

記住我








Total anomalous pulmonary venous connection (TAPVC) is a relatively rare cyanotic congenital heart disease, accounting for approximately 0.5%–2% of postnatal congenital heart diseases, in which all pulmonary veins (PVs) are not connected to the left atrium (LA) but directly or indirectly to the right atrium (RA) (1). According to different drainage pathways, TAPVC can be divided into four types: supracardiac, intracardiac, infracardiac, and mixed, with supracardiac type being the most common malformation and accounting for about 43% of all cases (2). TAPVC can occur alone or can accompany other deformities, and the most common comorbidity is right atrium isomerism (RAI) (3). Postnatally, TAPVC neonates often suffer from severe expiratory dyspnea, cyanosis, heart failure, etc. In case of pulmonary vein obstruction (PVO) complication, prompt emergency surgery is required; otherwise, most would die in the neonatal period. The prognosis of TAPVC is related to the specific subtypes, the presence of PVO, and associated malformations (4, 5). Therefore, an accurate prenatal diagnosis of TAPVC is of great significance for neonatal prognosis.
To date, the accuracy of TAPVC diagnosis varies significantly across different countries, regions, and institutions (3, 6). Some new ultrasound indicators or methods have been proposed to improve the prenatal diagnosis of TAPVC. For instances, post-LA space has been suggested as a potential indicator for prenatal diagnosis of TAPVC in many studies (7, 8). A four-dimensional spatiotemporal image correlation has been used to diagnose fetal TAPVC (9). Additionally, fetal PV variability index and vertical vein (VV) flow velocity have shown to predict postpartum PVO (10). Artificial intelligence can also be used to assist in diagnosing TAPVC (11). The routine prenatal screening has also identified pulmonary venous connections on a four-chamber view (12). Available literature demonstrates that prenatal screening, color Doppler, and spectral Doppler can identify 80% of suspected TAPVC, 34% of PVO, 59% of ventricular imbalance, 58% of increased LA posterior space, and 59% of VV cases (3). However, much remains to be desired with regard to a systemic assessment of TAPVC.
Given that the detection of PVO and the identification of its drainage pathway, an indispensable procedure of ultrasound diagnosis, are related to the prognosis of neonates with TAPVC, we proposed a four-step ultrasound approach to diagnose fetal TAPVC systematically, which demonstrated a favorable accuracy in prenatal diagnosis of TAPVC. The proposed method can provide a reliable support for prenatal consultation and clinical decision-making.
Materials and methodsA total of 62 TAPVC fetuses underwent prenatal ultrasound examination in the Fujian Maternal and Child Health Hospital between June 2012 and June 2022, and were confirmed by postnatal echocardiography, surgical procedures, or postabortion autopsy. The clinical data and imaging findings of these TAPVC cases were retrospectively analyzed. Inclusive criteria were as follows: the fetuses with TAPVC were examined by systematic ultrasonography and verified by the above-mentioned means in our hospital. The exclusion criteria were as follows: the fetuses with TAPVC that were not verified postnatally or pathologically; RAI cases that indicated the entry of PV into the atrium; or cases that reported incomplete clinical data or no follow-up. The study protocol was reviewed and approved by the Ethics Committee of the Fujian Maternal and Child Health Hospital. Informed consent was obtained from all pregnant women.
Prenatal ultrasonographyFor prenatal ultrasonography, GE Voluson E8 and E10 high-resolution color Doppler ultrasound diagnostic instruments were employed, with the frequency of the convex array probe set at 2–9 MHZ, and the conditions of middle and late pregnancy and fetal heart examination were selected. The fetuses were systematically evaluated following the ISUOG guidelines for the prenatal ultrasonography (13, 14). TAPVC was suspected with the presence of any of the following signs: a small LA, an increased distance from the LA to the descending aorta, a smooth posterior wall of the LA, unobservable orifices of the PV, evident extra vessels and centrifugal venous flow in some sections of the heart, and an abnormal dilated vein [e.g., superior vena cava (SVC), innominate vein (INN), azygos vein (AZV), inferior vena cava (IVC), or coronary sinus (CS)]. The suspected TAPVC cases were further assessed by a four-step ultrasound procedure: (1) no connection was observed between all the PVs and the LA, in which the orifices of the PV were detected by two-dimensional echocardiography and color Doppler flow imaging, and the waveform of the PV was examined by spectral Doppler imaging; (2) the presence of the common pulmonary vein (CPV) was detected behind and beside the LA, and the drainage route of PV to the systematic vein via the CPV and VV was traced, on which the classification of TAPVC was based; (3) the presence and location of obstruction of the pulmonary venous drainage pathway were assessed by color Doppler and spectral Doppler imaging, in which color Doppler flow imaging may indicate turbulent blood flow at the site of obstruction, with a maximum flow velocity above 50 cm/s (15); (4) the fetal cardiac structures and extracardiac systems were examined in detail to determine the presence of intracardiac and extracardiac malformations.
Postnatal verificationAll the prenatally diagnosed fetal TAPVC cases underwent a multidisciplinary consultation. For cases of termination of pregnancy (TOP), autopsy was performed, with informed consent obtained from the parents, by either local anatomy or combined casting of the thoracic and abdominal organs, in which all specimens were archived, photographed, videotaped, and recorded. For live births, echocardiography or other imaging examinations were performed postnatally, in which Phillips EPIQ 7C was employed for neonatal echocardiography, with the frequency of phased array probes set at 3–8 MHz. These live births all received follow-ups.
Statistical analysisThe data were analyzed with SPSS 25.0. The quantitative data displayed a normal distribution with homogeneous variance and were expressed as mean ± SD. For qualitative data, frequency (N) and percentage (%) were used. Comparisons were analyzed by the chi-square test with continuity correction. A value of P <0.05 was considered statistically significant.
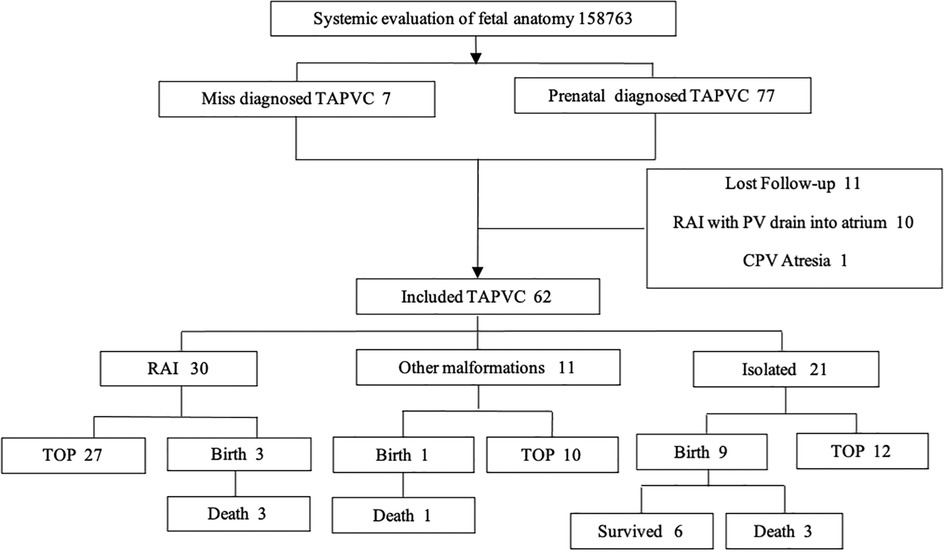
Results Data overviewFrom June 2012 to June 2022, 158,763 pregnant women received prenatal ultrasonography and 84 cases of TAPVC were identified (5‰). Among them, the following cases were excluded from the study: 11 cases of loss to follow-up, 1 case of CPV atresia by postnatal autopsy, and 10 cases of RAI with PV entry into the atrium; 50 cases received TOP, of which 49 were confirmed as TAPVC by local pathological anatomy or combined casting of organs in thoracic and abdominal cavity; 6 cases chose to continue pregnancy and 7 were missed to be diagnosed prenatally. Live TAPVC infants suffered from cyanotic and respiratory distress, and the diagnosis was confirmed by echocardiography. Finally, 62 cases were included in the study (Figure 1). The mean age of the 62 pregnant women was 27.7 ± 3.5 years (19–36 years), and the mean gestational age (GA) was 25.56 ± 3.95 weeks (20.3–38 weeks). Of the 62 fetuses, 59 were singleton pregnancies and 3 were twin pregnancies (one of the fetuses was TAPVC). Among the 13 live TAPVC births, 4 infants died in the neonatal period without operation and 9 infants underwent surgery, including 5 total recoveries, 1 survival but with complication of SVC obstruction and collateral circulation, and 3 deaths after surgery.
Figure 1. Flowchart of the enrollment in the study.
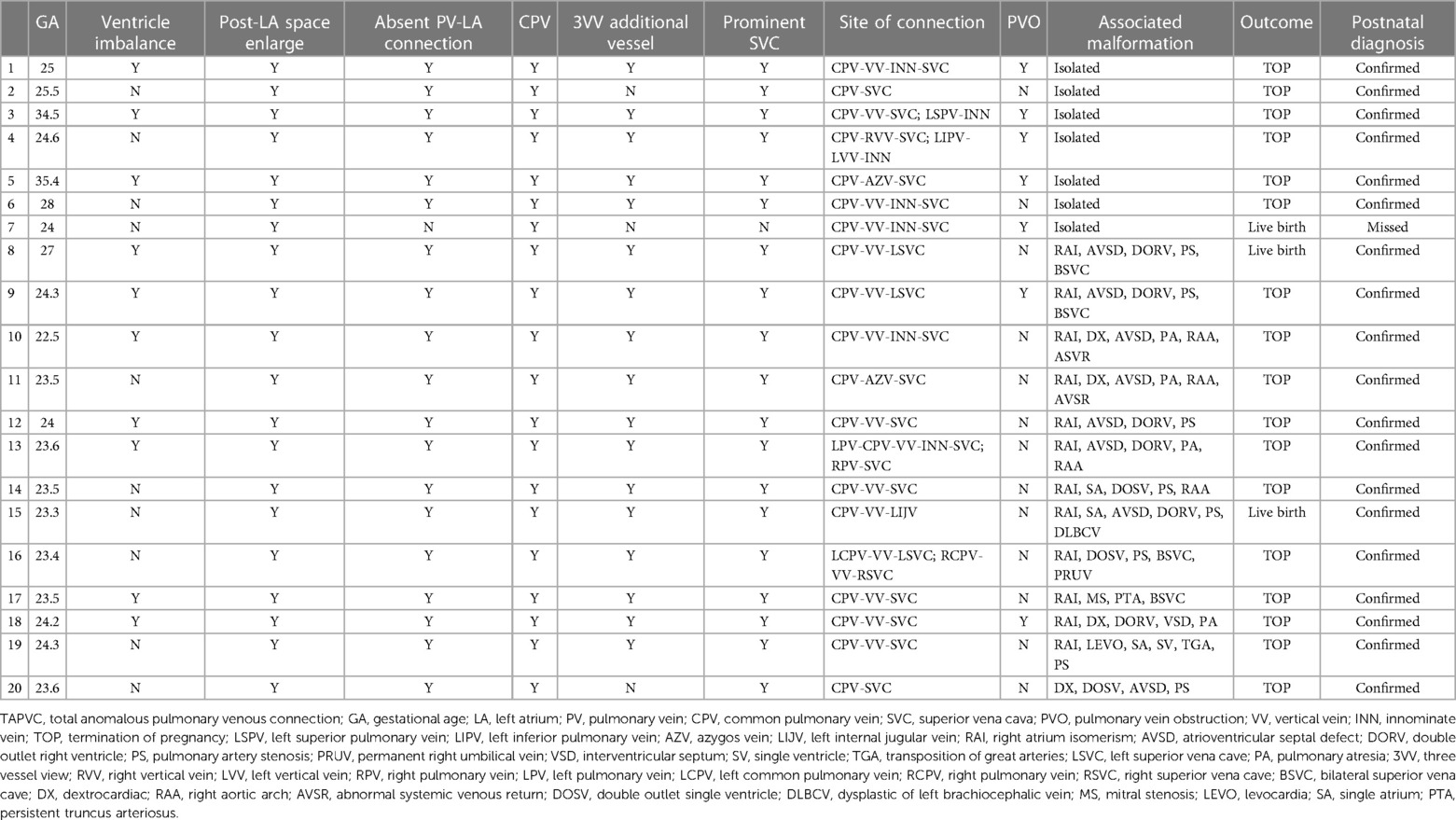
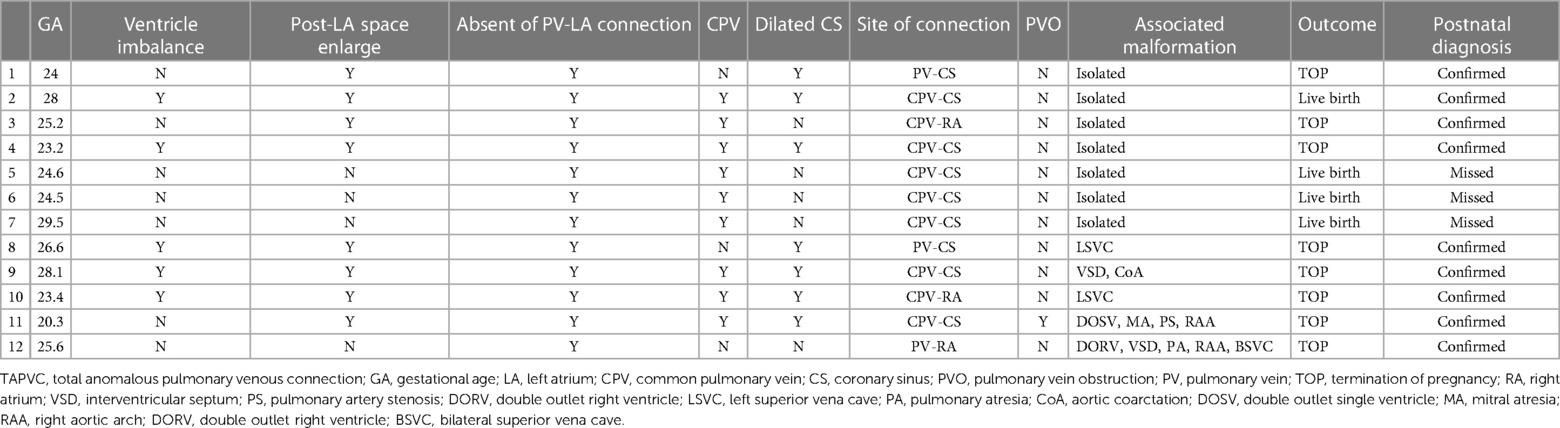
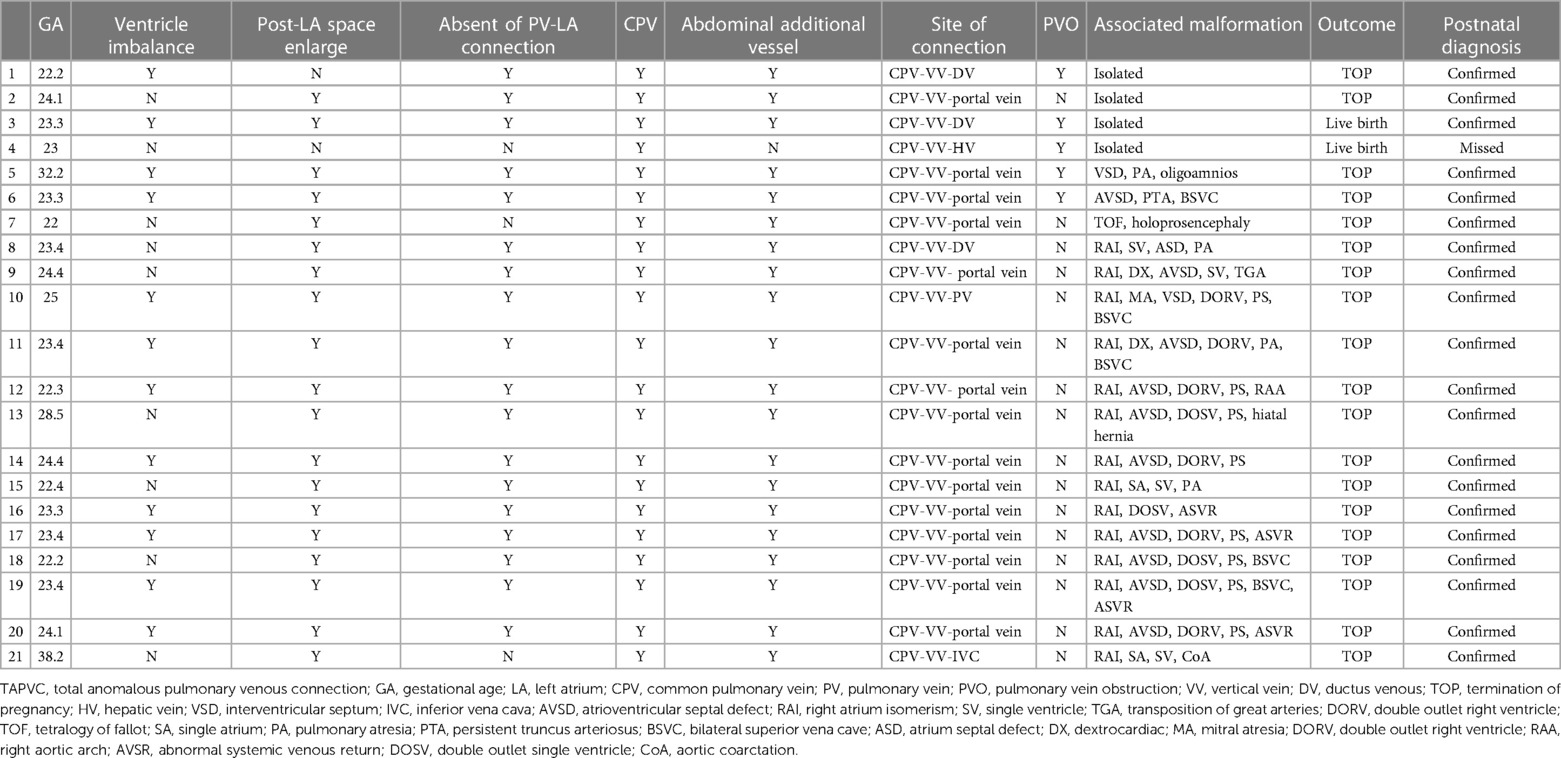
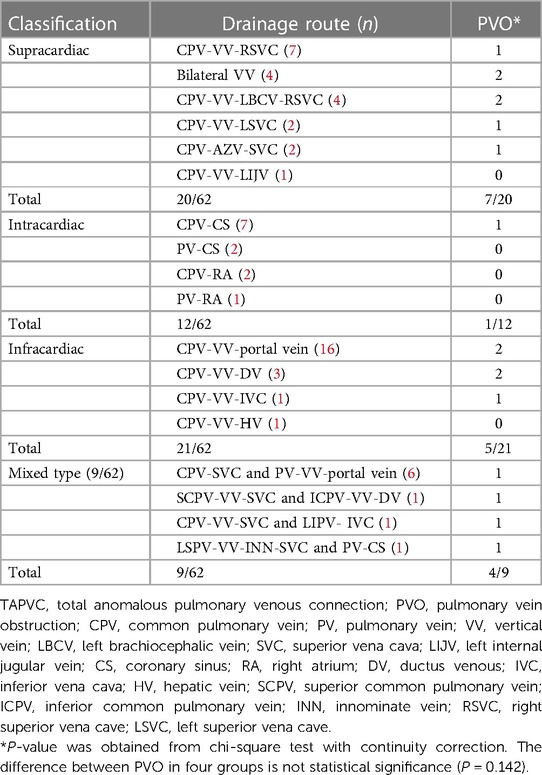
Classification and sonographic characterization of TAPVCOf the 62 TAPVC cases, there were 20 supracardiac cases (32%), 12 intracardiac cases (19%), 21 infracardiac cases (34%), and 9 cases of mixed type (15%). Of the 20 cases of supracardiac TAPVC, CPV and single VV were found in 16 cases, of which 9 cases finally regurgitated into SVC, 4 into INN, 2 into AZV, 1 into left internal jugular vein (LIJV), and double VVs were reported in the remaining four cases, which regurgitated into SVC and INN (Table 1). Of the 12 cases with intracardiac TAPVC, 9 cases regurgitated into the RA through the CS and 3 cases drained directly into the RA (Table 2). Of the 21 cases of infracardiac TAPVC, 16 cases drained into the portal vein, 3 cases into ductus venous (DV), 1 into the hepatic vein (HV), and 1 into IVC (Table 3). Of the 9 cases of mixed TAPVC, 8 cases were combined with supracardiac and infracardiac drainage and 1 case was combined with supracardiac and intracardiac drainage (Table 4).
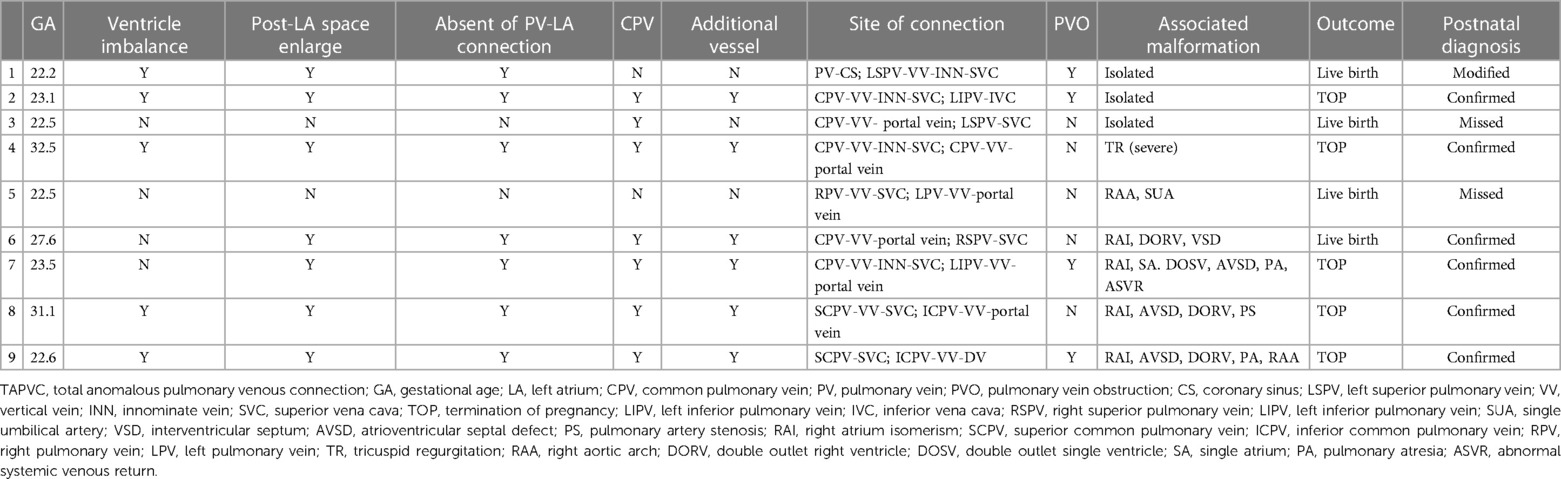
Table 1. Prenatal sonographic findings of supracardiac TAPVC.
Table 2. Prenatal sonographic findings of intracardiac TAPVC.
Table 3. Prenatal sonographic findings of infracardiac TAPVC.
Table 4. Prenatal sonographic findings of mixed TAPVC.
The common sonographic characteristics of TAPVC included small LA, smooth posterior wall of the LA, no PV orifice, increased distance between the LA and the descending aorta, and a continuous flow spectrum of the PV. CPV was shown in 56 cases, which appeared as an additional vessel behind or beside the LA. The sonographic image varied for different types of TAPVC. The supracardiac TAPVC featured an ascending VV, which was an additional vessel on a three-vessel trachea view and appeared as a centrifugal venous flow with dilated drainage site via color Doppler flow imaging (Figure 2). Echocardiographic findings of intracardiac TAPVC showed that the CPV either flew back into the RA through dilated CS or drained directly into the RA (Figure 3). The sonographic appearance of infracardiac TAPVC revealed a descending VV, an additional vessel in the transverse section of the abdomen, which appeared as a downward centrifugal vessel into the liver along with the IVC and the descending aorta in the sagittal section of the abdomen (Figure 4). Mixed TAPVC displayed multiple anomalous pulmonary venous drainage pathways, featuring two or more of the above ultrasonic findings (Figure 5).
Figure 2. The prenatal sonographic features of supracardiac TAPVC. (A) The posterior wall of LA was smooth without orifice of PV, the pulmonary venous confluence behind the LA. (B) The left and right PVs converging to form a common PV truck, the CPV going upward as VV. (C) The VV drained into the SVC via the LBCV. (D) The entire drainage route of PVs. TAPVC, total anomalous pulmonary venous connection; PV, pulmonary vein; LA, left atrium; CPV, common pulmonary vein; VV, vertical vein; SVC, superior vena cava; LBCV, left brachiocephalic vein.
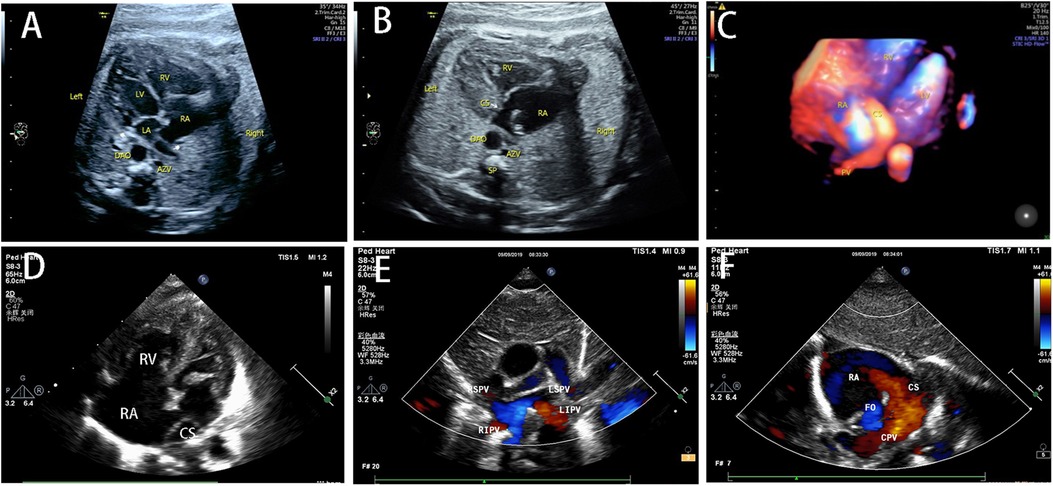
Figure 3. The prenatal and postnatal sonographic features of intracardiac TAPVC. (A) The four-chamber view showed ventricular discrepancy and no connection between PVs and LA. (B) The PVs drained into RA via dilated CS. (C) The entire drainage route of anomalous PVs. (D) The obvious asymmetry on the four-chamber view after birth. (E) All the PVs were not connected with LA. (F) The CPV drained into RA via dilated CS. TAPVC, total anomalous pulmonary venous connection; PV, pulmonary vein; LA, left atrium; RA, right atrium; CPV, common pulmonary vein; CS, coronary sinus.
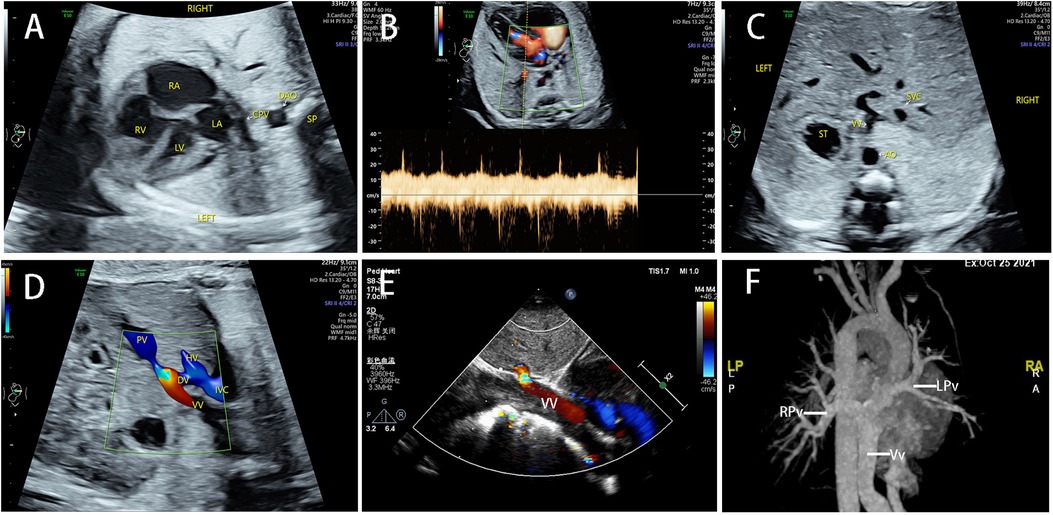
Figure 4. The sonographic features of infracardiac TAPVC and postnatal confirmation. (A) CPV was located behind the LA, with an increased posterior left atrium space. (B) The Doppler spectrum of PV was continuous instead of pulsatile. (C) The VV appeared as an extra vessel in the transabdominal section. (D) The VV drained into DV in a turbulent flow. (E) The obstruction was confirmed postnatally. (F) The CTA showed the entire drainage route of PVs. TAPVC, total anomalous pulmonary venous connection; PV, pulmonary vein; LA, left atrium; CPV, common pulmonary vein; VV, vertical vein; DV, ductus venous; CTA, computerized tomographic angiography.
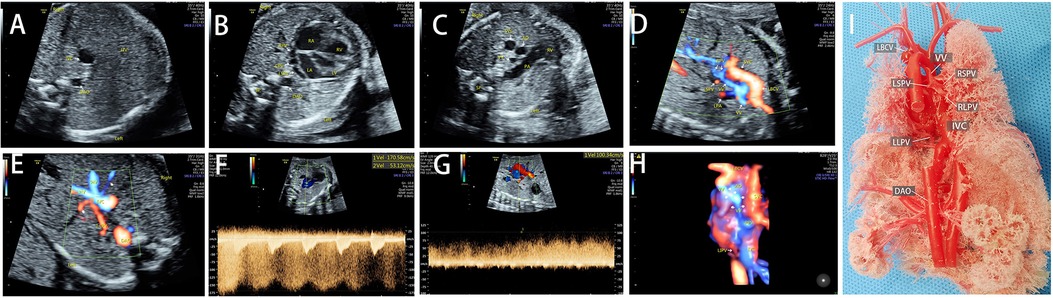
Figure 5. The sonographic features of mixed TAPVC and postnatal anatomic cardiovascular casting findings. (A) A dilated IVC in transabdominal section. (B) The ventricles were asymmetrical and the CPV was located behind the LA. (C) The VV appeared as an extra vessel behind the aorta. (D) The color Doppler showed the drainage of the RSPV, RLPV, and the LSPV into the LBCV via VV. (E) The LLPV drained into IVC. (F,G) Obstruction was confirmed in both the supracardiac and infracardiac pathways. (H) The entire drainage route of all PVs. (I): The postnatal casting of the TAPVC heart showed the RSPV, RLPV, and LSPV drainage into LBCV via the VV, and the LLPV drainage into the IVC. TAPVC, total anomalous pulmonary venous connection; IVC, inferior vena cava; CPV, common pulmonary vein; LA, left atrium; VV, vertical vein; RSPV, right superior pulmonary vein; RLPV, right low pulmonary vein; LSPV, left superior pulmonary vein; LBCV, left brachiocephalic vein; LLPV, left low pulmonary vein.
The obstruction of pulmonary veins in fetal TAPVCOf the 62 cases of TAPVC, 17 cases were complicated with PVO, including 7 cases of supracardiac type (42%), 5 cases of infracardiac type (29%), 4 cases of mixed type (24%), and 1 case of intracardiac type (6%), with no statistical PVO difference among the different groups of TAPVC (P > 0.05) (Table 5). Among the seven supracardiac TAPVC cases, five cases reported PVO at the opening of the ascending VV into the SVC, one case at the opening of the ascending VV into the AZV, and one case at the VV crossing the bifurcation of the pulmonary artery. Of the five infracardiac TAPVC cases, the obstruction was located at the confluence of the descending VV into the DV in three cases and at the confluence of the descending VV into the PV in two cases. In the intracardiac TAPVC case, four PVs formed a CPV and the VV were tortuous, in which the obstruction was located at the bifurcation of pulmonary artery and confluent to the CS. Of the four cases of mixed TAPVC, three cases reported a mixture of supracardiac and infracardiac TAPVC, in which the obstruction occurred during the infracardiac drainage when the descending VV entered the IVC, portal vein, and DV, and one case displaying obstruction in the supracardiac route, with the ascending VV crossing the left pulmonary artery. The remaining case displayed a mixture of intracardiac and supracardiac TAPVC, in which the obstruction was found in the supracardiac and intracardiac pathways, respectively, at the point where the left inferior pulmonary vein (LIPV) joined the CPV and at the point where the VV joined the INN. All the PVO cases displayed the sonographic features of the tortuous and slender obstructive site, with turbulent blood flow by color Doppler imaging and continuous high-speed blood flow by spectrum Doppler imaging at a maximum velocity of 110 ± 33 cm/s (58–170 cm/s).
Table 5. The drainage route and obstruction of TAPVC.
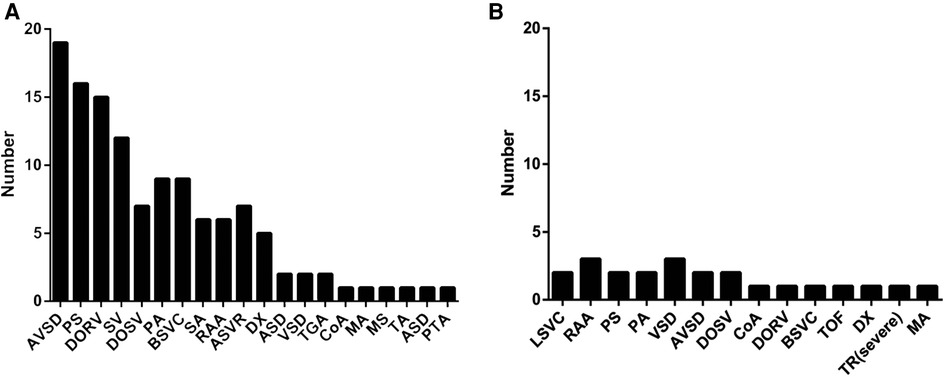
The associated malformations of the fetal TAPVCOf the 62 TAPVC cases, 41 cases were complicated with other intracardiac and extracardiac malformations, including 30 RAI cases and 11 cases with other intracardiac and extracardiac malformations, and the remaining 21 cases were isolated TAPVC. In the 30 TAPVC cases combined with RAI, the common concomitant malformations included atrioventricular septal defect (AVSD) (19/30), pulmonary artery stenosis (PS) (16/30), double outlet right ventricle (DORV) (15/30), single ventricle (SV) (12/30), etc., and the rare complicated malformations were interventricular septum (VSD) (2/30), transposition of great arteries (TGA) (2/30), etc. (Figure 6A). In the 11 TAPVC cases complicated with other cardiac malformations, common concomitant malformations were VSD (3/11), right aortic arch (3/11), left superior vena cave (LSVC) (2/11), PS (2/11), etc. (Figure 6B). TAPVC cases combined with extracardiac malformations displayed cleft lip and palate, holoprosencephaly, hiatal hernia, oligohydramnios, and permanent right umbilical vein (PRUV), one case per category, and single umbilical artery (SUA) in two cases. Of the 62 TAPVC cases, seven cases underwent chromosome tests, which reported chromosome normality in six cases and inversion of chromosome 9 in one case.
Figure 6. Obvious differences of the associated intracardiac malformations between TAPVC with RAI (A) and without RAI (B). TAPVC with RAI is usually associated with a series of complex intracardiac anomalies and TAPVC without RAI can be isolated or accompanied with other anomalies. TAPVC, total anomalous pulmonary venous connection; right atrium isomerism.
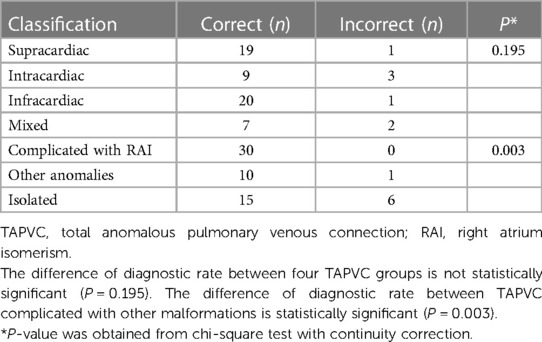
The diagnostic accuracy of the four-step prenatal ultrasonographyOf the 62 cases of TAPVC, the diagnostic accuracy of the four different TAPVC types by the four-step prenatal ultrasonography was 95%, 75%, 95%, and 77%, respectively, with no statistical significance (P > 0.05) (Table 6). Thirty cases complicated with RAI and 10 cases combined with other intracardiac and extracardiac abnormalities were correctly diagnosed by the proposed prenatal ultrasonic procedure, while 1 case was missed, which was a mixed type (supracardiac and infracardiac) with right aortic arch and SUA. Of the 21 isolated cases of TAPVC, 14 cases were correctly diagnosed; 1 case was diagnosed as intracardiac type prenatally, which was postnatally confirmed to be a mixed type (supracardiac and intracardiac) with obstruction of the supracardiac and intracardiac drainage pathway by echocardiography; 6 cases were missed. As shown in Table 6, the proposed four-step prenatal ultrasonography reported a higher accuracy in diagnosing TAPVC cases that were complicated with RAI (P < 0.05).
Table 6. Comparison of the diagnostic rate of different types of TAPVC and comparison of the diagnostic rate of TAPVC complicated with other malformations.
DiscussionPrenatal diagnosis of TAPVC has always been a great challenge, especially in isolated cases (16). Due to its low incidence and difficulty in obtaining detailed images, it is rarely detected during obstetric screening in the second trimester of pregnancy (17). Diagnostic accuracy has been improved thanks to sonographic advances and experience accumulation in the past decade. Several retrospective studies have documented many suspicious signs of TAPVC during prenatal ultrasound screening, including a small LA, lengthened distance between the LA and the descending aorta, the smooth posterior wall of the LA, obscured orifices of the PV, additional vessels in some sections, centrifugal venous flow, and dilatated fetal systemic veins (e.g., SVC, INN, AZV, IVC, or CS) (15). When the above-mentioned suspicious TAPVC diagnostic clues appear, the use of prenatal ultrasound four-step observation can help improve the diagnosis and classification of TAPVC, especially when TAPVC is associated with other malformations. In this article, we found that after postpartum validation or pathological comparison, the prenatal correct diagnosis rates of the supracardiac, intracardiac, infracardiac, and mixed types were 95%, 75%, 95%, and 77%, respectively. Thirty TAPVC cases with RAI were accurately detected by the proposed prenatal ultrasonography, though one case of TAPVC with other extracardiac and intracardiac malformations was missed. Six cases of isolated TAPVC were missed. The potential explanation for missed diagnosis may lie in the following considerations: (1) The entry of fetal PV into the LA is falsely identified during the examination, since the echoes of bronchial and pulmonary arteries may interfere with the orifices of the PVs at the top of the LA and may be mistaken for the connection with the LA; (2) Due to the small size of the fetal PV, the fetal position, and the thickness of abdominal wall of the pregnant woman, two-dimensional ultrasonography may not clearly delineate the lumen of the PV; (3) The dilated systemic veins and VV in the drainage site were overlooked because of inexperience. These weaknesses may be remedied by adjusting the blood flow velocity scale to about 20 cm/s during color Doppler flow imaging and verifying the connection by spectrum Doppler imaging. In addition, an extra vessel in the trachea section or abdominal cross-section is an important indicator for TAPVC diagnosis.
Of the four types of TAPVC, the infracardiac and mixed types of TAPVC have a poor prognosis (18). Even for the same type, the prognosis differs for different drainage paths. For example, for different subtypes of supracardiac TAPVC, direct access to the right SVC via the right VV is more likely to result in postoperative PVO (19). The prognosis of intracardiac TAPVC is generally considered good (20). In this study, four cases of isolated intracardiac TAPVC had a good prognosis after surgical treatment. However, the prognosis of intracardiac TAPVC varies for different sites of connection. Studies have shown that the number of PV orifices, the length of the drainage path, and the drainage through the roof of the RA are associated with postoperative PVO (21). Therefore, the prenatal diagnosis of TAPVC should delineate not only the type of TAPVC but also the specific connection of ectopic PV and the length of the drainage path.
PVO is also an essential factor for a poor prognosis, and preoperative PVO is closely associated with mortality (18, 22). The available literature indicates that preoperative PVO occurs in approximately 25%–50% of cases (23, 24) and the incidence of PVO in prenatal TAPVC fetuses is as high as 34.1% (95% CI: 22.7%–47.7%) (3), signifying that one-third of the cases are likely to show evidence of prenatal obstruction. Our cohort found PVO in 17 cases (17/62, 27.4%): prenatally in 14 cases and postnatally in 3 cases. The disparity may be attributed to the following facts: as, in the current study, the average GA for the prenatal diagnosis was 25.56 ± 3.95 weeks (20.3–38 weeks) and most cases were diagnosed in the second trimester, the minor pulmonary blood flow may result in unnoticeable or no obstruction while with the progression of gestation, the increase in pulmonary blood flow may induce the obstruction; most cases in the current study received induced labor after TAPVC diagnosis and no follow-up was conducted in late pregnancy. Therefore, fewer PVO cases were diagnosed in this cohort.
PV stenosis is often caused by insertion site stenosis and external organ compression, and the longer the drainage path is, the more likely it is to be obstructed. PVO can occur at any site and aggravate during pregnancy, especially when pulmonary vascular resistance decreases, leading to increased blood flow (25). PVO can also lead to PV remodeling and even progress to atresia (26). Studies have suggested that an earlier occurrence of PVO may indicate a poorer prognosis, as it will lead to pulmonary vascular remodeling and may even compromise the efficacy of a successful surgery (26). In this study, of the 13 live births, 4 PVO infants died in the neonatal period and the prognosis of fetuses without PVO was good. Therefore, PVO should rank as an essential part of prenatal TAPVC evaluation.
TAPVC can be combined with a series of intracardiac and extracardiac malformations. The complication with RAI, one of the most common malformations in TAPVC, is associated with a worse prognosis due to faster disease progression and a greater chance of multi-operation after repair of the PV (27). In our cohort, 30 cases (30/62, 48%) were complicated with RAI. RAI is characterized by complex intracardiac abnormalities, such as incongruent visceral atria position, complete AVSD, DORV, and right ventricular outflow tract obstruction (28). Due to the bilateral right atrial structure, evaluation of pulmonary venous return is an important step in diagnosing RAI (29, 30). In addition to RAI, TAPVC may be associated with other extracardiac and intracardiac malformations, such as TGA, tetralogy of fallot (TOF), single atrium (SA), persistent truncus arteriosus (PTA), tricuspid atresia (TA), hypoplastic left heart syndrome, pulmonary atresia (PA), VSD, aortic coarctation (CoA), and other abnormalities (25). In this cohort, 11 cases were complicated with other intracardiac or extracardiac malformations. The associated anomalies, especially complex intracardiac anomalies that require secondary surgery, are also associated with a poor prognosis of TAPVC. Some deformations require no remedy or can be simultaneously corrected during the repair of the PV, in which the deformation may not be a risk factor for postoperative death (5).
The mode of inheritance of TAPVC remains unknown. However, it may be a single gene inheritance according to the existent literature (25). In the affected families, the abnormal pulmonary venous connection is a common characteristic, but the location of the abnormal connection is inconsistent (31). TAPVC is associated with several syndromes, such as asplenia, polysplenia, and Cat's eye syndrome (25). In the current study, the chromosome examination of seven cases revealed chromosome 9 inversion in one case and no abnormality in the other six cases.
LimitationSeveral limitations should be noted in the current study. First, as a retrospective study, the archived images may affect the quality and integrity of data sources. Second, the sample size is quite small. In this study, only 13 TAPVC fetuses were retrieved for analysis, which was unfavorable for evaluating the prognosis of TAPVC. Third, the accuracy of the proposed four-step prenatal ultrasonography may be compromised by the complexity of the enrolled cases, in which the RAI complication and isolated TAPVC may confound the results of the analysis. Finally, a more detailed spectrum analysis of the VV and anomalous PV should be provided.
ConclusionsThe proposed four-step ultrasonography can satisfactorily delineate fetal TAPVC classification, the presence of PVO, and intracardiac and extracardiac abnormalities, which offers beneficial support for prenatal counseling and prognostic improvement of postnatal TAPVC. The retrospective analysis also reveals that isolated TAPVC is more prone to be missed in diagnosis.
Data availability statementThe original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Ethics statementThe studies involving human participants were reviewed and approved by Ethics Committee of Fujian Maternal and Child Health Center. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the individual(s), and minor(s)' legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author contributionsXQ and ZW designed and supervised the study. XX, QW, and MX worked on the literature review. ZW, QW, SG, XX, and WL focused on imaging acquisition, data collection, and analysis. XX performed the statistical analysis. QW, XX, and MX drafted the manuscript. HM, ML, and BH worked on the editing. All authors contributed to the article and approved the submitted version.
FundingThis publication was supported by Joint Funds for the Innovation of Science and Technology, Fujian province (2020Y9156); this publication was also supported by Fujian Natural Science Foundation (2021J01420).
AcknowledgmentsThe authors thank for the support from Department of Pathology, Department of radiology, and Department of Obstetrics, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, China. We also thank all the patients and families for their understanding and support.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References2. Tongsong T, Luewan S, Jatavan P, Tongprasert F, Sukpan K. A simple rule for prenatal diagnosis of total anomalous pulmonary venous return. J Ultrasound Med. (2016) 35(7):1601–7. doi: 10.7863/ultra.15.08016
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Paladini D, Pistorio A, Wu LH, Meccariello G, Lei T, Tuo G, et al. Prenatal diagnosis of total and partial anomalous pulmonary venous connection: multicenter cohort study and meta-analysis. Ultrasound Obstet Gynecol. (2018) 52(1):24–34. doi: 10.1002/uog.18907
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Valsangiacomo ER, Hornberger LK, Barrea C, Smallhorn JF, Yoo SJ. Partial and total anomalous pulmonary venous connection in the fetus: two-dimensional and Doppler echocardiographic findings. Ultrasound Obstet Gynecol. (2003) 22(3):257–63. doi: 10.1002/uog.214
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Seale AN, Uemura H, Webber SA, Partridge J, Roughton M, Ho SY, et al. Total anomalous pulmonary venous connection: morphology and outcome from an international population-based study. Circulation. (2010) 122(25):2718–26. doi: 10.1161/CIRCULATIONAHA.110.940825
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Seale AN, Carvalho JS, Gardiner HM, Mellander M, Roughton M, Simpson J, et al. Total anomalous pulmonary venous connection: impact of prenatal diagnosis. Ultrasound Obstet Gynecol. (2012) 40(3):310–8. doi: 10.1002/uog.11093
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Mao YK, Zhao BW, Zheng FH, Wang B, Peng XH, Chen R, et al. Z-scores for fetal left atrial size and left atrium-descending aorta distance in fetuses with isolated total anomalous pulmonary venous connection. Prenat Diagn. (2017) 37(10):992–1000. doi: 10.1002/pd.5119
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Han J, Li T, Wu W, Zhang Y, Liu X, Gu X, et al. Post-left atrium space index in fetuses with total anomalous pulmonary venous connection and other congenital heart diseases. J Ultrasound Med. (2020) 39(12):2405–12. doi: 10.1002/jum.15362
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Peng R, Xie HN, Du L, Shi HJ, Zheng J, Zhu YX. Four-dimensional sonography with spatiotemporal image correlation and tomographic ultrasound imaging in the prenatal diagnosis of anomalous pulmonary venous connections. J Ultrasound Med. (2012) 31(10):1651–8. doi: 10.7863/jum.2012.31.10.1651
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Campbell MJ, White BR, Rychik J, Linder J, Faerber JA, Tian Z, et al. Fetal Doppler echocardiographic assessment predicts severe postnatal obstruction in total anomalous pulmonary venous connection. J Am Soc Echocardiogr. (2022) 35(11):1168–75. doi: 10.1016/j.echo.2022.07.007
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Wang X, Yang TY, Zhang YY, Liu XW, Zhang Y, Sun L, et al. Diagnosis of fetal total anomalous pulmonary venous connection based on the post-left atrium space ratio using artificial intelligence. Prenat Diagn. (2022) 42(10):1323–31. doi: 10.1002/pd.6220
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Laudy JA, Huisman TW, de Ridder MA, Wladimiroff JW. Normal fetal pulmonary venous blood flow velocity. Ultrasound Obstet Gynecol. (1995) 6(4):277–81. doi: 10.1046/j.1469-0705.1995.06040277.x
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Carvalho J, Allan L, Chaoui R, Copel J, Devore G, Hecher K, et al. ISUOG practice guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol. (2013) 41(3):348–59. doi: 10.1002/uog.12403
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Salomon LJ, Alfirevic Z, Berghella V, Bilardo C, Hernandez-Andrade E, Johnsen SL, et al. Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. (2011) 37(1):116–26. doi: 10.1002/uog.8831
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Ganesan S, Brook MM, Silverman NH, Moon-Grady AJ. Prenatal findings in total anomalous pulmonary venous return: a diagnostic road map starts with obstetric screening views. J Ultrasound Med. (2014) 33(7):1193–207. doi: 10.7863/ultra.33.7.1193
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Laux D, Fermont L, Bajolle F, Boudjemline Y, Stirnemann J, Bonnet D. Prenatal diagnosis of isolated total anomalous pulmonary venous connection: a series of 10 cases. Ultrasound Obstet Gynecol. (2013) 41(3):291–7. doi: 10.1002/uog.11186
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Bromley B, Estroff JA, Sanders SP, Parad R, Roberts D, Frigoletto FD Jr, et al. Fetal echocardiography: accuracy and limitations in a population at high and low risk for heart defects. Am J Obstet Gynecol. (1992) 166(5):1473–81. doi: 10.1016/0002-9378(92)91622-H
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Shi G, Zhu Z, Chen J, Ou Y, Hong H, Nie Z, et al. Total anomalous pulmonary venous connection: the current management strategies in a pediatric cohort of 768 patients. Circulation. (2017) 135(1):48–58. doi: 10.1161/CIRCULATIONAHA.116.023889
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Liu X, Liufu R, Liu T, Cen J, Yu J, Wen S, et al. Supracardiac total anomalous pulmonary venous connection type Ib: morphology and outcomes. J Thorac Cardiovasc Surg. (2022):S0022-5223(22)01066-2. doi: 10.1016/j.jtcvs.2022.10.008
CrossRef Full Text | Google Scholar
20. Shi G, Zhu F, Wen C, Qiu L, Zhang H, Zhu Z, et al. Single-institution outcomes of surgical repair of infracardiac total anomalous pulmonary venous connection. J Thorac Cardiovasc Surg. (2021) 161(4):1408–17.e2. doi: 10.1016/j.jtcvs.2020.06.023
CrossRef Full Text | Google Scholar
21. Shi G, Zhu F, Wen C, Yan Y, Zhang H, Zhu Z, et al. Cardiac-type total anomalous pulmonary venous return is not benign. J Thorac Cardiovasc Sur. (2022) 165(2):449–59. doi: 10.1016/j.jtcvs.2022.03.036
CrossRef Full Text | Google Scholar
22. Hörer J, Neuray C, Vogt M, Cleuziou J, Kasnar-Samprec J, Jelena L, et al. What to expect after repair of total anomalous pulmonary venous connection: data from 193 patients and 2902 patient years. Eur J Cardiothorac Surg. (2013) 44:800–7. doi: 10.1093/ejcts/ezt129
CrossRef Full Text | Google Scholar
23. Karamlou T, Gurofsky R, Al Sukhni E, Coles JG, Williams WG, Caldarone CA, et al. Factors associated with mortality and reoperation in 377 children with total anomalous pulmonary venous connection. Circulation. (2007) 115(12):1591–8. doi: 10.1161/CIRCULATIONAHA.106.635441
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Husain SA, Maldonado E, Rasch D, Michalek J, Taylor R, Curzon C, et al. Total anomalous pulmonary venous connection: factors associated with mortality and recurrent pulmonary venous obstruction. Ann Thorac Surg. (2012) 94(3):825–31; discussion 31–2. doi: 10.1016/j.athoracsur.2012.04.026
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Moss AJ, Allen HD. Moss and Adams’ heart disease in infants, children, and adolescents: including the fetus and young adult. JAMA Pediatr. (2012) 150(7):774.
26. Seale AN, Webber SA, Uemura H, Partridge J, Roughton M, Ho SY, et al. Pulmonary vein stenosis: the UK, Ireland and Sweden collaborative study. Heart. (2009) 95(23):1944–9. doi: 10.1136/hrt.2008.161356
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Domadia S, Kumar SR, Votava-Smith JK, Pruetz JD. Neonatal outcomes in total anomalous pulmonary venous return: the role of prenatal diagnosis and pulmonary venous obstruction. Pediatr Cardiol. (2018) 39(7):1346–54. doi: 10.1007/s00246-018-1901-0
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Taketazu M, Lougheed J, Yoo SJ, Lim JS, Hornberger LK. Spectrum of cardiovascular disease, accuracy of diagnosis, and outcome in fetal heterotaxy syndrome. Am J Cardiol. (2006) 97(5):720–4. doi: 10.1016/j.amjcard.2005.09.119
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Atik-Ugan S, Saltik IL. Prenatally diagnosed infracardiac total anomalous pulmonary venous connection: from the two sides of the spectrum. J Obstet Gynaecol. (2018) 38(8):1171–3. doi: 10.1080/01443615.2017.1414775
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Acevedo JM, Lee S, Gotteiner N, Lay AS, Patel A. Total anomalous pulmonary venous connection (TAPVC): a familial cluster of 3 siblings. Echocardiography. (2017) 34(10):1531–5. doi: 10.1111/echo.13665
留言 (0)