
記住我
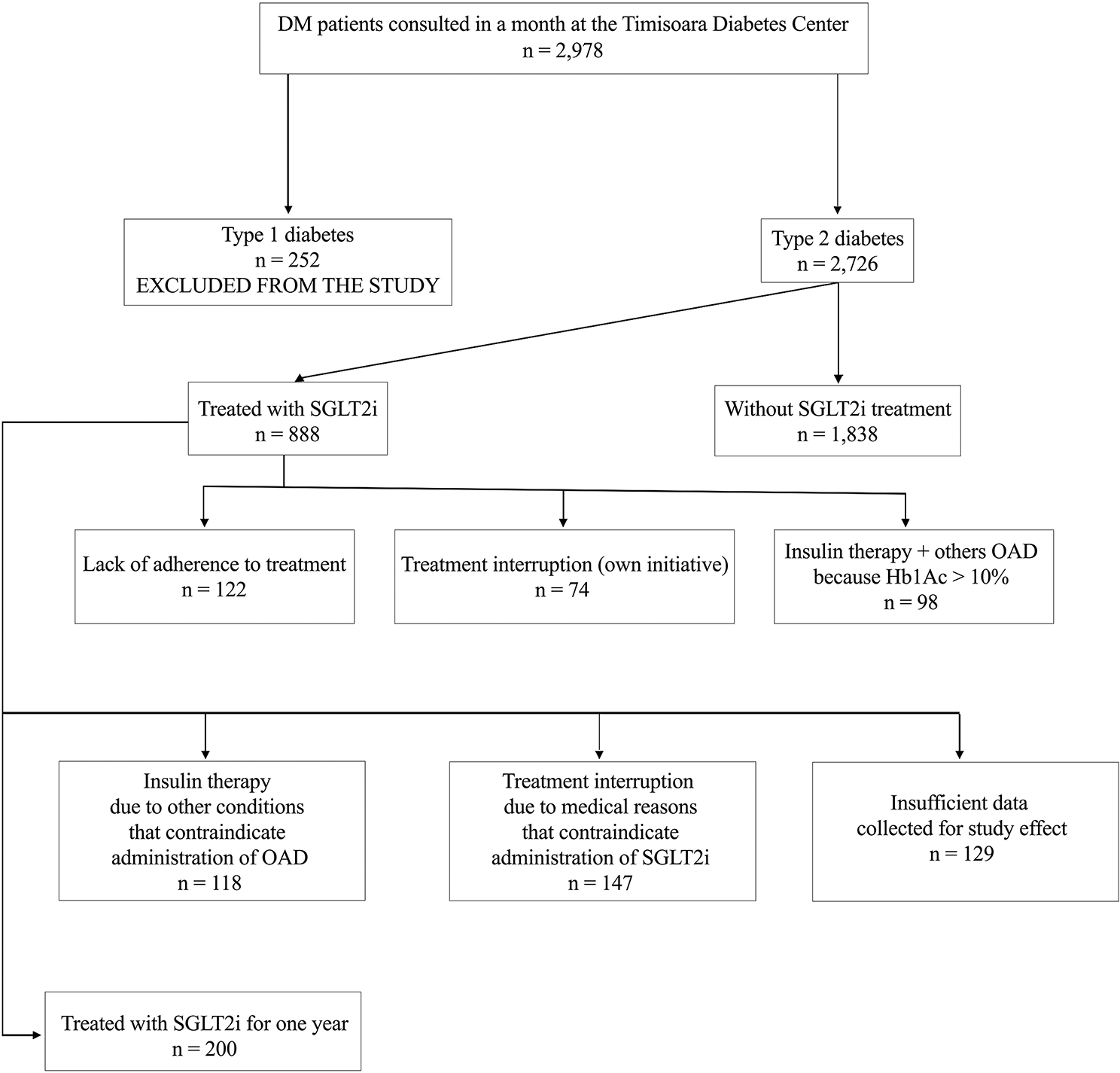
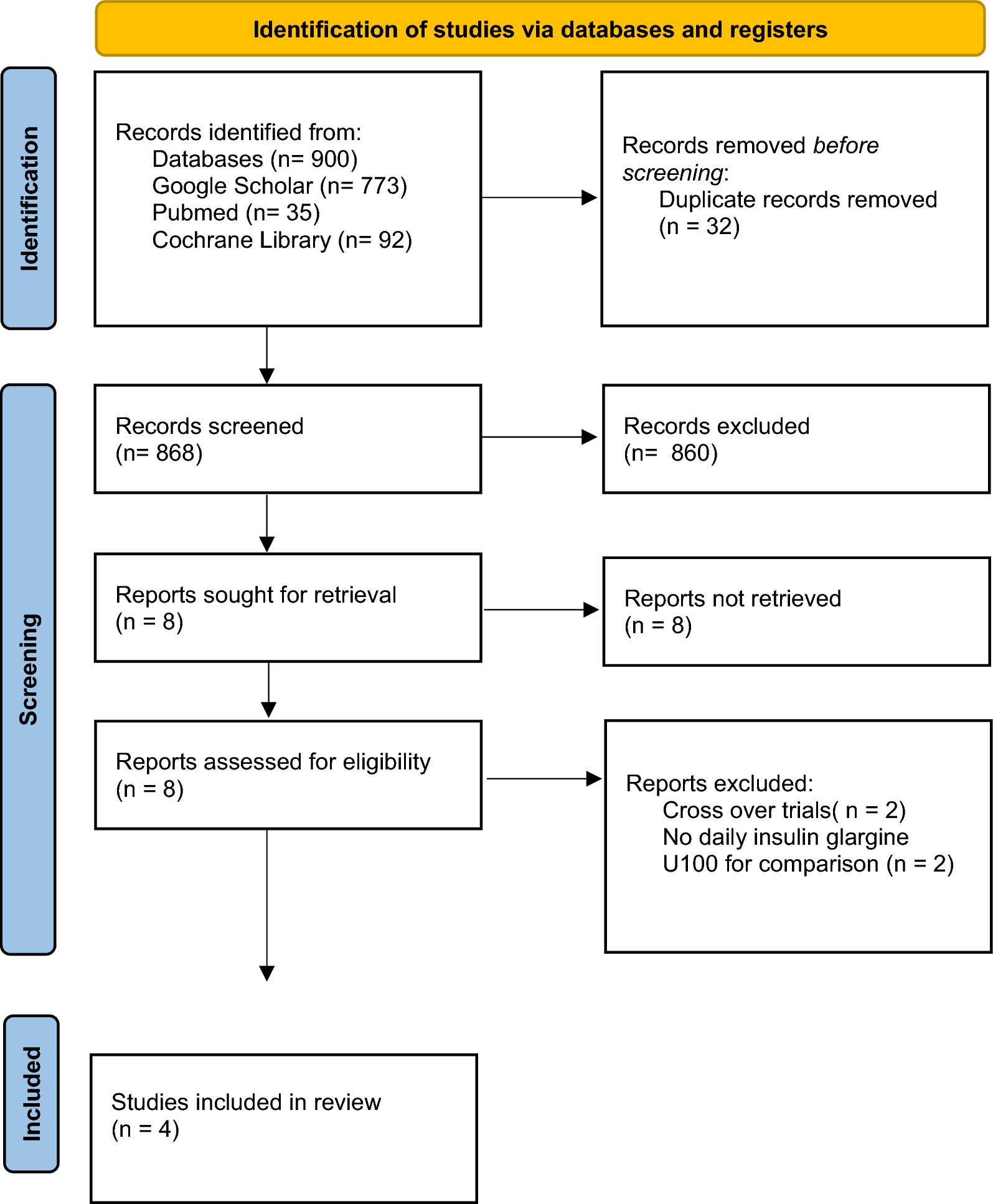
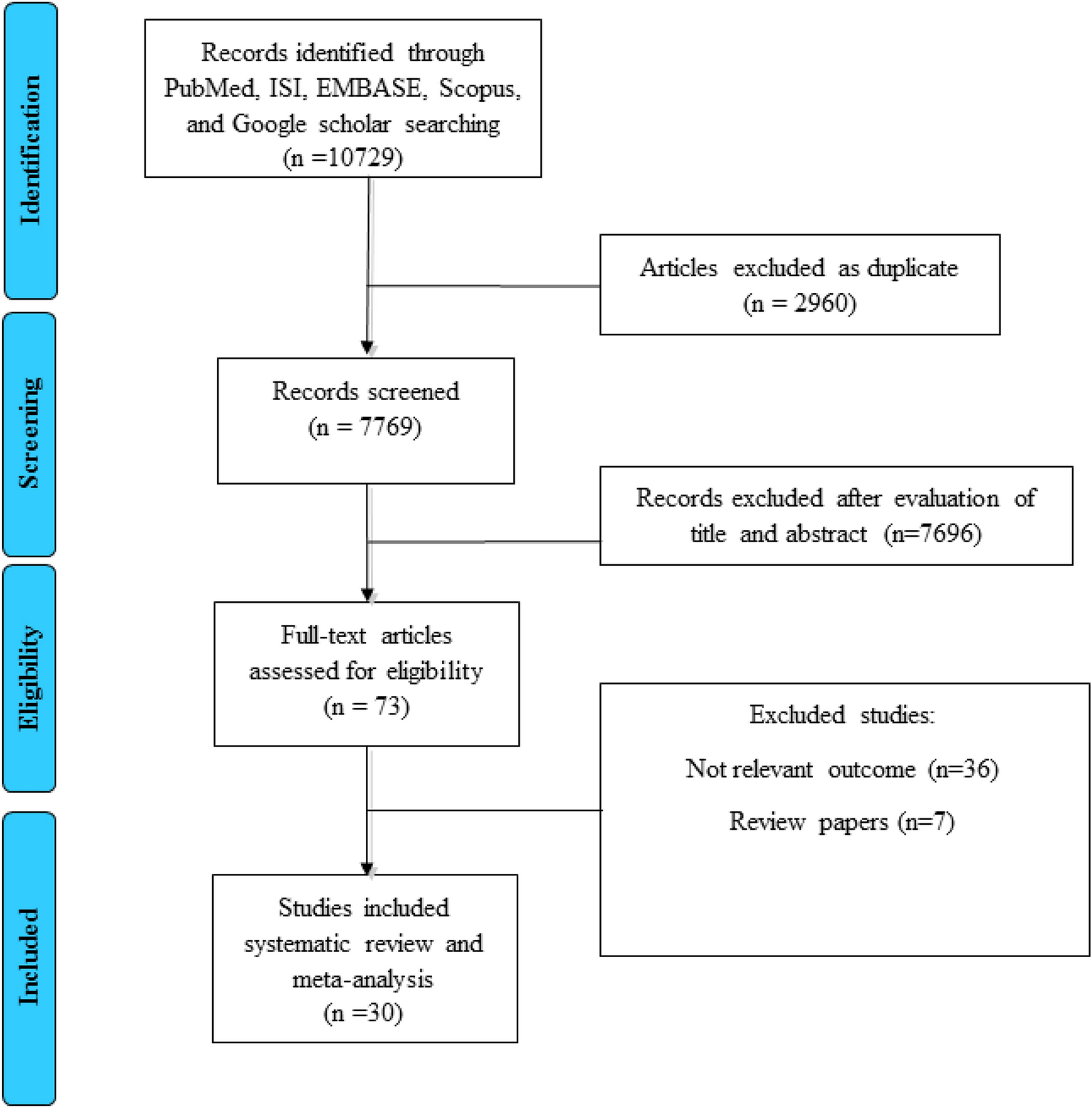
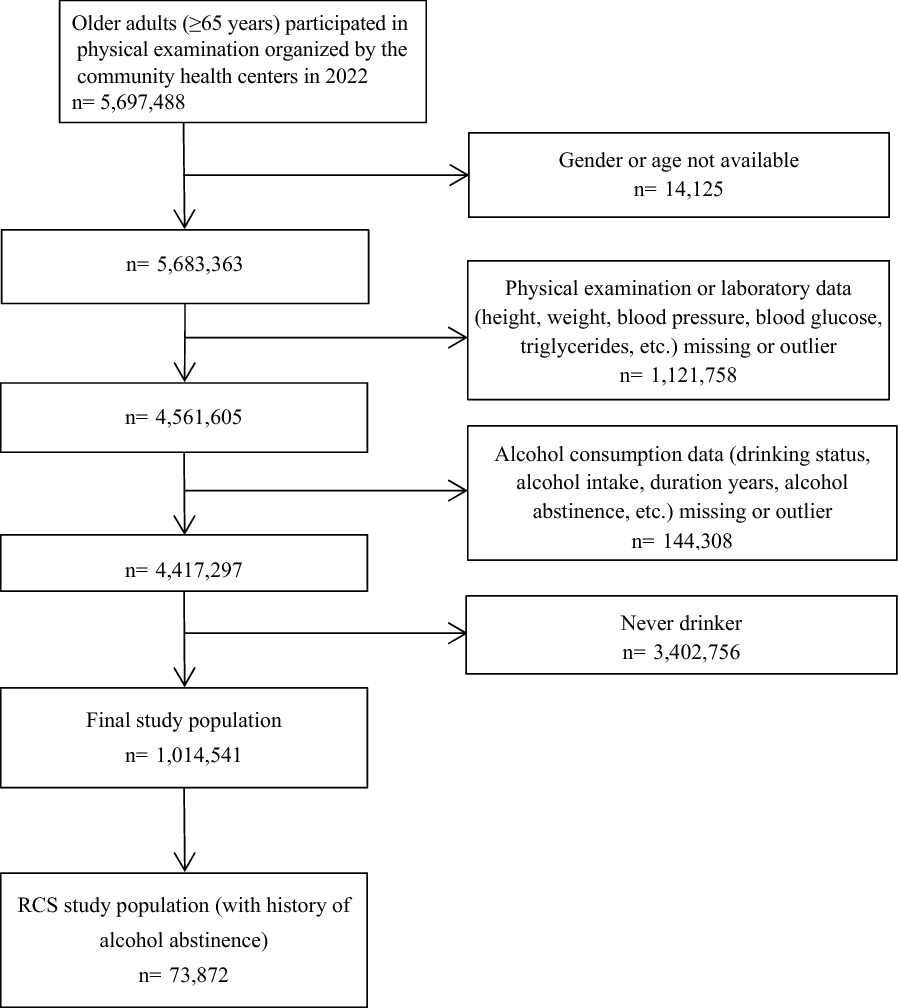
A total of 947 pieces of literature were retrieved, and ten pieces of literature [2, 9,10,11,12,13,14,15,16,17] were finally included in the analysis (literature 20 set subgroups, respectively refractory hypertension and non-refractory hypertension), with a total of 9913 participants (including 6293 in SGLT2i group and 3620 in the control group). The detailed screening process is shown in Fig. 1. Table 1 reports the basic information of the included articles.
Fig. 1
Flow chart of literature screening
Table 1 Basic information of included studiesBaseline characteristics of included cohortsTable 2 lists the subjects’ baseline data and basic information. The study population of the SGLT2i group and the control group are comparable in blood pressure, blood glucose control level, disease duration, disease severity grading, etc.
Table 2 Baseline data of the experimental population included in the studyLiterature quality assessmentThe Cochrane Collaboration’s risk of bias tool was used (Fig. 2).
Fig. 2
Literature quality assessment
Efficacy evaluation and outcome24H systolic blood pressureSeven articles were included in the study. The results showed that SGLT2i could reduce 24HSBP by 5.06 mmHg compared with placebo, 95% CI [− 7.10, − 3.01], t = − 6.19, P < 0.05, and the difference was statistically significant. The heterogeneity test showed that I2 = 83.4%, P < 0.1, showing strong heterogeneity among literature (Fig. 3). Considering the differences in the types, doses, and courses of SGLT2i in the included studies, which may cause heterogeneity, further subgroup analysis was performed, and the results were consistent (Table 3).
Fig. 3
Effect of SGLT2i on 24-h systolic blood pressure
Table 3 Subgroup analysis of the effect of SGLT2i on blood pressure24H diastolic blood pressureA total of 6 kinds of literature were included in the study. The results showed that SGLT2i could reduce 24HDBP by 2.39 mmHg compared with placebo, 95% CI [− 4.11, − 0.67], t = − 4.15, P = 0.004, and the difference was statistically significant. The heterogeneity test showed that I2 = 93.1%, P < 0.1, showing firm heterogeneity among literature, as shown in Fig. 4. Further subgroup analysis of SGLT2i type, dose, and treatment course showed consistent results (Table 3).
Fig. 4
Effect of SGLT2i on 24H diastolic blood pressure
Office systolic blood pressureA total of 8 works of literature were included in the study. The results showed that SGLT2i could reduce office SBP by 4.53 mmHg compared with placebo, 95% CI [− 5.66, − 3.40], t = − 9.50, P < 0.05, and the difference was statistically significant. The heterogeneity test showed that I2 = 69.7%, P < 0.1, showing substantial heterogeneity among literature, as shown in Fig. 5. Further subgroup analysis of SGLT2i type, dose, and treatment course showed consistent results (Table 3).
Fig. 5
Effect of SGLT2i on office systolic blood pressure
Office diastolic blood pressureA total of 7 pieces of literature were included in the study. The results showed that SGLT2i reduced office DBP by 2.12 mmHg compared with placebo, 95% CI [− 3.42, − 0.82], t = − 4.88, P = 0.001, and the difference was statistically significant. The heterogeneity test showed that I2 = 96.3%, showing substantial heterogeneity among literature, as shown in Fig. 6. Further subgroup analysis of SGLT2i type, dose, and treatment course showed consistent results (Table 3).
Fig. 6
Effect of SGLT2i on office diastolic blood pressure
HbA1cA total of 8 works of literature were included in the study. The results showed that SGLT2i could reduce HbA1c by 0.57% compared with placebo, with 95% CI [− 0.60, − 0.54], z = 37.02, p < 0.1, and the difference was statistically significant. Heterogeneity test I2 = 48.6%, Fig. 7
Fig. 7
Effect of SGLT2i on HbA1c
Sensitivity analysisThe sensitivity analysis of the effect of SGLT2i on blood pressure showed this literature [2] showed high sensitivity. The heterogeneity of the effect of SGLT2i on 24HSBP after excluding this literature was I2 = 2.8%, P > 0.1, combined effect size MD = − 4.03, 95% CI [5.10, − 2.97], z = 7.41 p = 0.000. After the literature [2] was excluded, the heterogeneity of the effect of SGLT2i on office SBP was I2 = 0%, P > 0.1, combined effect size MD = − 4.03, 95% CI [− 4.82, − 3.24] z = 10.02 p = 0.000. After excluding the literature [2], the heterogeneity of the effect of SGLT2i on 24HDBP, I2 = 0%, P > 0.1, combined effect size MD = − 1.84, 95% CI [− 2.47, − 1.21] z = 5.7 p = 0.000. After the literature [2] was excluded, the heterogeneity of the effect of SGLT2i on office DBP was I2 = 6.2%, P > 0.1, combined effect size MD = − 1.52, 95% CI [− 1.83, − 1.21] z = 9.59 p = 0.000.
Safety evaluationHypoglycemiaA total of 8 pieces of literature were included in the study, and the heterogeneity test showed I2 = 5.5%, P = 0.39, indicating no heterogeneity, RR = 1.22, 95% CI [0.916, 1.621], z = 1.36 p = 0.174. The results suggest that SGLT2i does not increase the risk of hypoglycemia compared with placebo (Fig. 8).
Fig. 8
Effect of SGLT2i on hypoglycemia and urinary tract infection
Urinary tract infectionA total of 8 studies on urinary tract infection were included. The heterogeneity test showed I2 = 0%, P = 0.76, indicating no heterogeneity, RR = 1.56, 95% CI [0.96, 2.52], meta-analysis result z = 1.79, p = 0.073, indicating SGLT2i did not increase the risk of urinary tract infection compared with placebo (Fig. 8).
Genital tract infectionA total of 9 works of literature were included in the study. The heterogeneity test showed that I2 = 49.9%, P = 0.00, indicating moderate heterogeneity. A star diagram was further drawn to judge heterogeneity, and the source of heterogeneity was analyzed by sensitivity. Ferreira [9] showed high sensitivity. After excluding this literature [9]: I2 = 16.9%, RR = 2.32, 95% CI [1.57, 3.42], z = 4.23, p = 0.00, suggesting a 2.32-fold increased risk of genital infections for SGLT2i compared with placebo (Fig. 9).
Fig. 9
Effect of SGLT2i on genital infection and renal injury
Renal injuryA total of 7 pieces of literature compared the incidence of acute kidney injury, among which, no renal injury occurred in three literature [13, 16, 17] in both the experimental and the control groups. Therefore, four pieces of literature were finally included in the meta-analysis. I2 = 59.4%, RR = 0.78, 95% CI [0.54, 1.13], Z = 1.31, P = 0.19, indicating that SGLT2i does not cause renal injury compared with placebo (Fig. 9).
留言 (0)