Explanation for the choice of comparators
The standard French liver allocation rules will be followed. The study does not interfere or change the process of accepting or declining a liver graft offered to a patient in any way. If the liver is suitable for transplantation and all inclusion and exclusion criteria are met, the liver will be randomized to either HOPE after cold storage or static cold storage only. The control group will use the gold standard static cold storage technique (4 °C) with Institute George Lopez (IGL-1)® solution from graft harvesting until liver transplantation as routine practice in the eight centers.
Intervention description Study group
Identification of the medical device
ECD liver grafts will be perfused with hypothermic oxygenated perfusion (HOPE) via the portal vein only for a minimum of 1 h (ideally 1–4 h) after the “back-table” phase (graft preparation). This will be performed, in parallel with the recipient hepatectomy, using the CE-certified Liver Assist® perfusion pump/device (XVivo®, Sweden) with Machine Perfusion Solution (Belzer-MPS, CE-certified). Ideally, the graft should be placed in the machine before or at the time of the incision of the recipient to allow a duration of machine perfusion of the graft between 1 and 4 h. The machine perfusion time should not exceed 4 h. However, if the hepatectomy phase is longer than expected, the graft can remain on perfusion and used for transplantation. A notification of adverse events with specific interest will have to be done if the hypothermic oxygenated perfusion lasted more than 4 h.
The Liver Assist® is a pump system providing temperature-controlled dual oxygenated isolated perfusion of donor livers to bridge the time span between the donor hepatectomy and the liver transplantation in the recipient.
The Liver Assist® is a modular system consisting of five main modules:
Portal vein pump unit (for portal vein perfusion)
Hepatic artery pump unit (for hepatic artery perfusion) (not used in this study where only the portal vein is perfused)
Thermo unit
Trolley including table top
Disposable set
The device incorporates neither medical substances nor non-viable materials of animal origin.
Date of CE mark: CE 663647 25/11/2016.
Market authorization: November 29, 2006.
Intended use of the medical device
The Liver Assist is intended to be used for isolated ex vivo oxygenated machine perfusion of donor livers, for up to a period of 4 h.
Method of use of the device
If the patient is randomized into the machine perfusion group, the first part of graft preservation is similar to the control group. The graft is perfused and stored in Institute George Lopez (IGL-1®) solution at 4 °C during transport to the transplantation center.
As soon as the liver graft arrives at the transplantation center, the surgeon immediately prepares it on the back-table. The graft is then put on the Liver Assist perfusion machine around the time the transplant procedure begins.
Perfusion settings will be:
Use of the same perfusion machine device in all centers (Liver Assist, Xvivo)
Hypothermic perfusion (8–12 °C)
Portal vein perfusion: portal vein is cannulated
Adjusted perfusion flow: 150–250 ml/min under 3 mmHg in the portal vein
Perfusate oxygenation at 70 kPA
Use of 3 L of perfusion solution: Machine Perfusion Solution (Belzer-MPS, Bridge-To-Life, CE-certified)
Contraindications, warnings, possible risks
The Liver Assist perfusion machine is routinely used worldwide, and many experiments in patients have been reported in the literature [14]. There are no specific contraindications. The main advantage of hypothermic perfusion compared to normothermic perfusion, is that, in the event of a defect in the machine, the liver graft stays in hypothermic conditions and is protected against ischemic injuries. Even if the machine cannot be run, the liver graft is kept in static cold storage and can still be implanted in the recipient.
Control group
The control group will use the gold standard static cold storage technique (4 °C) with Institute George Lopez (IGL-1)® solution from graft harvesting until liver transplantation as routine practice in the eight centers.
Criteria for discontinuing or modifying allocated interventions
In the following instances, patients will terminate the study prematurely if:
Technical problem preventing any use of the perfusion machine
Non-transplantable patients (e.g., peritoneal carcinosis)
However, all patients undergoing liver transplantation under the protocol conditions will be included in the modified intention-to-treat analysis (full analysis set).
Strategies to improve adherence to interventions
The intervention is a single event requiring no adherence monitoring.
Relevant concomitant care permitted or prohibited during the trial
There are no additional restrictions other than those listed in the non-inclusion criteria.
Provisions for post-trial care
The sponsor has subscribed to an insurance policy for the entire duration of the study, covering its own civil liability as well as that of all the physicians involved in the realization of the study. It will also insure the full compensation for harmful consequences of the research for the participating persons and their beneficiaries, except with evidence, at their responsibility, that the damage is not attributable to their mistake or to that of all consultants, without the possibility of being opposed to an act by a third party or the voluntary withdrawal of the person who had initially consented to participate in the research.
Outcomes Primary endpoint
Difference between the two treatment arms in the proportion of patients with early allograft dysfunction (EAD). EAD (according to Olthoff et al. [7]) is defined by the presence of at least one of the following criteria:
Bilirubin level > 10 mg/dL (i.e., 171 μmol/L) on postoperative day (POD) 7
INR > 1.6 on POD 7
AST or ALT level > 2000 IU/L within the first 7 PODs
Primary non-function (PNF) of the graft is the very last stage of any EAD and is defined by the presence of at least one of the following criteria:
Secondary endpoints
1.
Quality of conservation
Dosage during perfusion by the HOPE machine (AST, ALT, LDH, hyaluronic acid, lactate levels in machine perfusate at 30 min and at the end of the perfusion)
Additional 3 mL of machine perfusate will be sampled at 30 min and at the end of machine perfusion and stored at − 80 °C. Those samples will be used in case of future unexpected research about machine perfusate compounds
2.
Difference between the two treatment arms in the proportion of patients with ischemia–reperfusion injuries
Liver injury assessed by serum AST and ALT at 6 h (± 2 h), 12 h (± 2 h) and every day until POD7 after transplantation
Post-reperfusion liver biopsy (histological changes, level of necrosis)
Untargeted liver graft metabolic profiling (by high-resolution nuclear magnetic resonance—1H HR-NMR spectrometer) on liver biopsies on the back-table in both study groups and immediately after liver perfusion in the HOPE group. This test will be centralized in the Strasbourg center
3.
Difference between the two treatment arms in the proportion of patients with intra-operative events
Intra-operative blood transfusions (red blood cells, fresh frozen plasma, thrombocyte concentrate)
Occurrence of post-reperfusion syndrome, defined as a 50% decrease in median arterial pressure during the 5 min following the graft revascularization
Duration of surgery
4.
Postoperative outcome (liver function tests not included in the definition of EAD)
Difference in means between the two treatment arms for:
Recipient blood level of factor V at 6 h (± 2 h), 12 h (± 2 h) and every day until POD7
Arterial lactates at 6 h (± 2 h), 12 h (± 2 h) and every day until discharge from intensive care (and maximum until POD7)
MEAF score (0–10) at POD3, including POD3 bilirubin, ALT max, and INR max at POD3. This score will be compared with the Olthoff’s definition of EAD and the L-GrAFT risk factor
L-GrAFT risk factor (− 6 to + 6) including AST, INR, total bilirubin, and platelets every day until POD 10. This score will be compared with both MEAF score and Olthoff’s score
Kidney function tests
Daily serum creatinine level during the first 7 PODs
Daily glomerular filtration rate (assessed using MDRD and CKD-EPI) during the first 7 PODs
Difference between the two treatment arms in the proportion of patients requiring renal dialysis within the first 7 PODs
5.
90-day morbidity and mortality
Difference between the two treatment arms in the proportion of patients with severe postoperative complication (defined as Dindo–Clavien classification ≥ 3) occurring before day 90 post surgery
Difference in means between the two treatment arms of the comprehensive complication index (CCI) [19] at day 90
Difference between the two treatment arms in the proportion of patients who were deceased before day 90 after surgery
6.
Difference in means between the two treatment arms of the length of intermediate care unit stay and total hospital stay
7.
Difference between the two treatment arms in the proportion of patients with intra- and extrahepatic biliary complications within the first year after liver transplantation, assessed by:
Serum cholestasis parameter (bilirubin, gamma-glutamyl transferase, alkaline phosphatase) every 3 months until 1 year
Liver contrast-enhanced MRI, including a magnetic resonance cholangiopancreatography (MRCP), 12 months after liver transplantation (except for patients who underwent a re-transplantation during the study)
8.
Actuarial graft and patient’s survival rates at 3 months and 1 year
Difference between the two treatment arms in the proportion of patients without graft loss at 3 months and 1 year.
Difference between the two treatment arms in the proportion of patients alive at 3 months and 1 year.
9.
Costs of liver transplantation with ECD grafts using HOPE or not, incremental cost-effectiveness ratio at 12 months post-surgery. Details about the cost-effectiveness analysis are given in Supplementary Material 2.
Participant timeline Study calendar
Duration of the inclusion and randomization period: 36 months.
Duration of follow-up by patient: 12 months (± 30 days) after transplantation (36 months maximum).
Total duration of the study: 48 months (± 30 days).
Start of inclusions: September 2019.
Conduct of the study
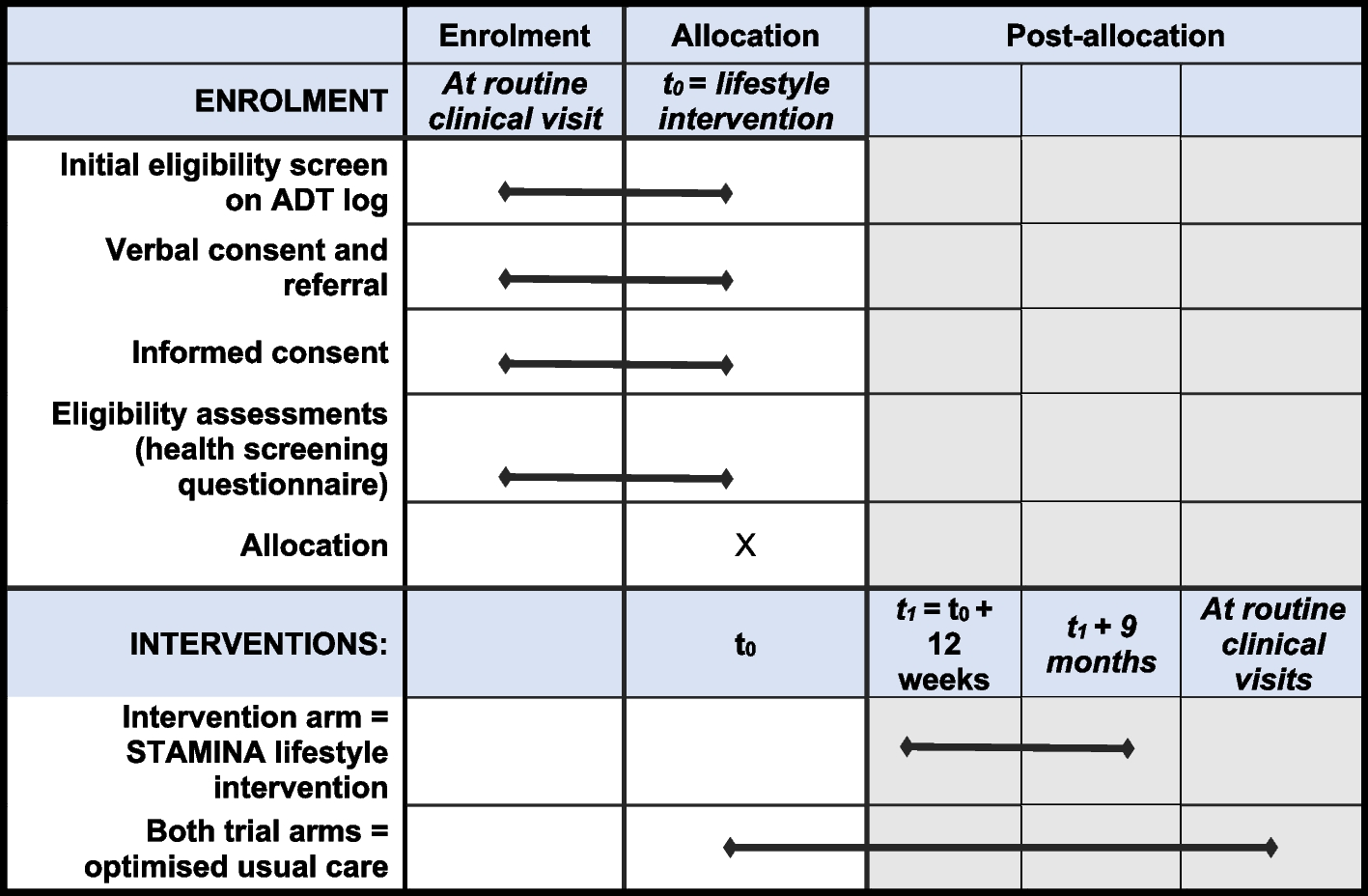
The overall schedule and time commitment for trial participants are summarized in Table 1.
Table 1 Schedule of enrolment, interventions, and assessments in the HOPExt trialPre-screening
Patient eligible for liver transplantation after decision of the multidisciplinary board.
Screening visit = V1
All consecutive transplant candidates admitted to interdisciplinary transplant outpatient clinics requiring liver transplantation will be assessed for study eligibility by senior staff physicians (transplant surgeon). Patients on the waiting list for liver transplantation will be informed orally and in writing by a physician (transplant surgeon or hepatologist) about the study. Patients who are willing to participate, meet inclusion/non-inclusion criteria, and provide written informed consent will be included in the study.
Past medical history and patient characteristics will be collected: age, gender, height, weight, BMI, blood group, cause of cirrhosis, indication of transplantation, medical history (diabetes mellitus, arterial hypertension, transjugular intrahepatic portosystemic shunt), and pretransplant status of residence (home, hospital ward or ICU). The MELD score at inscription (INR, creatinine, bilirubin, and dialysis) is also recorded.
Inclusion visit/randomization = V2
D0, visit 2
Verification that the consent form was signed by the patient and the investigator.
After the allocation and acceptance of the organs, the investigator will check the eligibility criteria. If the criteria are met, the liver recipient (study participant) will be randomized. The team of local investigators will be informed accordingly in order to set up the perfusion device. If the criteria are not respected, the patient will leave the study (premature termination of participation).
Randomization: it is important to note that absolutely no changes will be made to the national liver allocation rules. The study does not interfere or change the process of accepting or declining a liver offered to a certain patient in any way. Once a suitable recipient for the liver is identified, the recipient will be invited to come to the relevant transplant center for the surgical procedure as per routine procedure. Randomization will be performed after the allocation of the graft or after the harvesting team has macroscopically assessed the graft and confirmed that the graft will be harvested, according to the center practice. No study-related factors will be assessed before randomization. After checking the inclusion and non-inclusion criteria, an online randomization tool will be used. Randomization will be stratified by center and MELD score at the time of transplantation with a cut-off of 30.
Prior to transplantation: physical examination, vital signs, laboratory values (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR, lactates), MELD score (dialysis), CHILD–PUGH score (encephalopathy, ascites, albumin, prothrombin rate), and donor characteristics will be recorded. Concomitant medications and adverse events will be assessed.
Liver transplantation: back-table, recipient hepatectomy, and implantation will always be done by the principal investigator and sub-investigators. During recipient hepatectomy, the liver graft will be either stored in cold storage or perfused with the HOPE machine, according to the randomization. Parameters of the HOPE perfusion will be collected. Lot numbers of perfusate (Belzer-MPS) and perfusion device disposables will be recorded in the source document and eCRF.
In the control group, a biopsy of the liver graft will be taken at the beginning of the back-table preparation. Another biopsy will be taken after liver graft reperfusion in the recipient (routine practice).
In the experimental group, a biopsy of the liver graft will be taken at the beginning of the back-table preparation. Another biopsy will be taken at the end of the HOPE perfusion. A third biopsy will be taken after liver graft reperfusion in the recipient (routine practice). Study-related liver biopsies are (1) additional liver graft biopsy on the back-table in the control group and (2) additional liver graft biopsies before and after machine perfusion in the experimental group. Those biopsies are performed ex situ on the back-table without specific risk for the patient.
In order to look for any bacterial or fungal contamination during the whole process, samples of static storage solution (IGL in both groups) at the end of the back-table and samples of machine perfusion solution (Belzer-MPS) at the end of machine perfusion will be taken for bacteriological and fungal analyses. Those bacteriological and fungal samples will be analyzed by the microbiology laboratories of the participating centers in accordance with the European Pharmacopoeia 2.6.1 Sterility Analysis Protocol.
During surgery, intra-operative data are collected: surgical technique of transplantation (piggy-back vs. vena cava resection), length of procedure, transfusions needed (fresh frozen plasma, red blood cell, thrombocyte concentrate), occurrence of post-reperfusion syndrome (decrease of 50% of the median arterial pressure during the 5 min after the revascularization), cold ischemia time, and circulatory support at the end of transplantation (noradrenaline (mg/h)).
Follow-up visits
Visits 3–11 (6 and 12 h (± 2 h) after reperfusion and postoperative days 1–7, ± 1 day):
Laboratory analyses (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR, lactates) will be performed. Concomitant medications and adverse events will be collected.
Visit 12 (last day of hospitalization)
Physical examination and laboratory analyses (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR, lactates) will be performed. Immunosuppression medication will be confirmed and post-transplant complications (Clavien–Dindo Score, CCI) will be assessed. Concomitant medications and adverse events will be collected. Post-transplant ICU and hospital stay will be assessed.
Visit 13 (3 months (± 30 days))
After liver transplantation, patients have regular checks at hospital, where physical examinations and lab test are performed (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR). During this appointment, the following will be recorded: the incidence of main postoperative complications (kidney function disorders, need for dialysis, infections, cholestasis and biliary obstructions, vascular complications, acute rejection, arterial or portal vein thrombosis, biliary fistula), Clavien–Dindo classification score, comprehensive complication index (CCI), reintervention, length of stay in intensive care unit, length of hospital stay, retransplantation, or death within 3 months after liver transplantation.
Adverse events and concomitant medications will be collected.
Visit 14–15 (6 months and 9 months after transplantation (± 30 days))
After liver transplantation, patients have regular checks at hospital, where physical examinations and lab tests are performed (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR). During this appointment, further examinations, modification of common medications, adverse events, or post-transplant complications will be noted and treated according to the routine management of patients after liver transplantation if necessary. Results of the checks will be documented in the eCRF.
Adverse events and concomitant medications will be collected.
Visit 16 (12 months after transplantation, outpatient control, final study visit closure, (± 30 days)
This is the last study visit. Patients will have physical examinations and lab tests (AST, ALT, GGT, alkaline phosphatase, bilirubin, factor V, INR, platelets, creatinine, GFR). During this appointment, further examinations, modification of concomitant medications, adverse events, or post-transplant complications will be noted and treated according to the routine management of patients after liver transplantation if necessary. Results of these checks will be documented in the eCRF. This is also the final control, including study closure and liver contrast enhanced MRI/MRCP.
Serious and adverse events will be evaluated throughout study participation.
Sample size
A sample size of 119 patients per randomized group (238 in total) is needed based on the following parameters:
Expected decrease of EAD rate from 30% in the control group to 15% in the HOPE group (50% decrease of EAD based on previous preliminary clinical studies) [15, 20]
Alpha: 0.05
Power: 0.80
Two-sided test
The sample size was calculated using the “pwr.2p.test” function of R (R Foundation for Statistical Computing, Vienna, Austria), package “Pwr”. In order to take into account a 10% proportion of dropouts or patients who prematurely terminate the study, 133 patients shall be recruited per group, i.e., 266 patients in total. Because there is about 20% of dropouts on the waiting list in France (2017 annual report of the “Agence de la Biomédecine”), and about 50% of liver grafts are provided from ECD, it is expected that 660 patients should be included in the study to be able to randomize 266 patients. In order not to slow down randomizations as they approach the total needed, inclusions will be possible beyond 660 patients within the limit of 1000 patients included.
According to EUROTRANSPLANT and the “Agence de la Biomédecine”, 50% of liver grafts are provided from ECD with the rate increasing over recent years. To be on the safe side, we expect that centers may randomize half of their potential transplanted patients with ECD, namely 25% of their total number of liver transplantations a year.
Recruitment
The 24-month inclusion period allows a reasonable mean rate of randomized patients of 1.39 patient/month/center. All participating centers are large and well-experienced liver transplantation centers in France. To ensure an adequate number of patients will be enrolled in the required time frame, the participating centers will be asked to report on a regular basis their problems related to enrolment, in order to find adequate responses to improve the enrolment rate. Moreover, to stimulate enrolment, a newsletter describing the enrolment status will be sent regularly to all centers.







留言 (0)