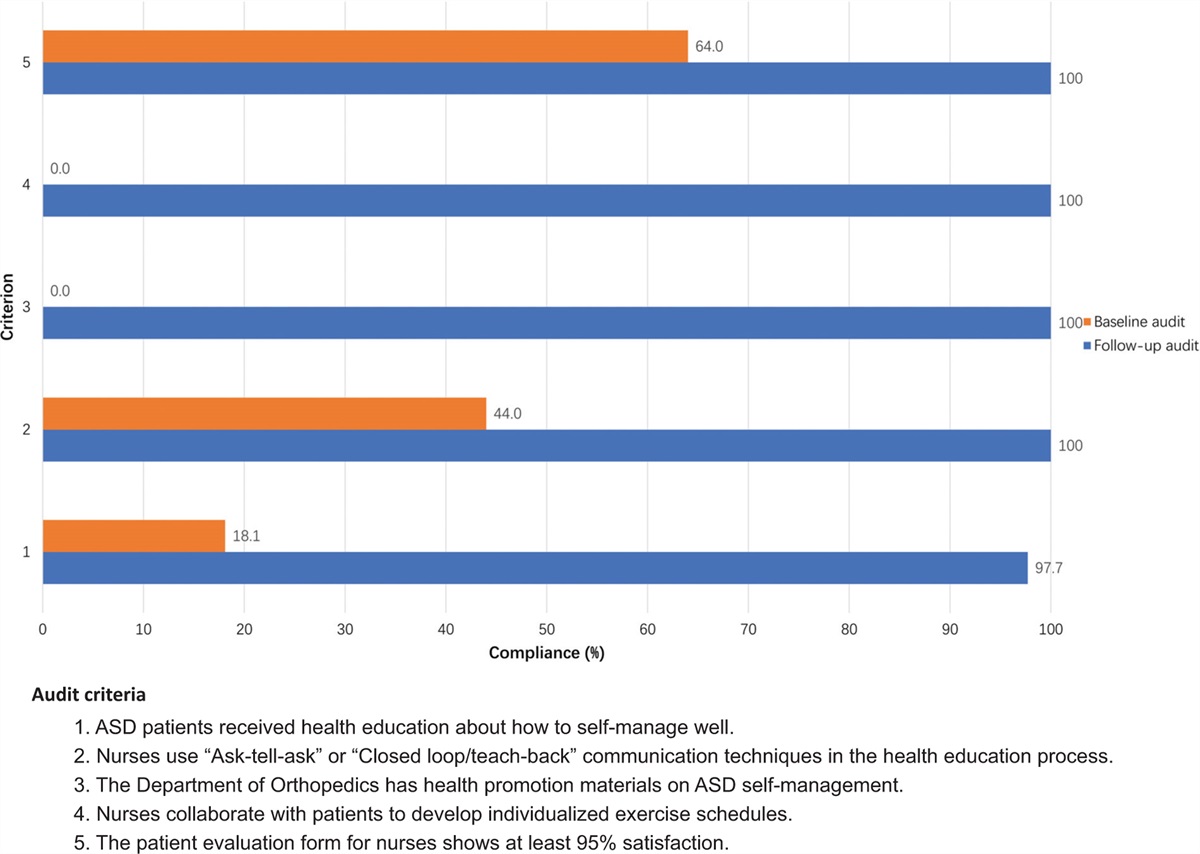
Results Phase 1: Baseline auditThe baseline data included a total of 87 patients with stroke (criteria 1–5) and 14 nurses in the neurology ward (criterion 6) (Fig. 1). Baseline compliance with criterion 2 was 10.3%, indicating that 9 out of 87 patients engaged in individually structured exercise programs. Five out of 87 patients (5.7%) received psychotherapy as per criterion 3. For criterion 4, 43 out of 87 patients (49.4%) received more company and encouragement from their family, friends, or colleagues. Furthermore, performance in the remaining criteria, 1, 5, and 6 was 0%. These results revealed that nurses and patients had never obtained training or education for the screening, prevention, and management of PSD. In addition, no patients with stroke responded to having been screened for depression upon admission.
 Figure 1:
Figure 1: Compliance with best practice for audit criteria in follow-up audit compared to baseline audit (%). Criteria legend: (1) All patients who have suffered a stroke are screened for depression upon admission by using a validated depression scale (baseline: 87 of 87 samples taken; follow-up: 75 of 75 samples taken). (2) Stroke patients without contraindications to exercise should engage in individually structured exercise programs that emphasize low to moderate intensity aerobic and progressive resistance exercises (baseline: 87 of 87 samples taken; follow-up: 75 of 75 samples taken). (3) According to the psychological state of patients, develop an individualized psychological intervention program (such as cognitive behavioral therapy or problem-solving therapy, baseline: 87 of 87 samples taken; follow-up: 75 of 75 samples taken). (4) Stroke patients have received more social support, company, and encouragement from family, friends, and colleagues (baseline: 87 of 87 samples taken; follow-up: 75 of 75 samples taken). (5) Patients or caregivers have received education on the screening, prevention, and management of poststroke depression (baseline: 87 of 87 samples taken; follow-up: 75 of 75 samples taken). (6) All staff have received education and training related to screening, prevention, and management of poststroke depression (14 of 14 samples taken).
The knowledge questionnaire on PSD screening, prevention, and management completed by 14 nurses before the training revealed the average score was 62.5/100 (see Table 2).
Table 2 - Comparison of nurses’ awareness of poststroke depression knowledge before and after the implementation of evidence Group Sample size Total score PSD test score t value p value Baseline audit 14 100 62.50 ± 7.53 −13.93 <0.001 Follow-up audit 14 100 86.07 ± 5.26HDRS, Hamilton Depression Rating Scale; PSD, poststroke depression.
Following the review of the baseline patient nursing record audit data, five barriers were identified by the nurses, and recommended strategies to address these barriers were agreed to be implemented (Table 3). The major barriers were that there was no formal PSD education handbook, screening tools, or management methods currently available in the neurology ward. In addition, nurses were busy and tended to neglect the psychological aspects of stroke patients, as well as lacking knowledge about PSD. To address these barriers, we undertook a series of measures to enhance the department's compliance in the screening, prevention, and management of PSD. An education package focusing on the six audit criteria was developed and included the following:
i) Using the best practice recommendations, the project leader conducted several formal 30–40 minute education sessions for the 14 nurses who agreed to participate. The training content included PowerPoint presentations and paper-based reference documents on PSD screening, prevention, and management. ii) A knowledge questionnaire with questions focusing on the screening, prevention, and management of PSD was developed to assess the ability of nurses to acquire knowledge. It included the symptoms of PSD, screening period, screening tools, risk factors, knowledge of prevention and treatment methods, etc. (see Appendix 1, https://links.lww.com/IJEBH/A133). iii) Our team compiled a patient education pamphlet after consulting PSD-related books and guidelines, focusing on the definition, risk factors, common symptoms, screening, prevention, and treatment of PSD, to improve patients’ understanding of PSD. Table 3 - Getting Research into Practice matrix Barrier Strategy Resources Outcomes (1) Lack of standardized depression screening tools Search for and collect depression screening tools for stroke patients “Four questions in 90 seconds”HDRS, Hamilton Depression Rating Scale; PSD, poststroke depression.
The following two scales for PSD screening were agreed to be used:
i) The Chinese version of the “Four questions in 90 seconds” was a short screening tool16; if the result of the “Four questions in 90 seconds” was positive, then a more detailed screening tool was to be used (see below). ii) The Chinese version of the HDRS16 is a more detailed screening tool for PSD that was used if the “Four questions in 90 seconds” was positive. The validity of HDRS ranges from 0.65 to 0.90.16 Please note, these materials are available in Chinese; please contact the first author if required. Phase 3: Follow-up auditA comparison of the first audit cycle and postimplementation audit is shown in Fig. 1, with a more detailed comparison presented in Table 4. Overall, in the postimplementation audit cycle, there were improvements in compliance for each audit criterion. Among the patients that were audited, screening for depression during the acute inpatient stay (criterion 1) attained 100%, rising from 0 in the baseline. In addition, compliance with education for patients (criterion 5) and nurses (criterion 6) about PSD assessment, prevention, and management also reached 100%, rising from 0 in the baseline. The compliance for criterion 3 (psychotherapy) was 88%, whereas compliance for criterion 2 (exercise programs) and criterion 4 (social support) both reached 84%. Lastly, the nurses’ knowledge was assessed using a questionnaire that was completed by nurses after they received training, and revealed the average score was 86.07/100 (see Table 2).
Table 4 - Comparison of baseline and follow-up audits of compliance with each criterion Baseline audit Follow-up audit Audit criteria Sample size Yes No Sample size Yes No x 2 p-value (1) Screen upon admission 87 0 87 75 75 0 – <0.001 (2) Exercise programs 87 9 78 75 63 12 88.50 <0.001 (3) Psychotherapy 87 5 82 75 66 9 110.69 <0.001 (4) Social support 87 43 44 75 63 12 21.29 <0.001 (5) Education of patients or caregivers on poststroke depression 87 0 87 75 75 0 – <0.001 (6) Education and training of nurses on poststroke depression 14 0 14 14 14 0 – <0.001The high incidence of PSD and its negative impact on the living standards of people living with stroke are well known.4 Nevertheless, in clinical practice, inadequate screening, prevention, and management of PSD are common. Therefore, it is necessary to develop quality improvement programs to help nurses systematically manage and reduce the occurrence of PSD. In the current project, we used mixed methods (nursing records audit, patient and caregiver surveys, and surveys of nurses’ knowledge) to evaluate the benefits of the screening, prevention, and management of PSD in a 56-bed neurology ward of the Fifth Affiliated Hospital of Zunyi Medical University, using practice change strategies and tools based on three JBI evidence summaries15,19,21 and two guidelines.10,12 The sample size included 14 nurses, 162 stroke patients and their caregivers.
Results from the baseline audit confirmed that there was a lack of screening, prevention, and management of PSD in clinical practice, with three out of the six audit criteria recording a compliance level of 0%. Following the implementation of our program, we found an improvement in all six criteria. Three criteria compliance rates significantly improved from 0% to 100%: criterion 1 (screened upon admission), criterion 5 (education of patients or caregivers on PSD), and criterion 6 (education and training of nurses for PSD). Further, three criteria also significantly improved: criterion 2 (exercise programs), criterion 3 (psychotherapy), and criterion 4 (social support). Many factors contributed to this improvement, including support from the director of nursing, supervision of the head nurse of the neurology department, organization by the project leader, and education of both nurses and patients.
The baseline audit revealed five barriers when attempting to implement best practices by the project team. These barriers were grouped into three categories: system-related (e.g., the department lacked screening tools and comprehensive education resources), nurse-related (e.g., increased workload and a lack of motivation and knowledge), and patient-related (e.g., lack of knowledge).
To address the system-related barriers, a series of strategies was implemented. The director of nursing and the head nurse worked to increase the motivation of stakeholders to participate in the project through award policy and encouragement. Other strategies to address the system-related barriers included optimizing the prevention and management of PSD to improve work efficiency and obtaining validated screening tools and comprehensive education materials about the management of PSD. These strategies were shown to effectively improve compliance.
To address the nurse-related barriers and improve their compliance with the evidence-based practice of PSD management, an education program was introduced. The education program included a PowerPoint presentation to impart knowledge on the screening, prevention, treatment, and management of PSD. Another crucial part of the presentation focused on how to quickly and effectively screen for PSD using a two-step method. This approach yielded positive results demonstrated by the improvement in compliance with criterion 1 (screening for depression during the acute inpatient stay) and criterion 6 (education and training of nurses). To further highlight this finding, the baseline audit revealed that the rate of screening for depression upon admission was low, signifying that nurses may have been unaware of the psychological state of patients with stroke before the implementation of this project. The subsequent improvement in the average score on the paper-based test on PSD knowledge, undertaken by all trained nurses, reflected the success of the education program for changing clinical practice and knowledge of PSD. Results from the follow-up interviews with nurses indicated that the combined use of the two scales helped nurses to quickly and accurately screen patients with stroke for depression upon admission.
To overcome the patient-related barriers, patients and their caregivers received an education pamphlet that included the risk factors, prevalence, prevention, and treatment of PSD. After strengthening the training of nurses on PSD-related knowledge, the health education of patients also improved, illustrated by the compliance rate of criterion 5 reaching 100%. For some patients with PSD who were unable to understand the content of the education pamphlets provided or those who were reluctant to take the initiative to learn independently, nurses would provide other means of education, such as broadcasting videos relating to PSD and carrying out health education lectures.
Although there was an improvement in compliance for all criteria, criteria 2, 3, and 4 did not reach 100%. Certain factors may have influenced these findings. For example, in criterion 2, 12 of the 75 patients failed to engage in physical exercise due to complications after their stroke, resulting in an incapacity to complete the exercises. Regarding criterion 3, 9 of the 75 patients did not receive an individualized psychological intervention program from nurses. There were two main reasons for this; nurses may have unintentionally overlooked intervening psychologically with patients because of their large workload, and in addition, some patients were unwilling to communicate with the nurses. With respect to criterion 4, 12 of the 75 patients did not receive visits or encouragement from their family, friends, or colleagues. This may have been due to a lack of time that some family members had to spend time with the patient due to work. Other family members and friends of patients reported that this type of social support would be ineffective in improving the patient's mood. Therefore, as a whole, while the strategies that were implemented to address the three categories of barriers were successful, improvements can still be made in specific areas.
Although several authors have summarized the evidence on PSD and its management, there are few published studies demonstrating where this evidence has been implemented in clinical practice or illustrating the processes and outcomes of knowledge translation (implementation) interventions. In a study by Van Dijk et al.,22 the implementation of a PSD toolkit resulted in a substantial increase in depression screening (+72.9%) and more patients receiving nursing interventions for PSD (+11.1%). The authors of another study showed that screening for PSD in patients by a trained nurse leads to the correct detection of depression.23 Furthermore, the results of our study are mostly consistent with those presented in a systematic review of treatment interventions for PSD. However, the authors of the review concluded that interventions focusing on social support were ineffective for the severity of depression. It was suggested that applying these forms of interventions may need the competence of experienced nurses with an advanced practice qualification, such as a nurse practitioner.24
A separate study from China examined the application of PSD prevention nursing practice protocols by aggregating evidence related to PSD prevention. The authors reported a reduced incidence of PSD (pre–post difference 27.74%) and increased nurses’ compliance rates regarding PSD prevention.25 These findings were consistent with aligned aspects of the current study, noting that our intervention was more comprehensive, also covering screening and management of PSD.
Future plans are in place following the project presented in this paper to sustain practice change by providing regular nursing training, patient education, frequent supervision, discussion, feedback, improvement, and management support. It is acknowledged that there have been updates of the guidelines on PSD in China and in other countries. It may be that audit programs to monitor practice or the features of PSD implementation interventions need to be updated regularly to align with updated or new recommendations.
ConclusionThe success of this project shows that strategies for the screening, prevention, and management of PSD can be implemented as evidence-based practice in neurology wards that target nursing practice and patients. We have established a workflow to help nurses manage PSD based on the current evidence and recommendations for China. Through training, nurses increased their focus on screening, prevention, and management of PSD and acquired the knowledge and skills needed for better care. In future research, implementation projects should focus on a broader context to ensure that more patients with PSD can effectively manage depressive symptoms and improve their quality of life.
LimitationsDespite the success of the implementation of the project, there were some limitations. First, due to a lack of time and funds, the best practice audit was only carried out in one hospital and on a small sample size of nurses and patients, reducing the generalizability of this study to other hospitals, groups of clinicians, and patients. Second, the timeframe of the implementation project was relatively short. However, 6 months is considered a common implementation period; a longer evidence-based period may have a larger effect on changing the behavior of nurses. In the future, more research with a larger sample size should be implemented to promote better management of PSD and observe the effect of this best practice.
AcknowledgmentsThe authors would like to thank the Neurology Department of the Fifth Affiliated Zhuhai Hospital of Zunyi Medical University for providing the opportunity to implement this project. The authors would also like to thank all team members and clinical nurses involved in this project.
FundingThe current project was funded by the implement science-driven agent simulation to construct psychological and behavioral intervention procedures for stroke patients-based on stepped wedge randomized controlled trial (the National Natural Science Foundation of China: NO:.82260281).
Author contributionsN.L., J.T., D.C., and O.B. developed the study design, supervised the analysis, and contributed to the final version of the article. J.T., B.D., and N.L. contributed to data analysis and drafting of the article and provided important intellectual content. D.C., Y.W., and Y.L. assisted in drafting the article for this study. All authors have read and approved the final article.
Conflicts of interestThere is no conflict of interest to declare for this project.
References 1. Campbell BCV, Khatri P. Stroke. Lancet 2020; 396:129–142. 2. Wang W, Jiang B, Sun H, Ru X, Sun D, Wang L, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation 2017; 135:759–771. 3. Wang YJ, Li ZX, Gu HQ, Zhai Y, Jiang Y, Zhao XQ, et al. China Stroke Statistics 2019: a report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc Neurol 2020; 5:211–239. 4. Towfighi A, Ovbiagele B, El Husseini N, Hackett ML, Jorge RE, Kissela BM, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2017; 48:e30–e43. 5. Dalvand S, Gheshlagh RG, Kurdi A. Prevalence of poststroke depression in Iranian patients: a systematic review and meta-analysis. Neuropsychiatr Dis Treat 2018; 14:3073–3080. 6. Karaahmet OZ, Gurcay E, Avluk OC, Umay EK, Gundogdu I, Ecerkale O, et al. Poststroke depression: risk factors and potential effects on functional recovery. Int J Rehabil Res 2017; 40:71–75. 7. Taylor-Rowan M, Momoh O, Ayerbe L, Evans JJ, Stott DJ, Quinn TJ. Prevalence of pre-stroke depression and its association with post-stroke depression: a systematic review and meta-analysis. Psychol Med 2019; 49:685–696. 8. Cai W, Mueller C, Li YJ, Shen WD, Stewart R. Post stroke depression and risk of stroke recurrence and mortality: a systematic review and meta-analysis. Ageing Res Rev 2019; 50:102–109. 9. Wu QE, Zhou AM, Han YP, Liu YM, Yang Y, Wang XM, et al. Poststroke depression and risk of recurrent stroke: a meta-analysis of prospective studies. Medicine (Baltimore) 2019; 98:e17235. 10. Zhao FY, Yue YY, Li L, Lang SY, Wang MW, Du XD, et al. Clinical practice guidelines for post-stroke depression in China. Braz J Psychiatry 2018; 40:325–334. 11. Pamaiahgari P. Evidence Summary. Post-stroke depression: risk factors. The JBI EBP Database, JBI@Ovid. 2019; JBI9018. 12. Lanctot KL, Lindsay MP, Smith EE, Sahlas DJ, Foley N, Gubitz G, et al. Canadian stroke best practice recommendations: mood, cognition and fatigue following stroke, 6th edition update 2019. Int J Stroke 2020; 15:668–688. 13. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016; 47:e98–e169. 14. Porritt K, McArthur A, Lockwood C, Munn Z, editors. JBI manual for evidence implementation. JBI; 2020. Available at: https://implementationmanual.jbi.global. 15. Moola S. Evidence Summary. Post-stroke depression: screening. The JBI EBP Database, JBI@Ovid 2019; JBI9019. 16. Wang SS, Zhou XY, Zhu CY. Chinese expert consensus on clinical practice of post-stroke depression. Chin J Stroke 2016; 8:685–693. 17. Volz M, Mobus J, Letsch C, Werheid K. The influence of early depressive symptoms, social support and decreasing self-efficacy on depression 6 month
留言 (0)