
記住我




Telephone triage services help in the provision of necessary emergency medical services to patients by enabling an evaluation of the patients’ conditions over the telephone. Using information provided by the patient, nurses assess the patient’s condition and can dispatch an ambulance, suggest appropriate hospitals, or send a visiting physician. This necessary service has been introduced in several countries, including the United Kingdom and Australia (1, 2). In Japan, telephone triage services were introduced in Tokyo in 2007 and in Osaka in 2009 (3). A previous study reported that the telephone triage service in the Osaka Prefecture effectively triaged patients, dispatched ambulances, and suggested appropriate medical institutions (4). The annual number of emergency medical consultations in Osaka Prefecture was mostly more than 100,000 (5).
Patients who are deemed as emergency cases based on telephone triage services should be admitted directly to the emergency department upon arrival by ambulance (2). The relationship between the use of telephone triage services and patient outcomes is unclear, though the use of telephone triage services is associated with a lower proportion of unfavorable patient outcomes (6, 7). In addition, it remains unclear what diseases it is especially effective for (6, 8).
As telephone triage services encourage patients to visit a hospital immediately by performing emergency triage according to a protocol, it may be more effective for patients with cerebrovascular diseases than for patients with other diseases, since the time from symptom onset to treatment significantly affects the prognosis of patients with cerebrovascular diseases. However, whether telephone triage services are effective for patients with cerebrovascular diseases remains unclear. If these services positively affect the prognoses of these patients, their use may become more widespread, which would further improve patient outcomes.
Using propensity score matching, this study evaluated the effects of a telephone triage service on the outcomes of patients with cerebrovascular diseases who were transported by ambulance and hospitalized.
2. Methods 2.1. Study designThis retrospective study included hospitalized patients with cerebrovascular diseases (International Classification of Diseases 10th edition [ICD-10] code: I60.0-I69.8) transported by the Osaka Municipal Fire Department (OMFD) between January 1, 2016, and December 31, 2019. Patients who were transported in the same ambulance with other patients and those with missing data were excluded from the analysis. Anonymized data from the Osaka Emergency Information Research Intelligent Operation Network system (ORION), published in 2022, were used in this study (7). This manuscript was prepared according to the Strengthening the Reporting of Observational Studies in Epidemiology statement to assess the reporting of cohort and cross-sectional studies (9).
2.2. Study areaOsaka City is the largest metropolitan area in western Japan (225.33 km2), with a population of approximately 2.75 million people (10). A total of 94 medical institutions receives ambulances in Osaka City, and the total number of ambulance dispatches by the OMFD during the study period was 942,778 (11).
2.3. Telephone triage service in Osaka CityThe telephone triage service in Osaka City has been described previously (4). In summary, a telephone triage nurse assesses the urgency of a caller’s symptoms using only the telephone triage protocol for each chief complaint (4). In principle, the emergency assessment in this service does not require doctors and is not affected by patients’ requests. This telephone triage service is similar to those in the United States, Canada, and the United Kingdom (1, 12, 13). Telephone triage services and ambulance requests in Japan are public services that are free of charge. Based on patient assessments, telephone triage nurses can dispatch an ambulance or suggest an appropriate medical institution (14). The Japanese telephone triage protocol includes 98 chief complaints for adults and children, and patients are triaged according to the signs and symptoms related to the chief complaints (14). In addition, data regarding telephone triage, such as sex, patient age, time of call initiation, end time of call, chief complaint, signs, urgency assessment, and whether an ambulance was dispatched or not, are recorded using the software. During the study period, 466,744 emergency medical consultations were conducted in the Osaka prefecture, including 20,387 ambulance dispatches requested by the telephone triage nurses (14).
2.4. Ethical considerationThis study was approved by the Institutional Review Board of Osaka Metropolitan University Hospital (approval number: 2021–233). As we used anonymized data provided by the OMFD, the requirement of obtaining patients’ informed consent was waived.
2.5. Main outcomeWe defined the primary outcome of this study as the proportion of patients diagnosed with cerebrovascular disease upon arrival at the hospital by ambulance who were discharged to home on hospital day 21 (15). We wanted to consider neurological assessment as an outcome of cerebrovascular disease, but we did not have the relevant assessment information (such as Glasgow Outcome Scale and modified Rankin Scale). We assumed that home discharge outcomes were correlated with better neurological outcomes. That’s why we used discharge to home as the primary outcome. The secondary outcome was defined as survival on hospital day 21 in patients diagnosed with cerebrovascular disease upon arrival at the hospital by ambulance.
2.6. Propensity score matchingPatient propensity scores were calculated using a logistic regression model with nine variables that existed before the use of the telephone triage service or were indicative of the patient’s condition, including age, sex, calendar year, season, time, holiday (including weekends), accident location, consciousness, and administrative districts. Seasons were defined as spring from April to June, summer from July to September, autumn from October to December, and winter from January to March. The time was considered daytime from 09:00 to 17:59 and nighttime from 18:00 to 08:59. The accident locations were categorized as residences or elsewhere. Consciousness was classified using the Glasgow Coma Scale (GCS) (16) in the ambulance: severe impairment, 3–8 points; moderate impairment, 9–11 points; mild impairment, 12–13 points; and clear, 14–15 points. Administrative districts were classified into 24 areas as defined by Osaka City (17).
The effects of telephone triage service use on patient outcomes were evaluated. One-to-one pair matching was conducted by nearest-neighbor matching without replacement between patients for whom an ambulance was dispatched by the telephone triage service and for those whom an ambulance was dispatched without telephone triage, using a caliper width of 0.2 of the standard deviation of the logit of the propensity score. Covariate balances before and after matching were confirmed by comparing the standardized mean differences (SMD). An SMD < 10% was considered as a negligible imbalance between the two groups.
2.7. Statistical analysisPropensity score matching, univariate and multiple logistic regression models, and regression models with propensity scores as covariates were conducted. The variables used in the calculation of the propensity score and telephone triage services were used in the multiple regression model (Forced entry method). All statistical analyses were performed using SPSS version 25.0 J (IBM Corp. Armonk, NY, United States). All statistical tests were two-tailed, and statistical significance was defined as p < 0.05.
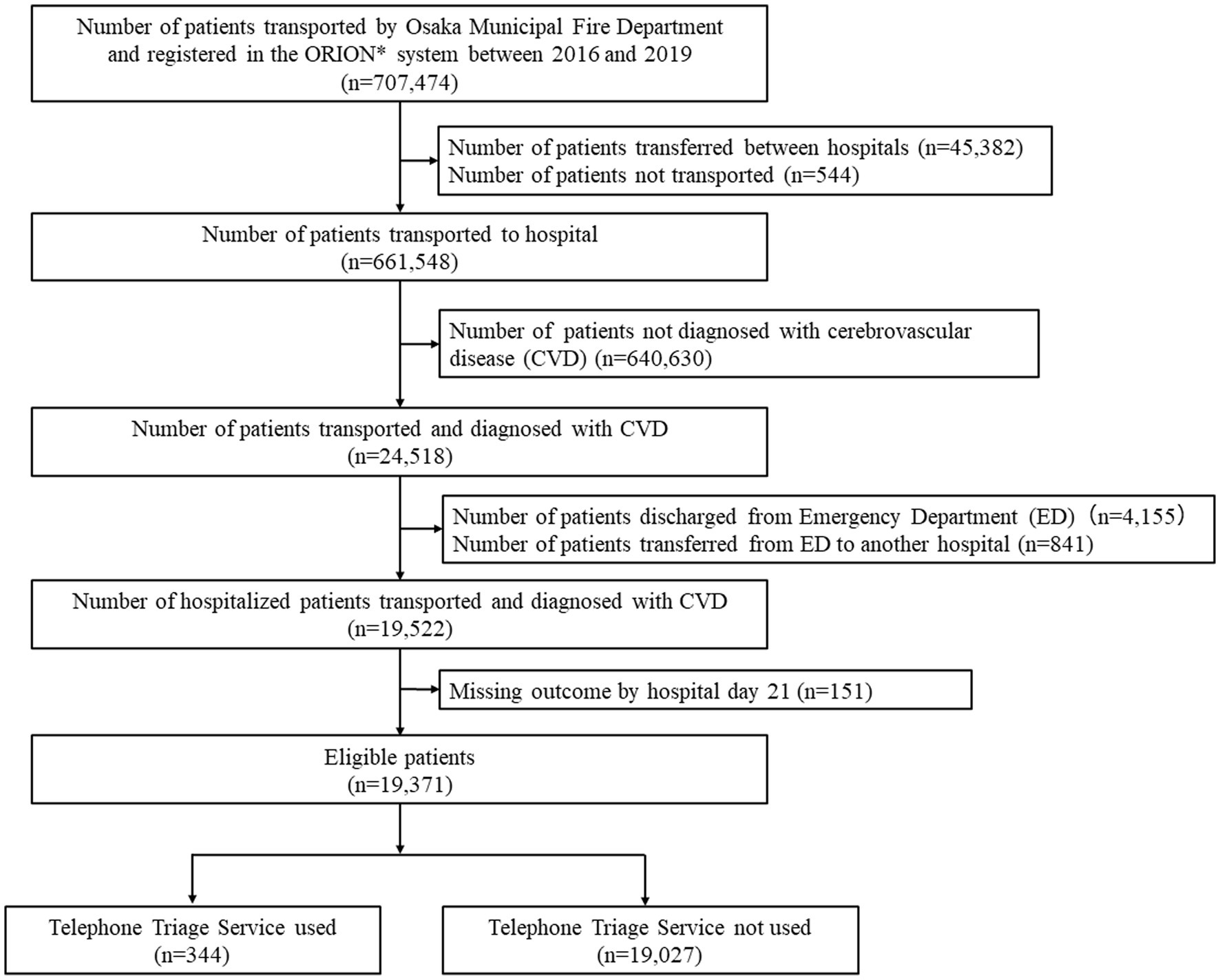
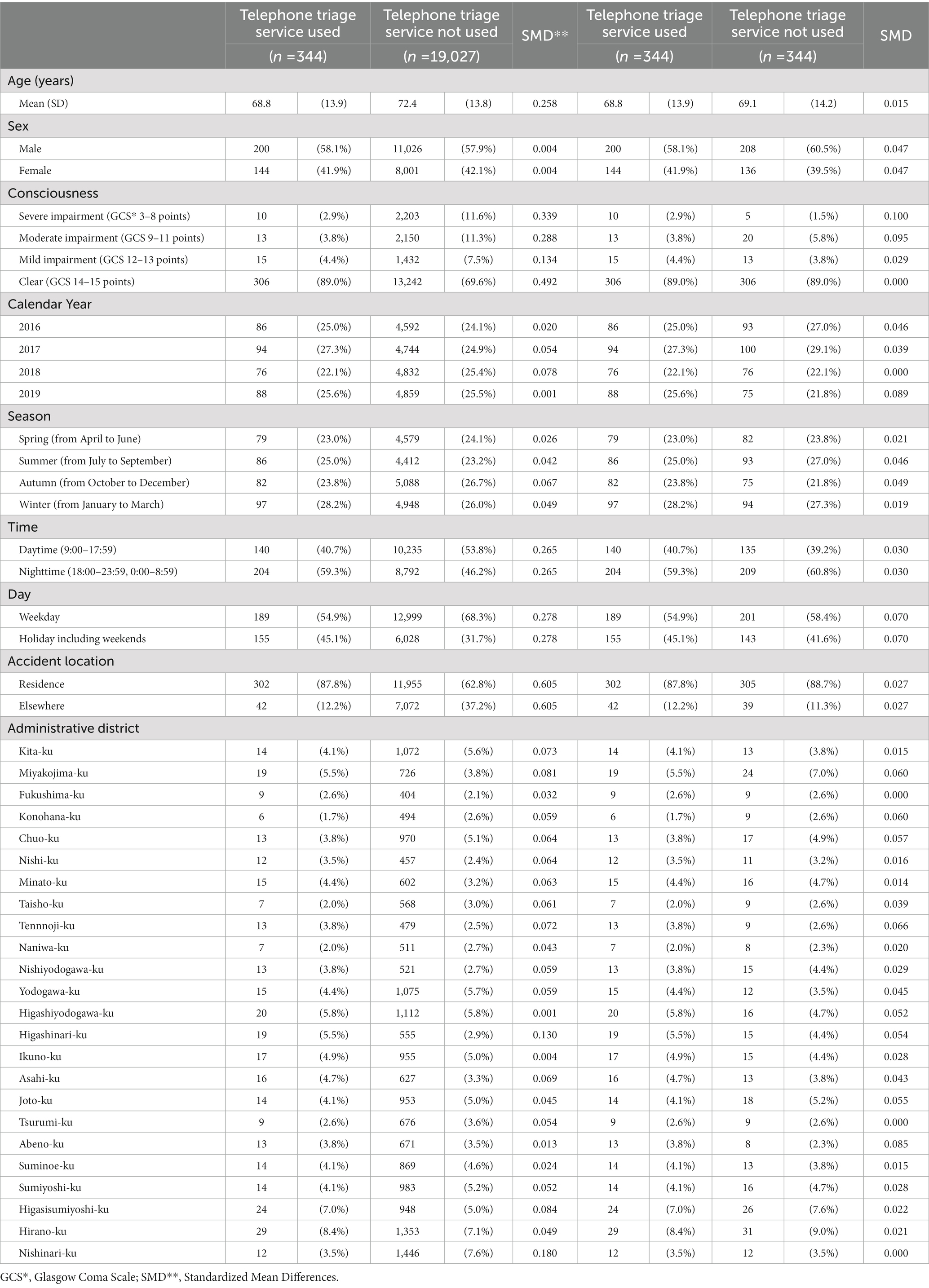
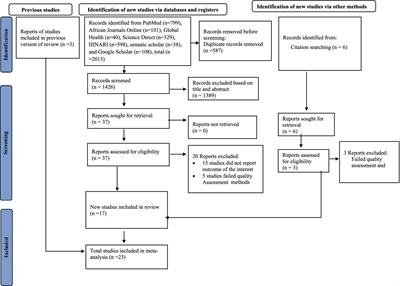
3. ResultsBetween 2016 and 2019, 707,474 patients were transported to medical institutions by OMFD ambulances and were registered in the ORION system (Figure 1). A total of 45,382 patients who were transferred between hospitals and 544 patients who were not transported were excluded from the study. Of the remaining patients, 24,518 had a diagnosis of cerebrovascular disease upon arrival at the hospital. To evaluate the inpatients’ outcomes, 4,155 patients who were discharged from the emergency department (including those who died), 841 patients who were transferred to another hospital, and 151 patients with missing data regarding hospital day 21 were excluded. Ultimately, 19,371 patients were included in this study. Of these patients, 344 (1.8%) had used the telephone triage service and 19,027 (98.2%) had not. Patients who used telephone triage services were younger and had a milder impairment of consciousness than those who did not (Table 1).
Figure 1. Patient flowchart in this study. Between 2016 and 2019, 707,474 patients were transported to medical institutions by Osaka Municipal Fire Department ambulances and were registered in the ORION system. A total of 45,382 patients who were transferred between hospitals and 544 patients who were not transported were excluded. Of the remaining patients, 24,518 had a diagnosis of cerebrovascular disease upon arrival at the hospital. To evaluate the inpatients’ outcomes, 4,155 patients who were discharged from the emergency department (including those who died), 841 patients who were transferred to another hospital, and 151 patients with missing data regarding hospital stay at day 21 were excluded. Ultimately, 19,371 patients were included in this study. Of these patients, 344 (1.8%) had used the telephone triage service and 19,027 (98.2%) had not. *ORION, Osaka Emergency Information Research Intelligent Operation Network.
Table 1. Patient characteristics before and after propensity score matching.
Approximately 90% of telephone triage service users were located at their residences. A total of 344 patients from the group that did not use the telephone triage service were matched to those who used the service using propensity score matching, and the balance of each covariate improved between the two groups after propensity score matching. The area under the curve in the logistic regression model for propensity score calculation was 0.746.
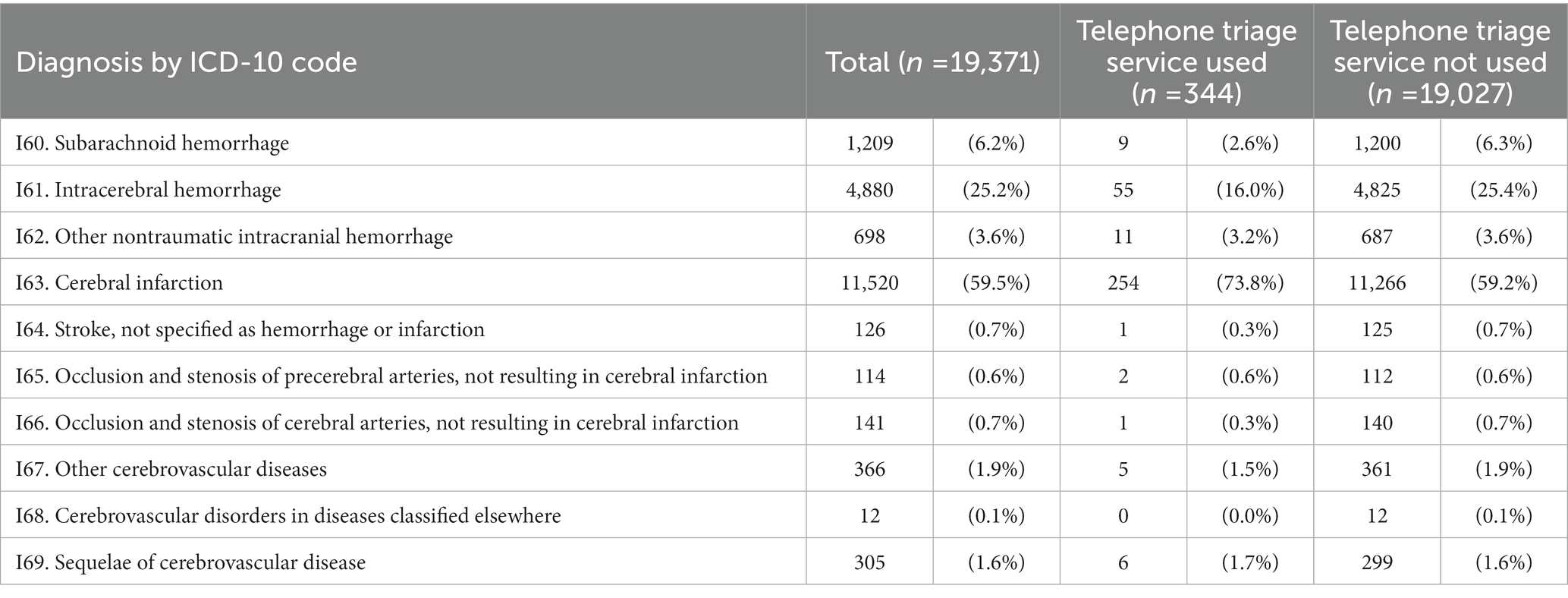
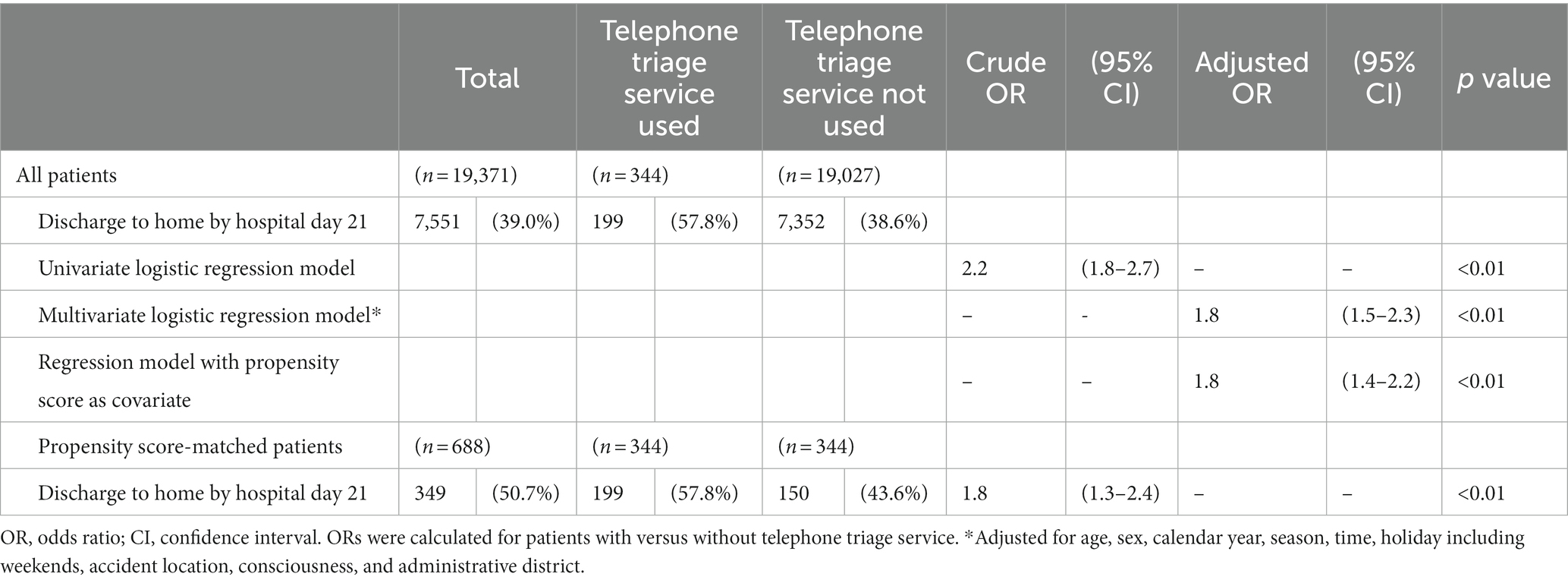
The most common cerebrovascular events diagnosed among all patients were cerebral infarction (59.5%, 11,520 patients), intracerebral hemorrhage (25.2%, 4,880 patients), and subarachnoid hemorrhage (6.2%, 1,209 patients) (Table 2). Of the 19,371 patients included in this study, 7,551 (39.0%) were discharged home by hospital day 21, including 199 (57.8%) patients who used the telephone triage service and 7,352 (38.6%) patients who did not use the telephone triage service. Telephone triage service use was associated with discharge to home by hospital day 21 (crude odds ratio [OR]: 2.2; 95% confidence interval [CI]: 1.8–2.7), and was also independently associated with discharge to home by hospital day 21 (adjusted OR: 1.8; 95% CI: 1.5–2.3). This association was also observed in the propensity score-matched analysis (crude OR: 1.8; 95% CI: 1.3–2.4) (Table 3), when the propensity score was included as a covariate (adjusted OR: 1.8 95% CI: 1.4–2.2).
Table 2. Number of hospitalized patients with cerebrovascular diseases transported by ambulance in this study.
Table 3. Discharge to home of hospitalized patients with cerebrovascular diseases transported by ambulance.
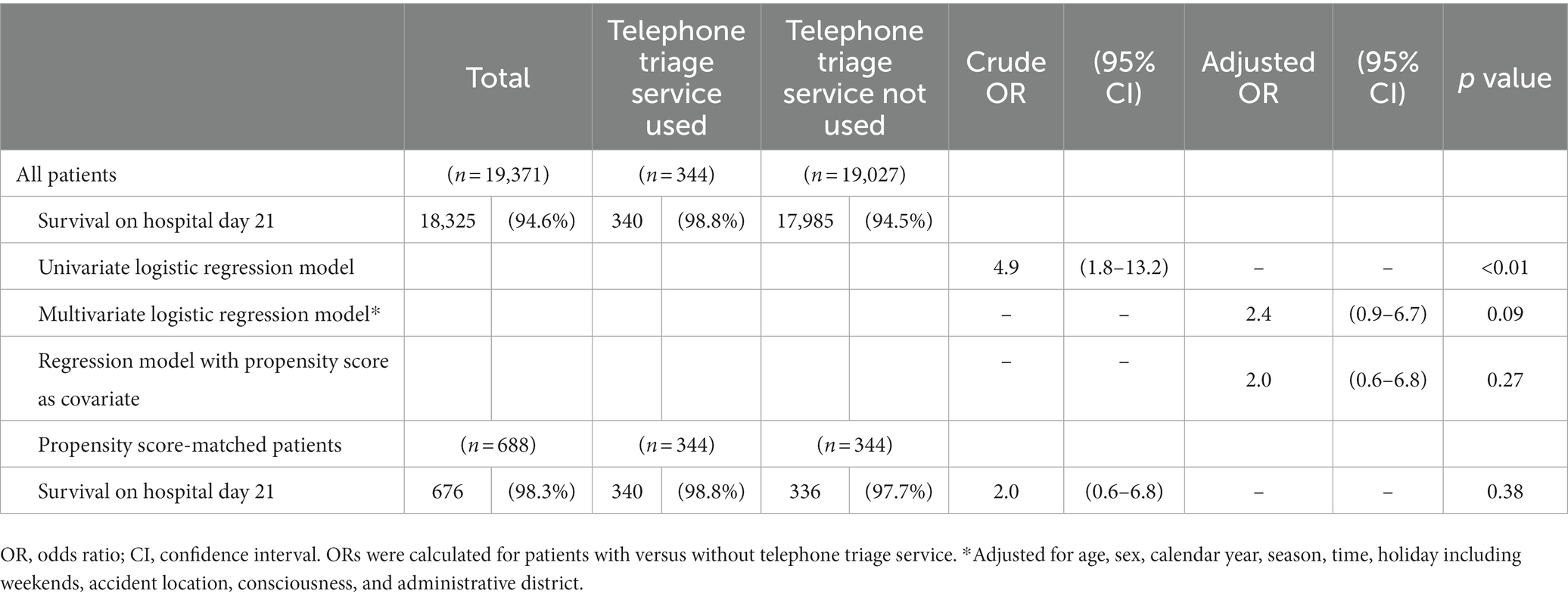
Of the 19,371 patients included in this study, 18,325 (94.6%) survived on hospital day 21, including 340 (98.8%) patients who used the telephone triage service and 17,985 (94.5%) patients who did not. Telephone triage service use was associated with survival on hospital day 21 by univariate regression model analysis (crude odds ratio (OR): 4.9; 95% confidence interval (CI): 1.8–13.2). However, telephone triage service use was not associated with survival on hospital day 21 by multivariate regression model analysis (adjusted OR: 2.4; 95% CI: 0.9–6.7). This association was also not observed when the propensity score was included as a covariate (adjusted OR: 2.0; 95% CI: 0.6–6.8) in the propensity score-matched analysis (crude OR: 2.0; 95% CI: 0.6–6.8) (Table 4).
Table 4. Survival of hospitalized patients with cerebrovascular diseases transported by ambulance.
4. DiscussionThe effects of telephone triage services on emergency care for cerebrovascular diseases in the urban areas of Japan were evaluated in this study. The most common cerebrovascular diagnosis was cerebral infarction, followed by intracerebral hemorrhage and subarachnoid hemorrhage. Among patients hospitalized with cerebrovascular diseases, telephone triage service use was associated with discharge to home by hospital day 21, which meant this service might be associated with improved neurological outcome (18). No significant associations were found between using this service and patient survival.
Previous studies have not reported the diagnoses of the patients who used telephone triage services. Therefore, it remained unclear what diseases the telephone triage service was effective for. The ORION system data includes ICD-10 coded diagnoses of patients transported by ambulance. In this study, the positive effects of telephone triage services on the outcomes of patients with cerebrovascular diseases were clarified. The prognoses of cerebral infarction, intracerebral hemorrhage, and subarachnoid hemorrhage are dependent on the time from symptom onset to treatment (19–21). Some treatments for these conditions cannot be implemented after a specific number of hours have passed from the time of symptom onset (22). Telephone triage service nurses may allow patients to receive treatment more rapidly than traditional ambulance requests, which may result in improved patient outcomes and lower medical and social security costs. While these findings may be applied worldwide, health care systems and ambulance request fees vary in different countries, which may affect the use and cost of telephone triage services.
The American Heart Association (AHA) describes the process from the onset of stroke to hospitalization as the ‘Ds’ of stroke care (23). The use of telephone triage services may shorten the detection (rapid recognition of stroke symptoms), dispatch (early activation and dispatch of emergency medical services system by calling 9–1-1), and delivery (rapid emergency medical service identification, management, and transport) processes described by the AHA. Citizens may choose to use telephone triage services that are free to the public over direct ambulance dispatch services due to the high costs associated with such services. The telephone triage service in the Osaka Prefecture used the face, arm, speech, time (FAST) acronym when triaging patients with stroke, which may have resulted in rapid and accurate ambulance dispatches. The FAST acronym is a simple screening algorithm created based on the Cincinnati Prehospital Stroke Scale (24). The algorithm identifies 88.9% of patients with stroke or transient ischemic attack and 99.9% of patients at acute onset (25). The use of telephone triage services may also shorten the time required to identify appropriate hospitals, improving the transportation process. Acute stroke is associated with a high risk of death and severe complications and requires long-term hospitalization, especially in older adults (26), and cerebral infarction is the most common disease among all hospitalized patients who arrive by ambulance (4). The findings of this study suggest that the use of telephone triage services is associated with improved outcomes in patients with cerebrovascular disease and indicates that the costs for medical expenses and disability may be greatly reduced in an aging society.
This study has several limitations. First, this study tended to include patients with mild cerebrovascular diseases. It remains unclear whether telephone triage will be useful for all severities of cerebrovascular diseases in ambulance transports. Telephone triage services may be unsuitable for patients with severe cerebrovascular diseases because it is reasonable to call an ambulance directly in such cases. Second, the outcomes of cases for which no ambulance was dispatched remain unknown. In the future, we plan to examine patients with cerebrovascular diseases for whom an ambulance was not called because of the telephone triage assessments. Third, we could not collect information related to cerebrovascular disease in this research, such as past medical history, or oral medication history. Fourth, the primary outcome of this study was discharge to home, which predicted the patients’ neurological outcomes, although it was affected by environmental factors including economic factors, such as income, and social factors, such as family composition. We were not able to adjust for these factors in this study; however, previous studies have shown that regional differences affect the outcomes of patients transported by ambulances (27), and we adjusted for this by including region-related factors as variables in the propensity score analysis. Finally, as this was an observational study, there are likely unknown confounding factors.
5. ConclusionThe use of telephone triage services is associated with improved outcomes among patients with cerebrovascular disease who are transported to hospitals by ambulance. These improved outcomes will likely reduce medical costs in an aging society.
Data availability statementThe original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving human participants were reviewed and approved by This study was approved by the Institutional Review Board of Osaka Metropolitan University Hospital (approval number: 2021–233). Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributionsYK and TS conceived the idea of this study. ST and JT contributed to the data collection. RD, HH, YN, and YK contributed to the data analysis and interpretation. RD was a major contributor in writing the manuscript. YK, TN, TK, TS, and YM supervised the conduct of this study. All authors contributed to the article and approved the submitted version.
FundingThis study was supported by the Fire and Disaster Prevention Technologies Program under Grant number JPJ000255.
AcknowledgmentsThe authors are greatly indebted to the Osaka Municipal Fire Department and the Fire and Disaster Management Agency. This article was supported by the Clinical Investigator’s Research Project of the Osaka University Graduate School of Medicine.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Turner, J, O’Cathain, A, Knowles, E, and Nicholl, J. Impact of the urgent care telephone service NHS 111 pilot sites: a controlled before and after study. BMJ Open. (2013) 3:e003451. doi: 10.1136/bmjopen-2013-003451
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Eastwood, K, Smith, K, Morgans, A, and Stoelwinder, J. Appropriateness of cases presenting in the emergency department following ambulance service secondary telephone triage: a retrospective cohort study. BMJ Open. (2017) 7:e016845. doi: 10.1136/bmjopen-2017-016845
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Katayama, Y, Kitamura, T, Hirose, T, Kiyohara, K, Ishida, K, Tachino, J, et al. Characteristics and outcome of patients triaged by telephone and transported by ambulance: a population-based study in Osaka, Japan. Acute Med Surg. (2020) 7:e609. doi: 10.1002/ams2.609
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Boggan, JC, Shoup, JP, Whited, JD, Van Voorhees, E, Gordon, AM, Rushton, S, et al. Effectiveness of acute care remote triage systems: a systematic review. J Gen Intern Med. (2020) 35:2136–45. doi: 10.1007/s11606-019-05585-4
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Katayama, Y, Kitamura, T, Nakao, S, Tanaka, K, Himura, H, Deguchi, R, et al. Association of a telephone triage service for emergency patients with better outcome: a population-based study in Osaka City, Japan. Eur J Emerg Med. (2022) 29:262–70. doi: 10.1097/MEJ.0000000000000902
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Campbell, JL, Fletcher, E, Britten, N, Green, C, Holt, TA, Lattimer, V, et al. Telephone triage for management of same-day consultation requests in general practice (the ESTEEM trial): a cluster-randomised controlled trial and cost-consequence analysis. Lancet. (2014) 384:1859–68. doi: 10.1016/S0140-6736(14)61058-8
CrossRef Full Text | Google Scholar
9. Vandenbroucke, JP, Von Elm, E, Altman, DG, Gøtzsche, PC, Mulrow, CD, Pocock, SJ, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int J Surg. (2014) 12:1500–24. doi: 10.1016/j.ijsu.2014.07.014
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Infinger, A, Studnek, JR, Hawkins, E, Bagwell, B, and Swanson, D. Implementation of prehospital dispatch protocols that triage low-acuity patients to advice-line nurses. Prehosp Emerg Care. (2013) 17:481–5. doi: 10.3109/10903127.2013.811563
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Feldman, MJ, Verbeek, PR, Lyons, DG, Chad, SJ, Craig, AM, and Schwartz, B. Comparison of the medical priority dispatch system to an out-of-hospital patient acuity score. Acad Emerg Med. (2006) 13:954–60. doi: 10.1197/j.aem.2006.04.018
CrossRef Full Text | Google Scholar
15. Okamoto, J, Katayama, Y, Kitamura, T, Sado, J, Nakamura, R, Kimura, N, et al. Profile of the ORION (Osaka emergency information research intelligent operation network system) between 2015 and 2016 in Osaka, Japan: a population-based registry of emergency patients with both ambulance and in-hospital records. Acute Med Surg. (2019) 6:12–24. doi: 10.1002/ams2.371
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Shkirkova, K, Saver, JL, Starkman, S, Wong, G, Weng, J, Hamilton, S, et al. Frequency, predictors, and outcomes of prehospital and early postarrival neurological deterioration in acute stroke: exploratory analysis of the FAST-MAG randomized clinical trial. JAMA Neurol. (2018) 75:1364–74. doi: 10.1001/jamaneurol.2018.1893
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Ohwaki, K, Hashimoto, H, Sato, M, Tokuda, H, and Yano, E. Gender and family composition related to discharge destination and length of hospital stay after acute stroke. Tohoku J Exp Med. (2005) 207:325–32. doi: 10.1620/tjem.207.325
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Hacke, W, Kaste, M, Bluhmki, E, Brozman, M, Dávalos, A, Guidetti, D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. (2008) 359:1317–29. doi: 10.1056/NEJMoa0804656
CrossRef Full Text | Google Scholar
20. Van Donkelaar, CE, Bakker, NA, Birks, J, Veeger, NJGM, Metzemaekers, JDM, Molyneux, AJ, et al. Prediction of outcome after aneurysmal subarachnoid hemorrhage. Stroke. (2019) 50:837–44. doi: 10.1161/STROKEAHA.118.023902
CrossRef Full Text | Google Scholar
21. Sporns, PB, Schwake, M, Schmidt, R, Kemmling, A, Minnerup, J, Schwindt, W, et al. Computed tomographic blend sign is associated with computed tomographic angiography spot sign and predicts secondary neurological deterioration after intracerebral hemorrhage. Stroke. (2017) 48:131–5. doi: 10.1161/STROKEAHA.116.014068
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Emberson, J, Lees, KR, Lyden, P, Blackwell, L, Albers, G, Bluhmki, E, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. (2014) 384:1929–35. doi: 10.1016/S0140-6736(14)60584-5
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Jauch, EC, Cucchiara, B, Adeoye, O, Meurer, W, Brice, J, Chan, YY, et al. Part 11: adult stroke: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. (2010) 122:S818–28. doi: 10.1161/CIRCULATIONAHA.110.971044
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Kothari, RU, Pancioli, A, Liu, T, Brott, T, and Broderick, J. Cincinnati prehospital stroke scale: reproducibility and validity. Ann Emerg Med. (1999) 33:373–8. doi: 10.1016/s0196-0644(99)70299-4
CrossRef Full Text | Google Scholar
25. Kleindorfer, DO, Miller, R, Moomaw, CJ, Alwell, K, Broderick, JP, Khoury, J, et al. Designing a message for public education regarding stroke: does FAST capture enough stroke? Stroke. (2007) 38:2864–8. doi: 10.1161/STROKEAHA.107.484329
CrossRef Full Text | Google Scholar
26. Virani, SS, Alonso, A, Aparicio, HJ, Benjamin, EJ, Bittencourt, MS, Callaway, CW, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. (2021) 143:e254–743. doi: 10.1161/CIR.0000000000000950
CrossRef Full Text | Google Scholar
27. Marfil-Garza, BA, Belaunzaran-Zamudio, PF, Gulias-Herrero, A, Zuñiga, AC, Caro-Vega, Y, Kershenobich-Stalnikowitz, D, et al. Risk factors associated with prolonged hospital length-of-stay: 18-year retrospective study of hospitalizations in a tertiary healthcare center in Mexico. PLoS One. (2018) 13:e0207203. doi: 10.1371/journal.pone.0207203
留言 (0)