
記住我







The aim of this study was to develop a model of septic shock in pig that can provide a realistic and clinically relevant starting point for further investigations. To provide a feasible basis for further research, the model must be implementable within a realistic time. In our specific case, this means that septic shock, defined by clinical criteria, should occur within a few hours to provide a meaningful starting point for further therapies. Using the keywords "sepsis AND septic shock AND pig", a systematic literature search was performed in the PubMed® database. 305 entries from the years 2002–2022 were evaluated. The obtained publications were examined for the applicability of the criteria of septic shock in humans (i.e., mean arterial pressure of less than 65 mmHg and elevated levels of serum lactate of more than 2 mmol/L [34]) together with the type and mode of sepsis induction and the age/weight as well as the sex of the used animals was analysed. Considering the above mentioned quality criteria for a model of septic shock in pigs, a cutoff for the occurrence of shock defined as a serum lactate level > 2 mmol/L and a mean arterial pressure < 65 mmHg within 8 h after sepsis induction was chosen. The corresponding pig models were limited to in vivo models of polymicrobial sepsis with septic shock. Publications that used a two-hit model (e.g., hemorrhage/ischemia and sepsis) or neonatal pigs were excluded. Publications (n = 7) without data about MAP and/or lactate levels were also excluded from Table 1. References of Table 1 are listed in Additional file 1: Table S1.
Table 1 Systematic literature review of porcine septic shock models used from the years 2002–2022 and their characteristicsAnimals and animal preparationThe present study was approved by the Animal Care Committee of the State Government of North-Rhine Westphalia (LANUV NRW, Recklinghausen, Germany; Approval AZ 81-02.04.2020.A428). All methods were performed in accordance with the National Institutes of Health Guide and as well as the American Physiologic Society’s “Guide for the Care and Use of Laboratory Animals”.
After an adaptation period of 1 week and a withdrawal of food for 12 h with water ad libitum, 10 healthy female German landrace pigs with a body weight of 29.5 ± 4.4 kg were anaesthetized by intramuscular injection of S-ketamine (15 mg/kg, Pfizer Inc, New York, USA) and azaperone (2 mg/kg, Elanco Animal Health Inc, Bad Homburg, Germany). Subsequently, venous access (20G) was established into an ear vein. After deepening anaesthesia with intravenous administration of propofol (2–3 mg/kg, CP-Pharma Handelsgesellschaft mbH, Burgdorf, Germany), the pigs were endotracheally intubated with an ID 7.5 tube (Teleflex Medical Europe Ltd, Athlone, Ireland) to provide mechanical ventilation (Cato®, Dräger Medical Deutschland GmbH, Lübeck, Germany) with a tidal volume of 7–10 mL/kg adjusted to an expiratory carbon dioxide partial pressure of 40 ± 5 mmHg and an inspiratory oxygen fraction of 30 ± 5%. Anaesthesia was continued with isoflurane (1.2–1.4Vol% et, Isofluran vet., Baxter Deutschland GmbH, Unterschleißheim, Germany) and continuous analgesia was provided by intravenous fentanyl (0.005 mg/kg/h, Janssen-Cilag GmbH, Neuss, Germany). Anaesthesia was maintained until the end of the study. All subsequent catheterizations and surgical procedures were performed under sterile conditions and after ensuring adequate general anaesthesia. After ultrasound-guided placement of a quad-lumen central venous catheter (Teleflex Medical Europe Ltd, Athlone, Ireland) in the jugular vein using Seldinger’s technique and a 13F high-flow catheter (HF-TLK, Achim Schulz-Lauterbach VMP GmbH, Iserlohn, Germany) in the femoral vein, a pulse contour cardiac output catheter was placed in the left femoral artery (PULSION Medical Systems AG, Munich, Germany). The intravascular catheters were sewn on and connected to a transpulmonary thermodilution and pulse contour cardiac output computer (PiCCO2, PULSION Medical Systems AG, Munich, Germany) for continuous analysis of hemodynamic parameters.
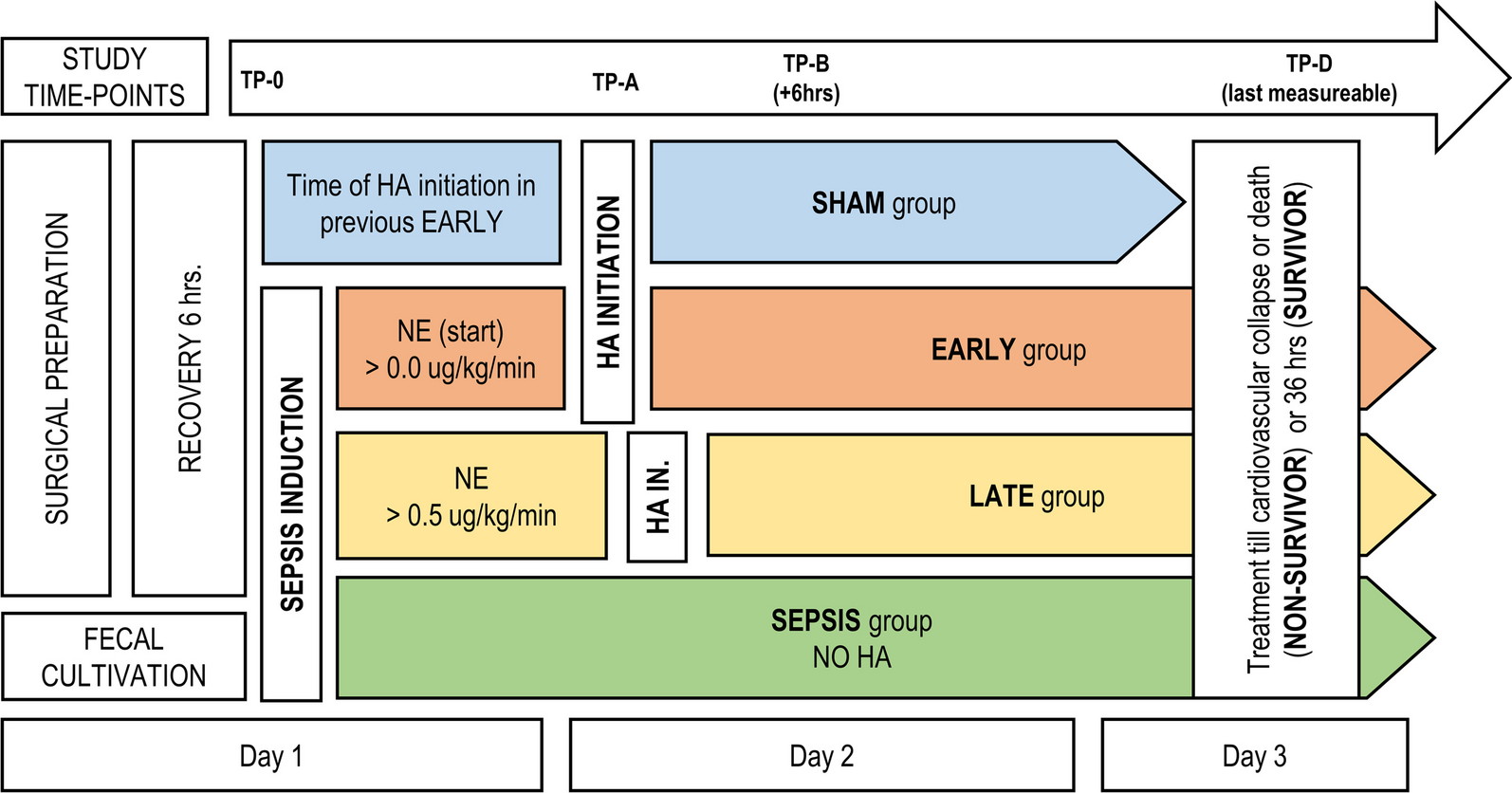
Experimental protocolAfter placement of intravascular catheters, a median laparotomy was performed. An electrocautery (ERBE VIO 300 D, ERBE Elektromedizin GmbH, Tübingen, Germany) was used immediately after skin incision to stop minimal bleeding from dermal and muscular vessels. An abdominal drain (Ch25) was placed between the small intestinal loops to exclude encapsulation or merely localized peritonitis following faeces application and a 12Fr balloon catheter (Teleflex Medical Europe Ltd, Athlone, Ireland) was surgically inserted into the urinary bladder to measure urine output. After placement of the drainages, the abdominal cavity was surgically closed. During surgery, the animals received a fluid bolus of crystalloid fluid (Sterofundin ISO, B. Braun SE, Melsungen, Germany, 10 mL/kg) in addition to the basic fluid requirement, which was met by a continuous infusion of 2 mL/kg/h during the experiment. After instrumentation and surgery, the pigs were allowed to recover until hemodynamic and laboratory parameters normalized for at least 1 h. At this timepoint baseline measurements were performed and sepsis was induced by injecting 3 g/kg bodyweight (BW) of faeces, collected the day before and incubated overnight (for at least 19 h) at 37 °C in 200 mL 1% glucose solution, through the drainage without prior filtration into the abdominal cavity. The occurrence of septic shock was defined as MAP < 60 mmHg in combination with serum lactate ≥ 2 mmol/L at a timepoint at least 4 h apart from faeces injection. During the establishment phase of the model, preliminary experiments showed that 1.5 g/kg faeces did not sufficiently induce septic shock. If criteria for septic shock were met a second set of measurements was taken. Afterwards treatment was initiated according to the 1-h-bundle of the surviving sepsis campaign including an i.v. fluid bolus (Sterofundin ISO, B. Braun SE, Melsungen, Germany) of 30 mL/kg over 1 h. In addition, broad spectrum antibiotic therapy (meropenem (Fresenius Kabi Deutschland GmbH, Bad Homburg, Germany) bolus 20 mg/kg, followed by continuous infusion (2 mg/kg/h) and vancomycin (Hikma Pharmaceuticals PLC, London, United Kindom) bolus 20 mg/kg over 1 h followed by continuous infusion (0.5 mg/kg/h)) was administered for the rest of the experiment. Norepinephrine (Sanofi-Aventis Deutschland GmbH, Frankfurt, Germany) was administered continuously and titrated to maintain a MAP > 65 mmHg. The treatment protocol was continued for 8 h after the onset of septic shock. After completion of the initial fluid bolus the pigs received additional fluid boluses of 5 mL/kg over 15 min if stroke volume variation (SVV) exceeded 12% (Fig. 1). If hypoglycaemia occured (serum glucose < 70 mg/dL), glucose was substituted using 40% glucose solution (Glucose40%, B. Braun SE, Melsungen, Germany).
Fig. 1
Timeline of the experimental protocol. After surgery and recovery time until hemodynamic and laboratory parameters were in a physiological range, baseline measurements were performed. Septic shock (defined according to the Sepsis-3 criteria) was induced by intraperitoneal injection of 3 g/kg BW feces. At the onset of septic shock (mean 4.8 ± 0.29 h post sepsis induction), a therapy phase over 8 h was succeeded according to the sepsis guideline with application of the 1 h-bundle, followed by a differentiated hemodynamic as well as volume therapy
Measurements and blood samplingHemodynamic parameters were observed continuously and extended hemodynamic parameters were measured hourly by thermodilution. The body surface area was calculated according to Kelley et al. (1973) [17]. Urine output and ventilatory parameters were also documented hourly. Blood sampling was performed hourly by bedside arterial and central venous blood gas analysis, including sodium, potassium, calcium, glucose, lactate and creatinine (epoc® Blood Analysis Systems with epoc® BGEM3 test cards, Siemens Healthcare GmbH, Erlangen, Germany). For immunoassay analysis, EDTA-stabilized blood was drawn preoperatively and at shock time, centrifuged, and the collected plasma fraction was frozen at − 80 °C until analysis. SVV and fluid bolus administration were documented every 15 min during the treatment phase.
Proinflammatory mediators and glycocalyx markerFor the determination of proinflammatory mediators and their changes during the development of septic shock, enzyme-linked immunosorbent assay (ELISA) (Cytokine and Chemokine 9-Plex Porcine ProcartaPlex™ Panel 1, ThermoFisher Scientific Inc., Waltham, Massachusetts, USA) was used following the instructor’s guide for n = 6 pigs preoperatively and at time of shock. To analyze glycocalyx damage, syndecan-1 ELISA (Pig Syndecan 1 (SDC1) ELISA Kit, Abbexa LTD, Cambridge, UK) was performed for n = 10 animals at the beginning of the experiment and at the end of the experiment, 8 h after the onset of septic shock (S + 8) according to the manufacturer's instructions.
After the end of the protocol pigs were euthanized with 200 mL potassium chloride (KCL) 7.46% (Deltamedica GmbH, Reutlingen, Germany) under deep anaesthesia and tissue samples were collected.
Microbiological and histopathological analysisTo differentiate the bacterial inoculum, faeces samples (n = 6) were analysed microbiologically and evaluated in terms of bacterial species and bacterial counts (colony forming units (CFU)). Bacteria were grown on blood agar (total CFU) (BD Columbia 5% SB/COL-S, BD, Heidelberg, Germany), MacConkey (BD Mac Conkey II, BD, Heidelberg, Germany) and CNA agar (BD CNA Improved II, BD, Heidelberg, Germany) for 24 h at 37 °C, and bacterial species were analysed by Matrix Assisted Laser Desorption Ionization Time of Flight (MALDI Biotyper Sirius One, Bruker Corporation, USA).
The porcine kidney biopsies from the medulla of n = 10 septic pigs and n = 5 healthy controls, kept in 4% formaldehyde at room temperature, were embedded using Microm STP 120 Spin Tissue Processor (Thermo Fisher Scientific, Germany) following coating with paraffin (Thermo Fisher Scientific, Germany) at 60 °C. Next, 6 μm thick slices were made using Microm HM 355 S (Thermo Fisher Scientific, USA), then transferred to a microscope slide (Thermo Scientific, Germany) and put on a slide warmer (Adamas Instrumenten, Netherlands) at 37 °C to dry. After incubation at 37 °C over night, the histology cross sections were stained in hematoxylin–eosin (HE) (Merck, Germany). Representative pictures were taken with a LionHeart FX Automated Microscope (BioTek Instruments, USA, Software Gen5 Version 3.05). In histopathology, acute kidney injury is defined as “acute tubular injury” (ATI) [14]. Thus, tubular injury was quantified by a score established by Rong et al.: presence or absence of epithelial necrosis, loss of brush border, cast formation, tubular dilatation and classified on a five-point-scale: 0: healthy kidney; 1: 1–25%; 2: 26–50%; 3: 51–75%; and 4: 76–100% tubuli affected [31]. In addition, glomerular integrity [13] was quantified in low power fields as follows: 1: 1–25%; 2: 25–50%; 3: 50–75%; and 4: 75–100% collapsed glomeruli.
StatisticsFor statistical analysis GraphPad Prism 7 software (GraphPad Software Inc., San Diego, California, USA) was used. To test for normal distribution the D’Agostino&Pearson as well as the Shapiro–Wilk normality test were used. Statistics were performed using a paired t test or a Wilcoxon matched-pairs signed rank test/Mann–Whitney test if the data were not normally distributed. When multiple measurement timepoints were compared, a repeated measures (rm) ANOVA with Geisser–Greenhouse correction and Bonferroni's multiple comparisons test was used. A P value of less than 0.05 was considered statistically significant. Data are represented as mean ± SEM or boxplot (Tukey).
留言 (0)