
記住我


Following the results of a pilot study showing an improvement in survival and lower resection rates [4], we created an intestinal stroke center (ISC) that provides 24/7 standardized multimodal and multidisciplinary care to AMI patients referred from the Paris region. Since the creation of this center, we prospectively enrolled AMI patients from the ISC department and control patients who underwent a contrast-enhanced CT-scan for acute abdominal pain from the emergency room (ER) as part of the SURVIBIO cross-sectional diagnostic study. This study was performed following the ethical standards of our institution's Committee on Human Experimentation (Institutional Review Board N°00006477, approval 15-062) and reported according to the Strengthening the Reporting of Observational Studies Epidemiology (STROBE) guidelines [16]. Informed consent was obtained from all patients.
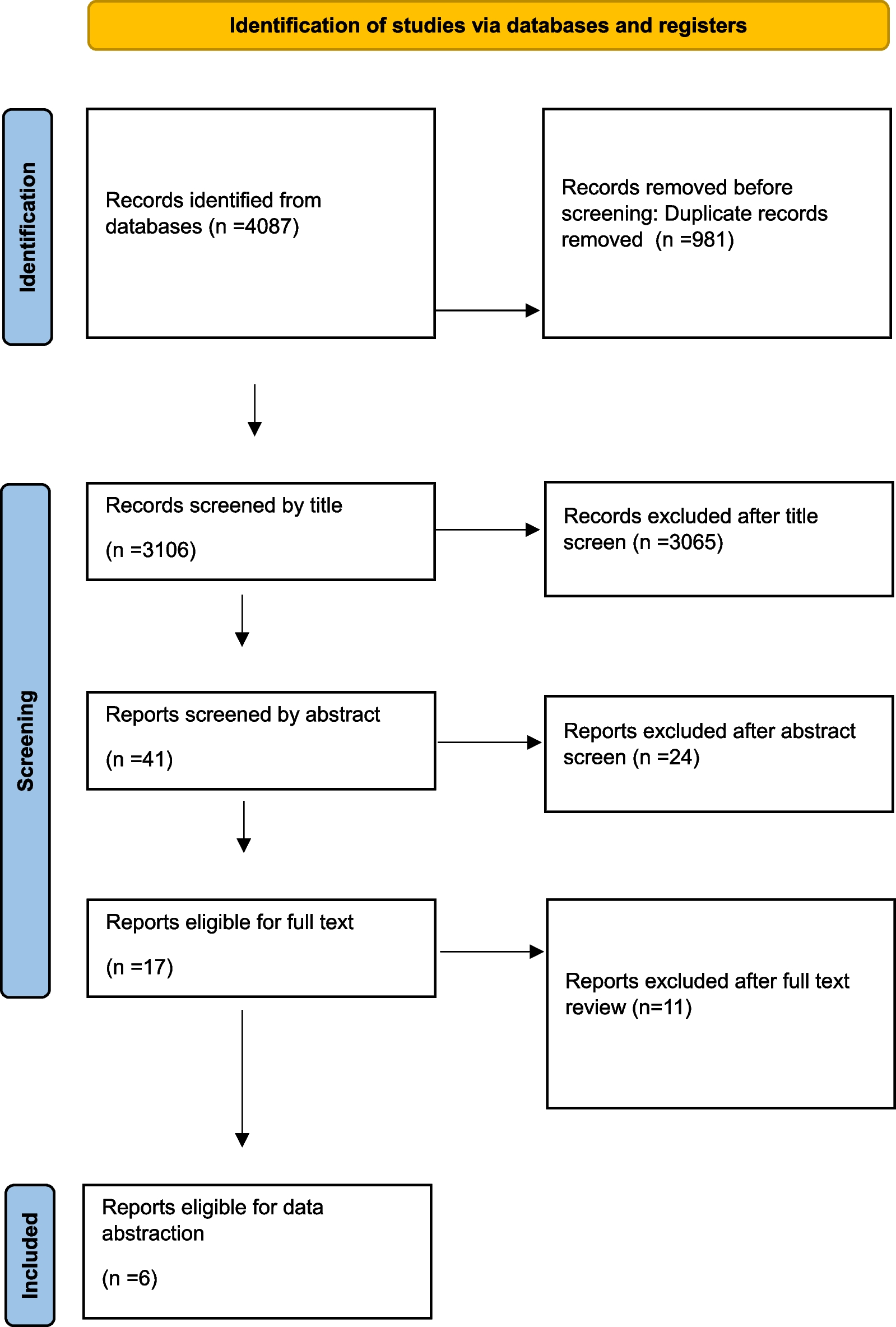
Patients and controlsFrom January 4, 2016, to March 5, 2018, prospective patients who presented with acute abdominal pain requiring a contrast-enhanced multiphasic CT scan to the ER department or referred to the ISC department were evaluated for inclusion in the SURVIBIO diagnostic study. Patients with AMI were admitted to the ISC, whereas those for whom the diagnosis of AMI was ruled out (controls) were admitted to the ER (see patient flowchart, Fig. 1). As previously published [12], the SURVIBIO diagnostic study was originally designed to assess diagnostic biomarkers of AMI. Patients presenting with a diagnosis of left-sided colon ischemia without small bowel injury, chronic mesenteric ischemia without acute injury, vascular lesions with no small bowel injury, or strangulated bowel obstruction were not included so as not to introduce heterogeneity to either the AMI or control groups (see patient flowchart, Fig. 1).
Fig. 1
Flowchart of AMI patients and controls: screening and selection
AMI was defined by the association of (1) acute clinical, biological, and contrast-enhanced CT features of bowel injury, (2) vascular insufficiency (occlusive or non-occlusive) of the celiac trunk and/or the superior mesentery artery and/or superior mesenteric vein, and (3) the absence of an alternative diagnosis [5]. The diagnosis of AMI was confirmed or ruled out by the CT scan and alternative final diagnoses were based on clinical, laboratory, and CT findings. Finally, all included patients underwent a multiphasic CT scan including arterial and venous phase images as previously described [17], and a routine biological work-up. Patient clinical records, CT scans, and pathological specimens were reviewed in a monthly multidisciplinary meeting that included gastroenterologists, radiologists, digestive and vascular surgeons, and intensivists, all experts in digestive vascular diseases to avoid misdiagnosis. All CT-scans were reviewed by two senior radiologists specialized in both AMI and digestive diseases (LG and MR).
All AMI patients were managed following a standardized multimodal and multidisciplinary approach in our ISC, as previously described [4]. Briefly, the patients were systematically administered oral antibiotics and antithrombotics [4, 5], and emergency endovascular revascularization of arterial AMI was performed whenever technically feasible. Alternatively, open surgical revascularization was performed. In addition, bowel viability was evaluated following published risk factors for irreversible transmural intestinal necrosis (occurrence of organ failure, elevated serum lactate concentrations, small bowel dilatation, or perforation on CT) [18]. Irreversible transmural intestinal necrosis was confirmed upon pathological assessment.
Data collection and processingRoutine baseline clinical and biological characteristics were prospectively collected upon admission for all patients: age, gender, history of cardiovascular disease, atherosclerosis risk factors (i.e., tobacco consumption, high blood pressure, diabetes mellitus, or elevated cholesterol or triglycerides), history of venous thromboembolism, history of chronic kidney disease, cirrhosis, ischemic colitis, or abdominal surgery. In addition, the following data concerning AMI was collected: clinical signs at presentation (characteristics of acute abdominal pain, including sudden onset or a requirement for morphine (or other strong opioids), gastrointestinal bleeding, diarrhea, vomiting, constipation, abdominal guarding, sequential organ failure assessment (SOFA) score, and laboratory test values at presentation (white blood cell [WBC], neutrophil, lymphocyte, and platelet counts, the neutrophil-to-lymphocyte ratio [NLR], and hemoglobin, and plasma C-reactive protein [CRP], procalcitonin, l-lactate, blood urea nitrogen, creatinine, aspartate aminotransferase, and bilirubin levels). Morphine-requiring abdominal pain was defined as a pain unrelieved by weak opioids (such as tramadol or codeine) and relieved by > 2 mg intravenous morphine (or equivalent). Pain relief was defined as ≤ 30/100 mm on the visual analogue pain scale. The sudden-onset was defined by an abdominal pain that started and peaked within an hour or less. The origin of AMI (arterial–thrombotic or embolic–venous, or non-occlusive) was specified based on the patient records, CT scan, and pathological review.
Statistical analysisCategorical variables, expressed as counts (percentages) and frequency distributions, were compared between groups using Chi square or Fisher exact tests, as appropriate. Continuous variables are expressed as medians [interquartile ranges (IQR)] and were compared between groups using Student t or Mann–Whitney U tests, as appropriate. Associations between the clinical and biological presentation and the diagnosis of AMI were assessed through multivariate logistic regression models. The main model included the following covariates: sudden-onset and morphine-requiring abdominal pain, abdominal guarding, SOFA score > 2, and WBC. A series of sensitivity analyses were performed to assess the robustness of the findings (Additional file 1). Models with further adjustments for age, history of cardiovascular disease, atherosclerosis risk factors, hematochezia, CRP and procalcitonin were also tested. Multicollinearity between selected variables was assessed using the variance inflation factor (VIF). Variables were considered to be suspicious for collinearity when the VIF was > 5 [19]. Neutrophil counts were excluded from the multivariate model because of collinearity with white blood cell counts. All other covariates were included in the model and no variable selection was performed. Results of the multivariate analysis are shown as odds ratios (ORs) (95% confidence interval) and were used to compute a score according to the number of independent factors. The accuracy of the resulting score was further evaluated using the area under the receiver operating characteristic (AUROC) curve, sensitivity, specificity, and positive/negative likelihood ratios. All tests were two-sided. A p-value < 0.05 was considered significant. No imputation of missing data was performed. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Mac OSX software (version 23.0, Chicago, IL, USA) and the pROC package in R software, version 3.6.2 (R Foundation for Statistical Computing) [20].
留言 (0)