


記住我








Heart failure (HF) is a complex clinical syndrome characterized by fatigue and dyspnea due to structural or functional deficiencies in the filling or ejection (1–3). HF affects more than 38 million people worldwide, and it is more prevalent in high-income countries among those aged 65 and older (1, 4). In the latest guidelines, patients are classified as having HF with reduced ejection fraction (HFrEF) (ejection fraction < 40%) or HF with preserved EF (HFpEF) (ejection fraction ≥ 50%). Furthermore, patients with a left ventricular ejection fraction of 40%–49% are classified as having HF with a mid-range ejection fraction (HFmrEF) (1). Patients with HF suffer from exercise intolerance, poor quality of life, and high hospitalization rates, as well as an inferior prognosis than most cancers (4–7). In addition to the substantial clinical burden, HF also imposes a global economic burden of $108 billion per year (8). Consequently, given the significant prevalence, inferior prognosis, and substantial economic burden of HF, it is imperative that stakeholders identify effective, sustainable, and acceptable treatments to optimally enhance the health outcomes of patients with HF.
Taking into account the evidence that cardiac rehabilitation (CR) is effective and safe in improving health outcomes and reducing mortality among patients with HF, the guidelines of the American College of Cardiology/American Heart Association, the European Society of Cardiology, and the Canadian Cardiovascular Society have included exercise training, which is the core of CR, in the treatment of HF (1, 3, 9–14). In spite of its effectiveness, cost-effectiveness, as well as be included in the guidelines, exercise-based CR has not been widely adopted (15–17). Nevertheless, we have witnessed tremendous progress over the past decades in the field of exercise training for heart failure, which is a multidisciplinary field that encompasses from epidemiology to management.
Nakagawa et al. distinguished deep synthesis, like systematic review, as well as broad synthesis, like bibliometric analysis, among the synthesis of both evidence and influence (18). Many deep syntheses, which examining a phenomenon across different trials already exist in the field of exercise training for HF (9, 10, 12). However, there is a lack of broad synthesis on the structure and development of this complex and multidisciplinary field.
Bibliometric analysis is a quantitative statistical tool that combines retrieval and statistics, which is used to describe the knowledge structure and trend hot spots in specific research fields, and can provide comparisons according to the distribution of countries, institutions, authors and periodicals (19, 20), to inform future research. Bibliometric analyses have been extensively used in research field such as HF (21–23), exercise (24–26), and CR (27). Yang et al. conducted a bibliometric analysis on the field of sedentary behavior and cardiovascular disease (28). However, there is a lack of bibliometric analysis in the field of exercise training for HF.
Therefore, this present study aims to conduct a bibliometric analysis of global publication in the field of exercise training for HF to identify (i): publication performance of author, institution, country, journal, and categories, and (ii): research status, hot spots, and frontiers in this field.
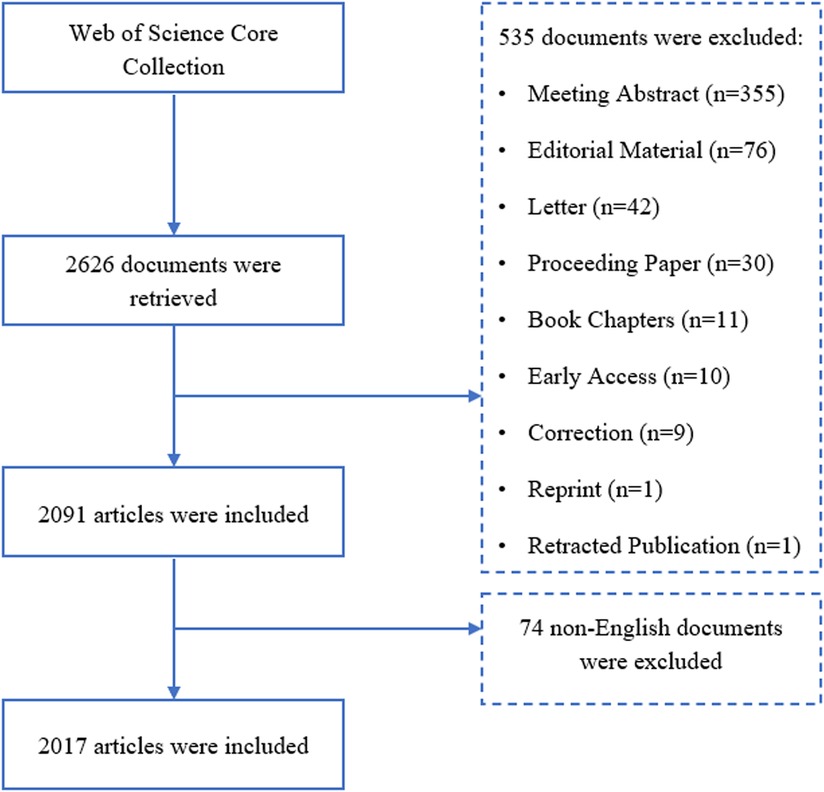
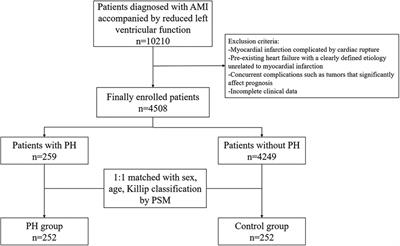
2. Methods 2.1. Data sourcesThis study was conducted according to the bibliometric analysis step-by-step procedure and the best practice guidelines proposed by Donthu et al. (20). There are strong correlations of citation counts across all the disciplines between Web of Science Core Collection (WoSCC), Google Scholar, and Scopus, whereas WoSCC provides earlier documents and more specific, and academic data for bibliometric analysis (29). Meanwhile, other databases of biomedical and life science like PubMed or Scopus, do not provide full text and citation analyses, which are mandatory for bibliometric analysis. Moreover, to eliminate bias caused by the different bibliometric formats of the different databases (30), only the WoSCC was applied for the literature search on the field of exercise training for HF. Following guidelines (20), the search terms in this study were based on a review of the literature of relevant systematic reviews (31, 32), and consultation with experts in the fields of exercise science, public health, physiotherapy, and cardiovascular medicine. The search strategy was as follows: TS = (“exercise training” OR “physical training” OR “exercise therapy”) AND TS = (“heart failure” OR “cardiac failure” OR “ventricular failure” OR “heart decompensation” OR “myocardial failure” OR “heart near failure”). The time span was 2002–2022, and only articles and review articles published in English were included. To eliminate the bias introduced by daily updates of WoSCC, the literature search and data extraction were conducted on 19 December 2022. All data were extracted from WoSCC as plain text files. The procedure of data collection was presented in Figure 1. Initially, the principal investigator conducted a search in the WoSCC database using the search terms described above, hitting 2,626 records. Subsequently, documents that were not articles or review articles were excluded, and 2,091 records were obtained. Finally, after excluding 74 documents that were not published in English, 2017 documents were finally included in the analysis.
Figure 1. Flow chart of data collection.
2.2. Data analysisTwo Java-based bibliometric tools, VOSviewer (1.6.18) and CiteSpace (6.1.R6 Basic), were used to analyze the extracted data. VOSviewer was applied to perform collaborative network analysis of countries/regions, institutions, and authors. CiteSpace was used to conduct keyword co-occurrence analysis, and timeline view of co-cited references. Performance analysis of countries/regions, institutions, authors, journals, categories, and funding agencies was carried out using data automatically generated from the WoSCC.
In CiteSpace, we set the following parameters: Time slicing was from 2002 to 01-01 to 2022-12-19; Year Per Slice was one; Text Processing was Author Keywords; Links were cosine strength within slices; Pruning methods were the pathfinder and the sliced networks; and the Log-Likelihood Ratio was applied as an algorithm for labelling of the clusters generated.
Total link strength and sum of citations were calculated automatically by VOSviewer, and the average number of citations per item (ACI) was derived by dividing the sum of citations by the number of items. The total ‘link strength weighting’ method was applied to demonstrate collaborative networks, in which the size of the node represents the quantity of publications (the larger the diameter the node the more publications). Links represent collaborations between items, with thicker lines representing more collaboration.
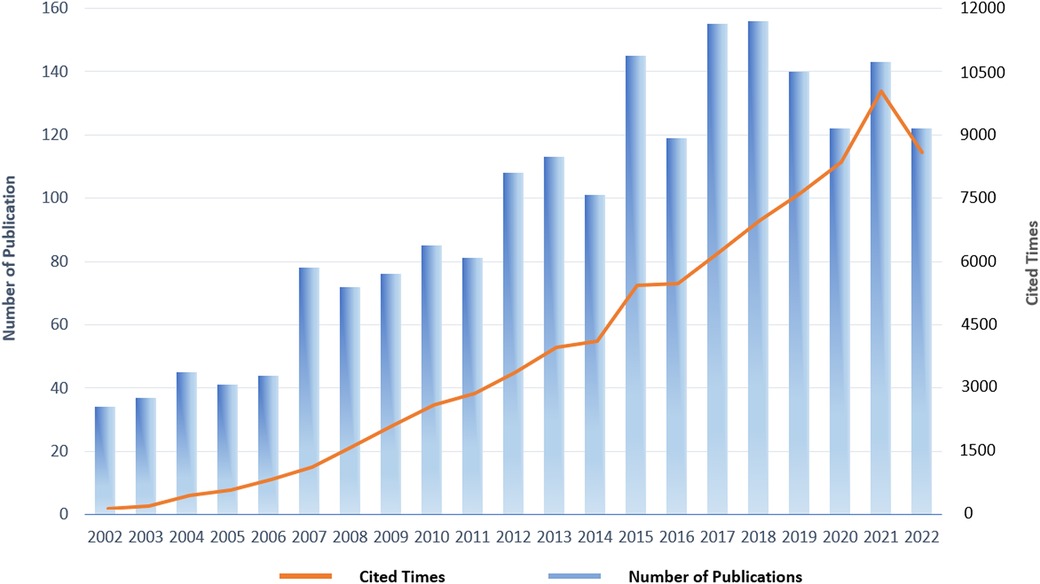
3. Results 3.1. Global publication trendsA total of 2017 publications were included in the final analysis, which included 1,515 articles and 502 review articles. The publications included in this study received a total of 80,854 citations, and each publication received an average of 40.09 citations. The annual distribution of publication and citation trends was shown in Figure 2. From 2002 to 2018, there was an increasing publication trend in the field of exercise training for HF until 2018 when it reached the peak of the annual publication (156 documents). Since then, there has been a slight decline, whereas the number of annual publications has maintained stable at over 120 per year. Collectively, the past two decades of publications in the field of exercise training and HF have demonstrated an upward-steady trend and have received continual interest from researchers.
Figure 2. Annual distribution of publications and citations in the field of exercise training for heart failure.
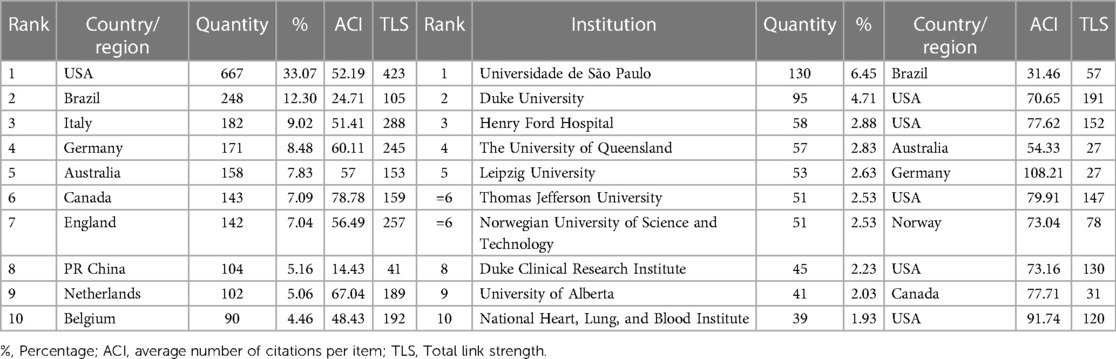
3.2. Analysis of countries/regions and institutionsIn the field of exercise training for HF, a total of 71 countries/regions and 2,269 institutions contributed to at least one publication between 2002 and 2022. As shown in Table 1, USA had the highest number of publications in the field of exercise training for HF (667 documents), accounting for 33.07% of the total, followed by Brazil, Italy, and Germany. Canada had the highest ACI, followed by Netherlands which represented the high quality of research and academic reputation in the field of exercise training for HF in both countries. Universidade de São Paulo in Brazil contributed the largest number of publications (130 documents). Leipzig University had the highest ACI (108.21), representing its high quality of research and academic reputation in the field of exercise training for HF.
Table 1. Top ten active countries/regions and institutions in the field of exercise training for heart failure.
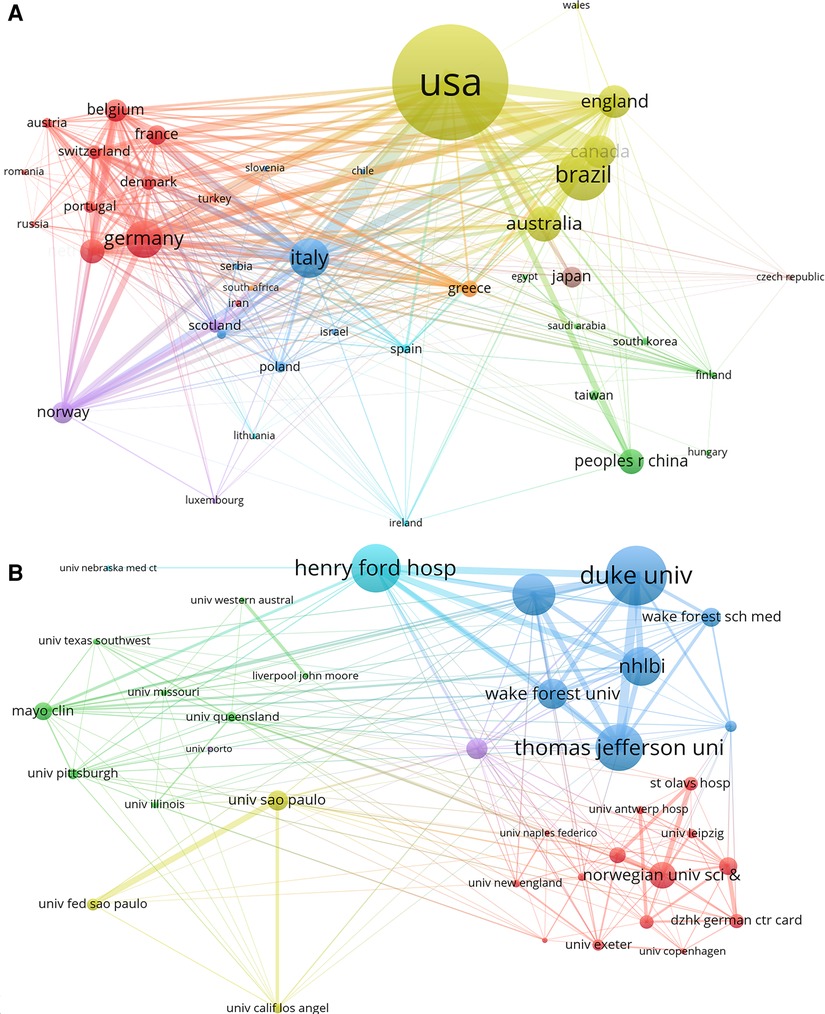
The number of publications by country/region and institution and their collaborative network were presented by visualization network maps. In VOSviewer, the minimum thresholds were set to 5 and 20 publications for countries/regions and institutions respectively, and a total of 42 countries/regions and 38 institutions reached this threshold and were presented in Figures 3A,B. It is clearly that collaboration was relatively strong across countries, with USA had the strongest collaborative network, followed by Italy, England, and Germany. Among institutions, Duke University had the strongest collaborative network, followed by Henry Ford Hospital and Thomas Jefferson University.
Figure 3. The collaborative network between countries/regions and institutions in the field of exercise training for heart failure. (A) Collaborative network map of countries/regions. (B) Collaborative network map of institutions.
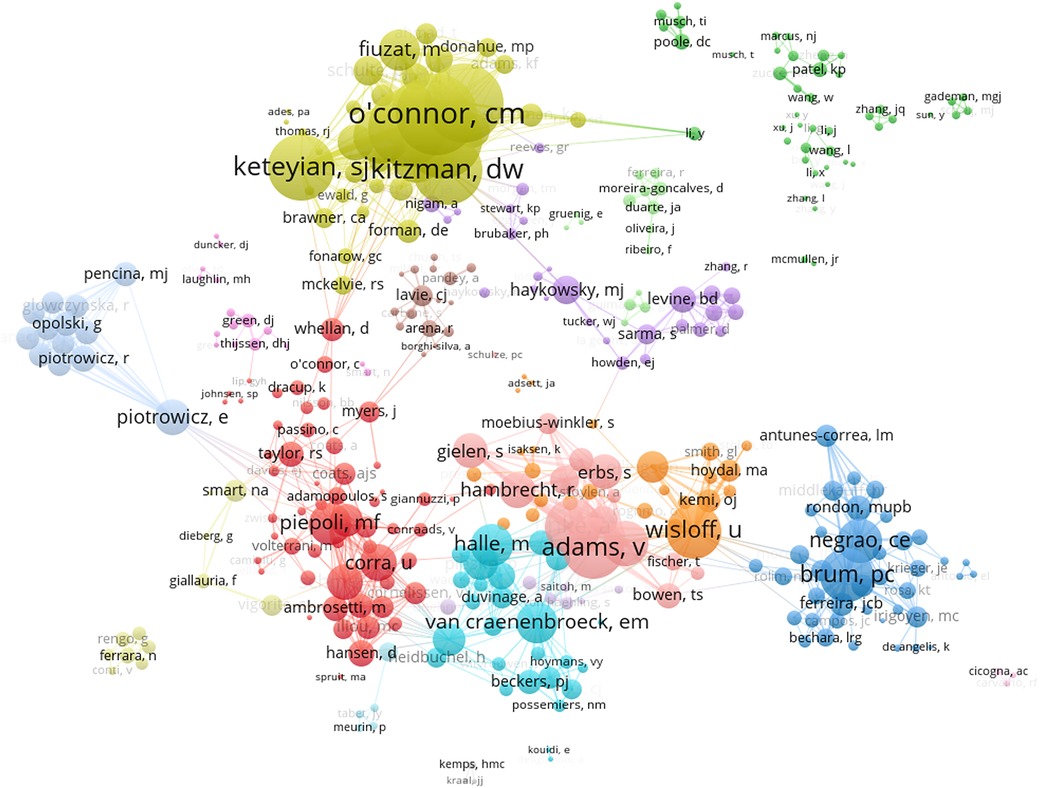
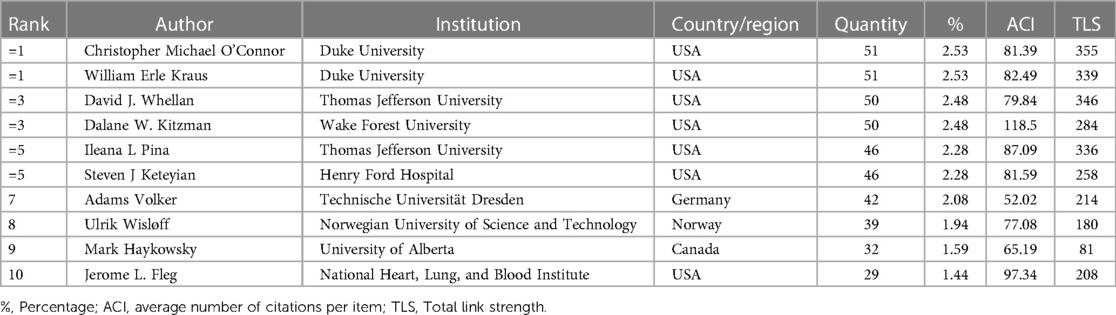
3.3. Analysis of authorsA total of 8,499 authors contributed to the 2017 publications. Table 2 shows the top ten authors with the highest number of publications in the field of exercise training for HF, seven of whom were from the USA and one from Germany, Norway, and Canada respectively. Christopher Michael O’Connor and William Erle Kraus from Duke University published 51 documents, tied as the most prolific researchers in the field of exercise training for HF. Dalane W. Kitzman from Wake Forest University had the highest ACI (118.5), implying that he may have a high quality of research in this field. In the collaborative networks among authors (Figure 4), the minimum thresholds were set to 5 publications, and a total of 403 authors reached this threshold. Christopher Michael O'Connor had the strongest collaborative network, followed by David J. Whellan and William Erle Kraus.
Figure 4. Collaborative network map of authors in the field of exercise training for heart failure.
Table 2. Top ten active authors in the field of exercise training for heart failure.
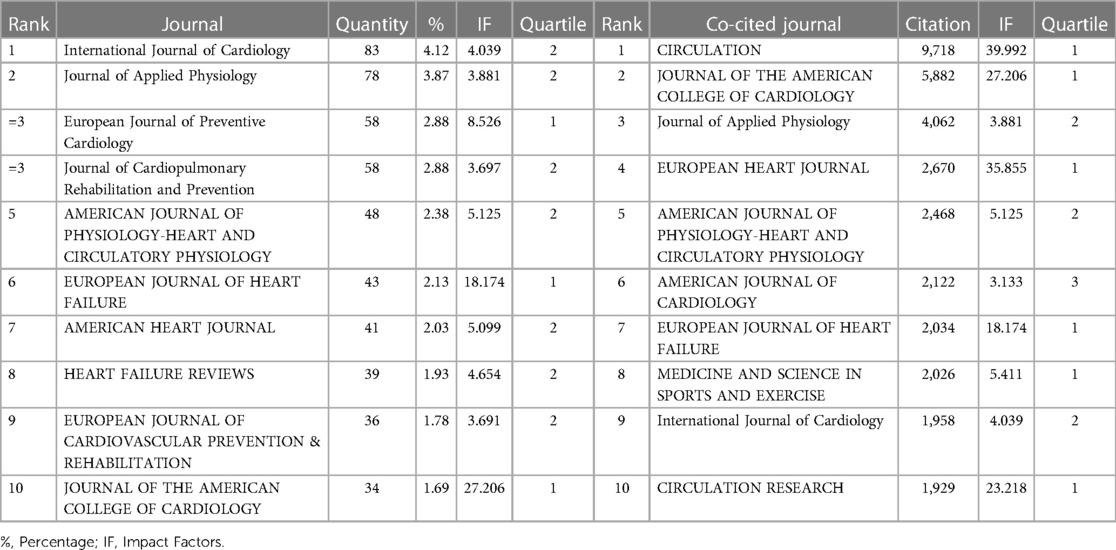
3.4. Analysis of journalsDocuments in the field of exercise training for HF were published in a total of 530 journals, with Table 3 showing the top ten popular journals. Impact factors (IF) and Quartile were reported from the 2021 Journal Citation Report. Three of the top ten popular journals were in quartile 1. The International Journal of Cardiology published the most documents and the JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY had the highest IF (27.206).
Table 3. Top ten active journals and co-cited journals in the field of exercise training for heart failure.
Table 3 shows the top ten popular journals out of a total of 6,149 co-cited journals, four of which were also listed as the top ten journals with the largest number of publications. CIRCULATION was the most cited journal (9,718 documents), followed by JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY (5,882 documents). Of the top ten co-cited journals, six were in Quartile 1, while CIRCULATION had the highest IF (39.992), followed by EUROPEAN HEART JOURNAL (35.855).
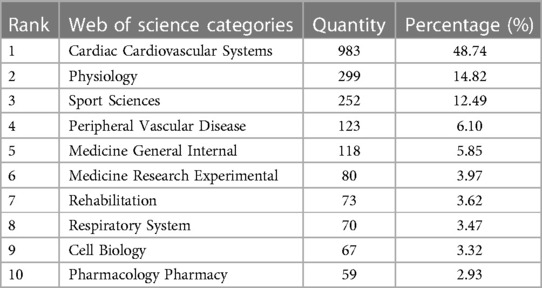
3.5. Analysis of categoriesA total of 77 Web of Science categories were classified for documents in the field of exercise training for HF from 2002–2022. The top ten Web of Science categories in this field is clearly shown in Table 4. Nearly half of the publications were classified as Cardiac Cardiovascular Systems, while Physiology and Sport Science were the second and third most categorized, with over ten percent.
Table 4. Top ten Web of science categories in the field of exercise training for heart failure.
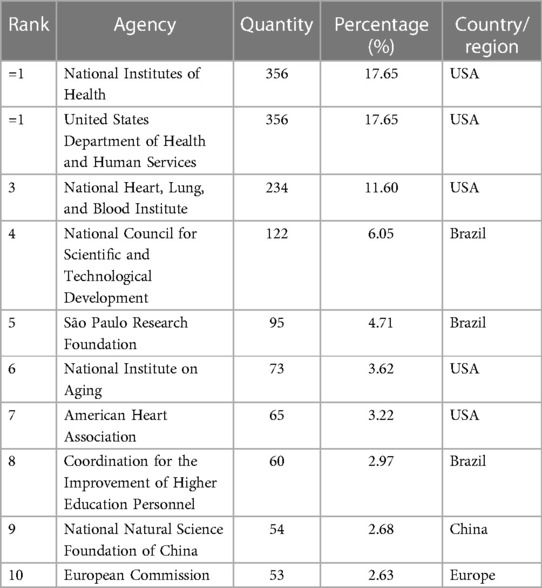
3.6. Analysis of funding agenciesAmong all publications in the field of exercise training for HF from 2002–2022, total of 1,314 research received at least one grant (65.15%). Table 5 presented the top ten funding agencies that provided the largest number of grants, with five from the USA, three from Brazil, and one each from China and Europe. The National Institutes of Health and the United States Department of Health and Human Services from the USA tied for first place, each funded 356 studies.
Table 5. Top ten funding agencies in the field of exercise training for heart failure.
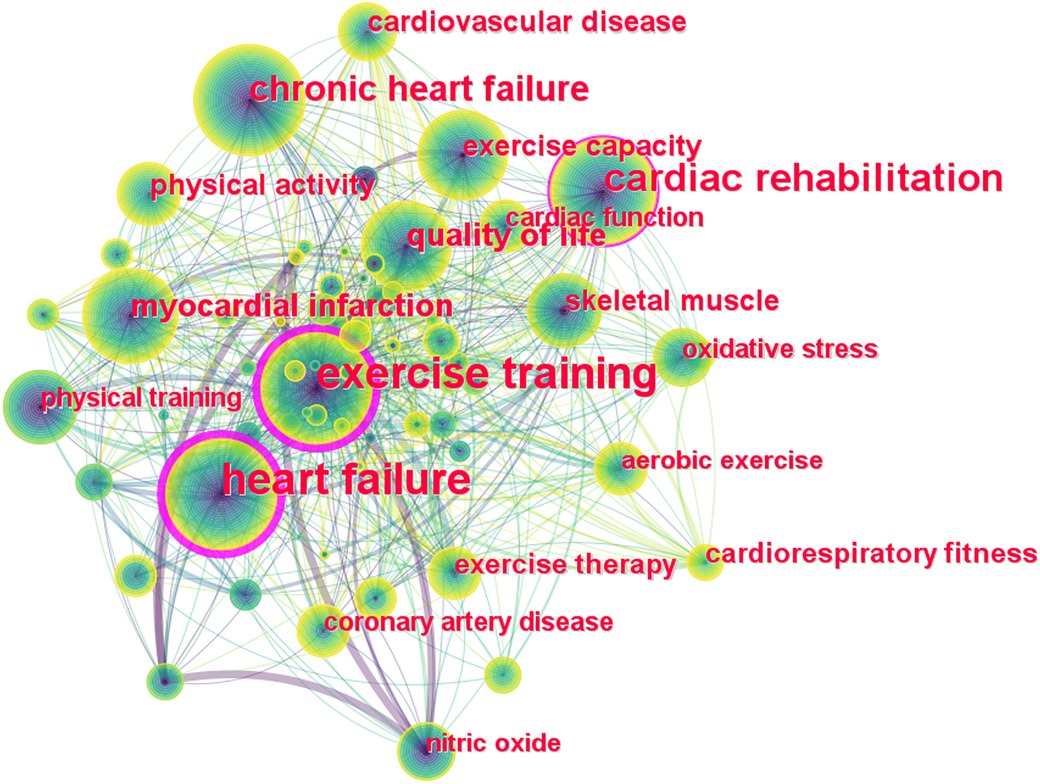
3.7. Analysis of keywordsKeywords are a highly condensed version of the core content and findings in a scientific document, and their number of occurrences and their evolution over time indicate hot spots and directions in a particular field of research. Figure 5 shows the network map of keyword co-occurrence in the field of exercise training for HF, with larger nodes representing more frequent occurrences of the keyword, and thicker links representing more frequent occurrences of both keywords together. The top twenty keywords with the most frequent occurrences are presented in Table 6, which includes types of exercise training, outcome indicators of HF, potential mechanisms: ‘heart failure’ (536), ‘exercise training’ (480), ‘cardiac rehabilitation’ (204), ‘chronic heart failure’ (120), ‘quality of life’ (87), “myocardial infarction” (77) etc.
Figure 5. Network map of keyword co-occurrence in the field of exercise training for heart failure.
Table 6. Top twenty high-frequency keyword in the field of exercise training for heart failure.
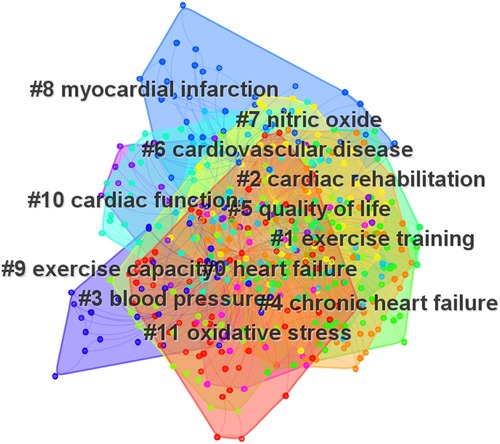
Keyword clustering contributes to the exploration and analysis of current hot spots and knowledge structures. Figure 6 presents the eleven clusters obtained, excluding #1, #2, #4, #6, #8, which are consistent with the research themes. The remaining clusters were divided into two groups as follows: (i): clusters which related to the outcome measures, including #3 blood pressure, #5 quality of life, #9 exercise capacity, and #10 cardiac function; (ii): clusters which related to the potential mechanism, including #7 nitric oxide and #11 oxidative stress.
Figure 6. Network map of keyword clusters in the field of exercise training for heart failure.
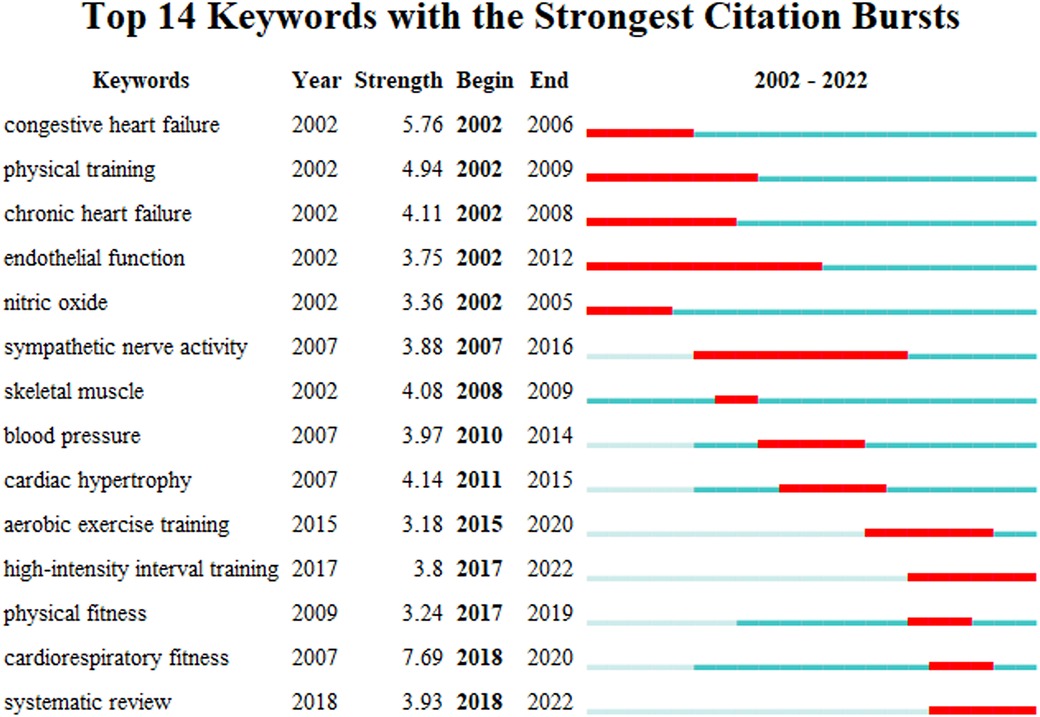
Keyword citation bursts reflect the trends and frontiers of a research field and contribute to predicting and guiding future research directions. Figure 7 shows the top fourteen keywords with the strongest citation bursts in the field of exercise training for HF, where the red line indicates the duration of a keyword citation burst during 2002–2022 (blue line). The keyword ‘high-intensity interval training’ is continually bursting from 2017 to the present, while the keyword ’systematic review’ is continually bursting from 2018 to the present. This indicates that research on high-intensity interval training (HIIT) and evidence synthesis has continued to receive attention in recent years and may be a trend for future research in the field of exercise training for HF.
Figure 7. Top fourteen keywords with the strongest citation bursts in the field of exercise training for heart failure.
3.8. Analysis of co-cited referenceA co-cited reference is a document that was cited by both documents, and the analysis of co-cited references contribute to guiding further research hot spots in the field of research. The top ten most co-cited references are presented in Table 7. The document entitled ‘Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomised controlled trial’ by O’Connor et al. published in JAMA in 2009 was co-cited the most times. This document reported the results of a multicenter, randomized controlled trial designed to investigate the effectiveness and safety of exercise training in patients with chronic HF (33). The second most co-cited document was published in 2016 in the European Heart Journal by Ponikowski et al. entitled: ‘2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC’ (34). This guideline for the diagnosis and treatment of acute and chronic HF recommended regular aerobic exercise to improve functional capacity and symptoms in patients with HF and to reduce the risk of HF hospitalization in stable patients with HFrEF. The document entitled: ’Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study’, published by Wisløff et al. in 2007 in CIRCULATION, received the third largest number of co-citations. This randomized controlled trial compared the cardiovascular effects of aerobic interval training with moderate continuous training in patients with HF (35).
Table 7. Top ten most co-cited references in the field of exercise training for heart failure.
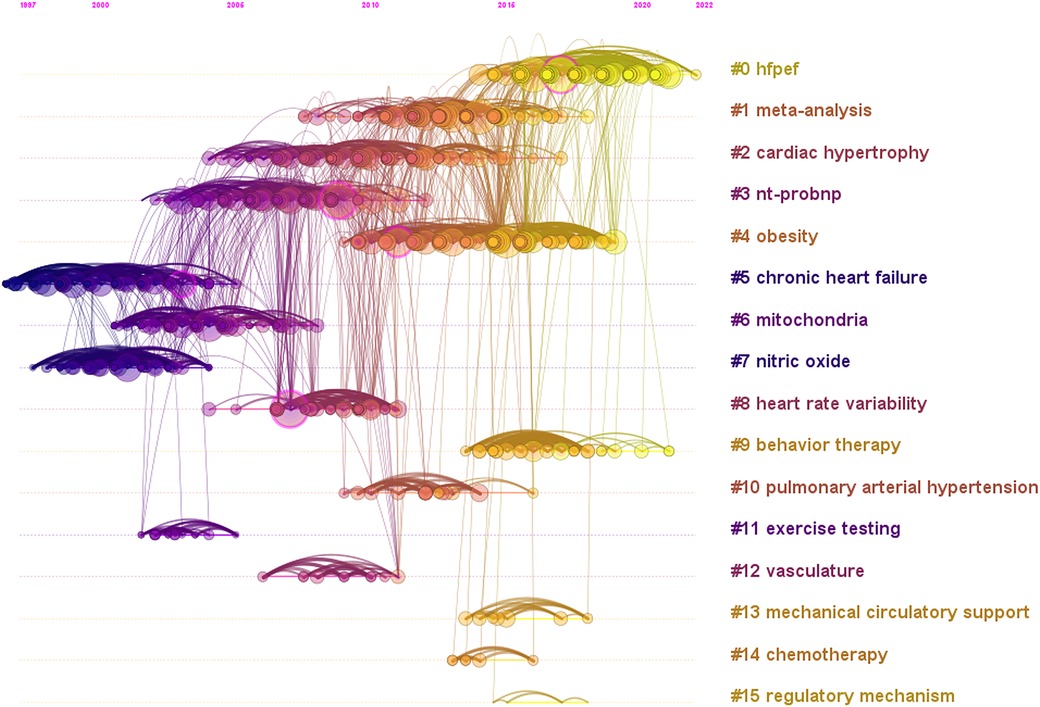
A timeline view of co-cited references in the field of exercise training for HF is presented in Figure 8, indicating a change in research topics over time. Earlier research in this field focused on chronic HF, mitochondria, and nitric oxide. More recently, researchers have focused on HFpEF and behavior therapy, which may be the latest research hot spot and future trend.
Figure 8. Timeline view of co-cited reference in the field of exercise training for heart failure.
4. Discussion 4.1. General informationResearch progress in the field of exercise training for HF can be estimated based on the quantity and trend of annual publications and citations. In general, the number of publications in this field has gradually increased in the past two decades. From 2002–2014, relatively few documents were published, thus relevant research was still in its infancy. Since 2014, publications in this field have entered a period of rapid growth, indicating that research on exercise training for HF has received increasing attention in recent years. The USA contributed the largest quantity of publications and had the strongest collaborative network. In contrast to other active developed countries in this field, such as Italy and Germany, developing countries had a larger number of publications, while the quality of research and cooperation needs to be further enhanced. Among the institutions, while Universidade de São Paulo from Brazil published the largest number of documents, those from the USA, Canada and Germany had higher quality of research. In terms of institutional collaboration, only the USA institutions had strong collaborative networks. Overall, apart from the USA, cooperation between countries and institutions were weak, thus strengthening international and institutional cooperation, especially in developing countries, is a priority in this field. The scientists with the largest number of publications, led by Christopher M O’Connor, William E Kraus, David J Whellan, and Dalane W Kitzman, are the backbone of scientific productivity in the field of exercise training for HF and are all from the USA. Through analysis of journals, this study found that the top ten most productive journals in the field of exercise training for HF are all quartile 1 or quartile 2 journals. Therefore, it is achievable to publish research on the topic of exercise training for HF on high quality journals.
4.2. Hot spots and frontiersBased on the citation burst of co-occurring keywords and the timeline view of co-cited reference, we identified the following hot spots and frontiers in the field of exercise training for HF. HIIT is the promising and cutting-edge exercise training treatment in this field. HIIT is defined as repeated high-intensity interval bouts between 80% and 100% of peak heart rate interspersed with recovery periods or light exercise (36, 37). It is initially designed to improve the aerobic capacity of runners, was first adopted as a treatment for patients with coronary artery disease and chronic HF in 1990 (38, 39). This emerging exercise training method can further enhance the metabolic, cardiopulmonary, and systemic vascular adaptations of patients with HF (36), and has been demonstrated to be safe for patients with cardiac pathology (40). This type of exercise training is often used to compare with traditional moderate intensity training. Recent meta-analyses proposed that HIIT is significantly more effective than moderate intensity training for improving peak VO2 value and left-ventricular ejection fraction among patients with HF, which are independent predictor of cardiovascular mortality in patients with cardiovascular diseases (41, 42). Furthermore, a previous meta-analysis recommended that patients with HF conduct HIIT at least three days a week, while the active recovery intervals should be between 40% and 60% of the peak VO2 (43).
HFpEF is a active type of HF in the field of exercise training for HF. This type of HF is a condition with similar clinical manifestations and event rate to HFrEF (44, 45), but different in etiology, cardiac remodeling, pathophysiology, comorbid disorders, and response to therapy (44). CR for patients with HFpEF has recently received increasing attention. A recent systematic review with meta-analysis examined reported that exercise training significantly improved cardiorespiratory fitness, with no difference in peak VO2 between resistance and aerobic exercise, while HIIT significantly improved peak VO2 compared to aerobic exercise (46). Another meta-analysis including the largest sample size to date in this field proposed that exercise training in patients with HFpEF improved their exercise tolerance and somatic-related quality of life, but not emotional or mental quality of life or echocardiographic parameters (47). It is noted that the majority of clinical trials included in recent systematic reviews on exercise training and HFpEF were small sample-sized randomized controlled trials rather than large multicenter trials, which may have reduced the strength of evidence for the findings. Therefore, more robustly designed, multicenter large randomized clinical trials are needed in the future to further examine the effects of different types of exercise training on relevant indicators in patients with HFpEF.
Systematic review is a hotly mentioned study design in the field of exercise training for HF and is at the heart of evidence-based medicine (48). The American Heart Association considered the evidence from systematic reviews and meta-analyses to be ‘A’ level, assuring the highest confidence. However, Murad et al. suggest using this as a lens to observe other types of studies, that is, evaluations and applications, given the different risks of bias in different systematic reviews (49). Furthermore, systematic review with meta-analysis is tools for stakeholders to access and apply evidence (49). Researchers can identify research gaps and future research orientations based on the evidence derived from systematic reviews. Policy makers can use the Grading of Recommendations Assessment, Development and Evaluation to determine the strength of evidence from systematic reviews and to develop relevant policies and guidelines (50). Clinical practitioners can be guided in their clinical practice by evidence-based guidelines that include evidence from systematic reviews. In the field of HF management, national and international evidence-based guidelines have incorporated exercise training into treatment and management (3, 34, 51). However, implementation is limited by the need to safely select patients and develop exercise prescriptions through cardiopulmonary exercise testing and the lack of coverage by the Centers for Medicare and Medicaid Service for patients with HFpEF (52, 53).
4.3. LimitationThis research is the first bibliometric analysis of exercise training for HF, but there are some inevitable limitations. First, this study only included literature published in English, and there may have been some omissions for studies published in other languages. However, given the impact of English-language publications, the impact of this exclude criteria was limited. Second, this study only searched one electronic database, WOSCC, and may have omitted publication in other databases and grey literature. This is because different databases have different rules for abbreviating author names, etc., and integrating data from different databases may result in a significant amount of duplication. Furthermore, only articles and review articles were included in the analysis, while WoSCC has more accurate document type labelling than alternative database such as Scopus (54).
5. ConclusionThis study applied state-of-the-art bibliometric and scientific mapping methods to provide researchers and other stakeholders with a panoramic view of the field of exercise training for HF from 2002–2022. Publications in the field show an upward-stable trend, with developed countries, led by the USA, maintaining a high number and quality of publications at the same time. Brazil and China represent the developing countries in this field, but there is a need to improve the quality of research as well as the international cooperation. In the field of exercise training for HF, the hot and cutting-edge type of exercise training is HIIT, while HFpEF is the type of heart failure that has received attention, and systematic review is the promising study design.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributionsZY, ZZ, and MQ designed the study; ZY, CZ, and MQ collected and analysed the data; ZY, MY, JW, and JW interpreted the data; ZY and ZZ drafted the manuscript; ZY, ZZ, ZW, and MQ revised the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC). developed with the special contribution of the heart failure association (HFA) of the ESC. Eur J Heart Fail. (2016) 18(8):891–975. doi: 10.1093/eurheartj/ehw128
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll Cardiol. (2013) 62(16):e147–239. doi: 10.1016/j.jacc.2013.05.019
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Calvert MJ, Freemantle N, Cleland JGF. The impact of chronic heart failure on health-related quality of life data acquired in the baseline phase of the CARE-HF study. Eur J Heart Fail. (2005) 7(2):243–51. doi: 10.1016/j.ejheart.2005.01.012
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. J Nat Rev Cardiol. (2017) 14(10):591–602. doi: 10.1038/nrcardio.2017.65
CrossRef Full Text | Google Scholar
9. Smart N, Marwick THJ. Exercise training for patients with heart failure: a systematic review of factors that improve mortality and morbidity. Am J Med. (2004) 116(10):693–706. doi: 10.1016/j.amjmed.2003.11.033
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Taylor RS, Long L, Mordi IR, Madsen MT, Davies EJ, Dalal H, et al. Exercise-based rehabilitation for heart failure: cochrane systematic review, meta-analysis, and trial sequential analysis. JACC Heart Fail. (2019) 7(8):691–705. doi: 10.1016/j.jchf.2019.04.023
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Long L, Mordi IR, Bridges C, Sagar VA, Davies EJ, Coats AJ, et al. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev. (2019) 1(1):CD003331. doi: 10.1002/14651858.CD003331.pub5
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Bjarnason-Wehrens B, Nebel R, Jensen K, Hackbusch M, Grilli M, Gielen S, Schwaab B, Rauch B, Prevention GSoC, cardiology RJEjop. Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: the cardiac rehabilitation outcome study in heart failure (CROS-HF): a systematic review and meta-analysis. Eur J Prev Cardiol. (2020) 27(9):929–52. doi: 10.1177/2047487319854140
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Ezekowitz JA, O’Meara E, McDonald MA, Abrams H, Chan M, Ducharme A, Giannetti N, Grzeslo A, Hamilton PG, Heckman GA, et al. 2017 Comprehensive update of the Canadian cardiovascular society guidelines for the management of heart failure. Can J Cardiol. (2017) 33(11):1342–433. doi: 10.1016/j.cjca.2017.08.022
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Piepoli MF, Binno S, Corrà U, Seferovic P, Conraads V, Jaarsma T, Schmid JP, Filippatos G, Ponikowski PP, Physiology CoE et al. ExtraHF survey: the first European survey on implementation of exercise training in heart failure patients. Eur J Heart Fail. (2015) 17(6):631–8. doi: 10.1002/ejhf.271
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Bozkurt B, Fonarow GC, Goldberg LR, Guglin M, Josephson RA, Forman DE, et al. Cardiac rehabilitation for patients with heart failure: JACC expert panel. J Am Coll Cardiol. (2021) 77(11):1454–69. doi: 10.1016/j.jacc.2021.01.030
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Grace SL, Gravely-Witte S, Brual J, Monette G, Suskin N, Higginson L, et al. Contribution of patient and physician factors to cardiac rehabilitation enrollment: a prospective multilevel study. Eur J Cardiovasc Prev Rehabil. (2008) 15(5):548–56. doi: 10.1097/HJR.0b013e328305df05
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Golwala H, Pandey A, Ju C, Butler J, Yancy C, Bhatt DL, Hernandez AF, Fonarow GC: Temporal trends and factors associated with cardiac rehabilitation referral among patients hospitalized with heart failure: findings from get with the guidelines–heart failure registry. J Am Coll Cardiol. (2015), 66(8):917–26. doi: 10.1016/j.jacc.2015.06.1089
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Nakagawa S, Samarasinghe G, Haddaway NR, Westgate MJ, O’Dea RE, Noble DWA, et al. Research weaving: visualizing the future of research synthesis. Trends Ecol Evol. (2019) 34(3):224–38. doi: 10.1016/j.tree.2018.11.007
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. (2021) 133:285–96. doi: 10.1016/j.jbusres.2021.04.070
CrossRef Full Text | Google Scholar
21. Zhang X, Zhou Y, Wei N, Shou X, Fan S, You Y, et al. A bibliometric analysis of heart failure with preserved ejection fraction from 2000 to 2021. Curr Probl Cardiol. (2022) 47(9):101243. doi: 10.1016/j.cpcardiol.2022.101243
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Wang H, Shi J, Shi S, Bo R, Zhang X, Hu Y. Bibliometric analysis on the progress of chronic heart failure. Curr Probl Cardiol (2022) 47(9):101213. doi: 10.1016/j.cpcardiol.2022.101213
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Edlinger C, Mösenlechner T, Krizanic F, Wernly B, Kretzschmar D, Hoppe UC, et al. Emerging trends in cardiovascular research: hFpEF in the spotlight. A bibliometric analysis of the years 2009–2016. Minerva Med. (2020) 112(4):506–13 doi: 10.23736/S0026-4806.20.06447-2
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Khatra O, Shadgan A, Taunton J, Pakravan A, Shadgan B. A bibliometric analysis of the top cited articles in sports and exercise medicine. Orthop J Sports Med. (2021) 9(1):2325967120969902. doi: 10.1177/2325967120969902
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Zhang F, Ye J, Bai Y, Wang H, Wang W. Exercise-Based renal rehabilitation: a bibliometric analysis from 1969 to 2021. Front Med (Lausanne). (2022) 711(9):842919. doi: 10.3389/fmed.2022.842919
CrossRef Full Text | Google Scholar
26. Dong Y, Weng L, Hu Y, Mao Y, Zhang Y, Lu Z, et al. Exercise for stroke rehabilitation: a bibliometric analysis of global research from 2001 to 2021. Front Aging Neurosci. (2022) 14:876954. doi: 10.3389/fnagi.2022.876954
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Yuan G, Shi J, Jia Q, Shi S, Zhu X, Zhou Y, Shi S, Hu Y. Cardiac rehabilitation: a bibliometric review from 2001 to 2020. Front Cardiovasc Med. (2021) 8:672913. doi: 10.3389/fcvm.2021.672913
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Yang Z, Chen S, Bao R, Li R, Bao K, Feng R, et al. Public health concern on sedentary behavior and cardiovascular disease: a bibliometric analysis of literature from 1990 to 2022. Medicina (Kaunas). (2022) 58(12):1764. doi: 10.3390/medicina58121764
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Martín-Martín A, Orduna-Malea E, Thelwall M, Delgado López-Cózar E. Google scholar, web of science, and scopus: a systematic comparison of citations in 252 subject categories. J Informetr. (2018) 12(4):1160–77. doi: 10.1016/j.joi.2018.09.002
CrossRef Full Text | Google Scholar
31. Sagar VA, Davies EJ, Briscoe S, Coats AJ, Dalal HM, Lough F, et al. Exercise-based rehabilitation for heart failure: systematic review and meta-analysis. Open Heart. (2015) 2(1):e000163. doi: 10.1136/openhrt-2014-000163
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Lloyd-Williams F, Mair FS, Leitner M. Exercise training and heart failure: a systematic review of current evidence. Br J Gen Pract. (2002) 52(474):47–55.11791816
PubMed Abstract | Google Scholar
33. O’Connor CM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ, Leifer ES, Kraus WE, Kitzman DW, Blumenthal JA, et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. Jama (2009), 301(14):1439–50. doi: 10.1001/jama.2009.454
CrossRef Full Text | Google Scholar
34. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC)Developed with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. (2016) 37(27):2129–200. doi: 10.1093/eurheartj/ehw128
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Wisløff U, Støylen A, Loennechen JP, Bruvold M, Rognmo Ø, Haram PM, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation. (2007) 115(24):3086–94. doi: 10.1161/CIRCULATIONAHA.106.675041
CrossRef Full Text | Google Scholar
36. Weston KS, Wisløff U, Coombes JS. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. Br J Sports Med. (2014) 48(16):1227–34. doi: 10.1136/bjsports-2013-092576
留言 (0)