This study was designed to analyze the rate of β-cell death in different groups of diabetes mellitus (GDM, T1D and T2D) by two potential biomarkers (INS and Amylin). Our main finding is the detection of β- cell death in pregnant women, both with GDM and non-GDM; and the association with relevant parameters as well as insulin resistance and newborn birth weight in the GDM group.
A large number of studies have been addressed on T1D due to great interest in identifying noninvasive biomarkers that allow us to detect the onset of the disease before the symptoms appear and the β-cell destruction has not been completed yet. Based on the approach of specific methylation pattern from circulating DNA, several studies have reported the presence of β cell-derived cfDNA in individuals at risk of T1D and patients recently diagnosed [10, 11, 22, 24]. However, other authors have shown inconsistent results [25]. In our study, T1D subjects showed the lowest rate of β cell death compared with the other groups. These results are consistent with those recently published by Neiman et al. [25]. These authors showed for the first time the presence of unmethylated Ins cfDNA in T1D subjects [7]. Later, in a more rigorous and exhaustive, they did not observe an increase of β cell-derived cfDNA in autoantibody positive subjects at risk for T1D, individuals with recent onset T1D or those with longstanding disease [25]. These discrepancies could be explained by several facts. On the one hand, the different methodological processes and the confounders variables affecting these assays should be considered: type of sample (serum versus plasma); preanalytical processing (time between collection and centrifugation, double centrifugation); isolation of cfDNA using specific kits, volume of sample and finally, the targeted CpGs sites in INS gene [5, 26, 27]. On the other hand, in our study, the patients who attended to the clinic with a case of hyperglycemia, have probably already suffered the preclinical phase in which the beta cell destruction occurs. So, if T1D is advanced, the number of live beta cells is very low, thus the rate of cell death is also low. The remaining beta cells produce small amount of insulin, what relates to low level of peptide-c. Thus, low level of beta cell markers indicates that there is low number of live beta cells that may undergo death, thereby the rate of beta cell death is the lowest. Maybe this could explain the similar methylation levels in T1D patients and control group. At diagnosis, there is not enough beta cell, and maybe the method is not sensitive enough to detect a signal of β cell destruction in this stage [28]. Even, some authors suggest that autoimmune β cell death does not release such fragments of circulating DNA into the circulation, because they are previously phagocytosed [25]. In any case, our assay did not detect β cell death by these two markers (Ins and Amylin) in recently diagnosed subjects with diabetes.
Regarding to other metabolic phenotypes, to the best of our knowledge, only two studies have explored the presence of this marker in women with gestational diabetes. The first one, performed by Akirav et al. [29], measured levels of unmethylated Ins cfDNA in non-pregnant women, pregnant, pregnant with GDM and postpartum without previous diabetes. They did not find an increase of β cell death in GDM compared with the other groups. The other study analyzed the levels of cell free circulating methylated and unmethylated Ins DNA in plasma of GDM women followed up to 10 years for the development of T2D. Samples were collected twelve weeks at postpartum [30]. They found that postpartum levels of cfDNA Ins marker were significantly higher in those women with a previous GDM who later developed T2D. However, both studies have several limitations and can not be comparable with ours. Samples from Akirav study were obtained from serum and it is known that cfDNA levels in serum appear significantly higher than in plasma due to contamination from genomic DNA (gDNA). Quantification and integrity of cfDNA fragments should be measured. None of these studies used specific kit to isolate cell free DNA to avoid carrying over larger fragments that could indicate genomic contamination. Finally, cfDNA extraction requires of greater volume of sample to obtain enough DNA. Minimum volumes of 1 ml are highly recommended. All these recommendations are being incorporated into the last years according to the literature to guarantee that circulating cell free DNA is properly isolated [26]. One of the main strengths of this study is the rigorous methodology. First, we have processed all the samples following the same protocol and within 4 h post collection. A double centrifugation to minimize the potential for contamination of plasma with cells from the buffy layer were carried out. All the samples were quantified and visualized by the Agilent 2200 TapeStation system to ensure the presence of cfDNA around 200 pb and non gDNA contamination. Moreover, two biomarkers (INS and Amylin) were analyzed for each sample. We have shown that demethylation index of both markers is decreased in pregnant women and there is an association with parameters related with β cell function, as insulin resistance in the GDM group. In addition, among pregnant women with GDM, those with a higher rate of β cell death gave birth newborns with higher birth weight. During pregnancy an increased insulin resistance is produced independently of the metabolic status, to compensate the greater substrate availability required by the fetus. In this period β cell adaptation occurs by increasing mass, number, and glucose-stimulated insulin secretion [31]. This effect is observed in all the pregnant women and could be reflected in a higher β cell death due to a higher turn-over process. In addition, Salazar suggests that the increase in β cell mass occurs in the first half of pregnancy and, when we look at it, we are seeing whether these adaptations have been sufficient to counteract the physiological insulin resistance during pregnancy. Maybe the beta cell death is similar in both groups, but the mass of beta cells that is achieved is lower in those who end up developing GDM and most likely it influences in the development of GDM. This could explain our finding of a higher β cell death in both groups of pregnant women with GDM and non-GDM. Regarding GDM group, we observed an interesting relationship between β cell death and the newborn weight and insulin resistance. This finding is interesting because reinforce what we already know, that GDM pregnant women have newborn with higher birthweight and a worst metabolic profile, but introduce a new variable in this observation, their potential association with beta cell death.
Our data show for the first time that β cell death occurs during pregnancy, and probably this could be more significant in GDM pregnant women, but more studies with larger samples and followed-up over time, are needed.
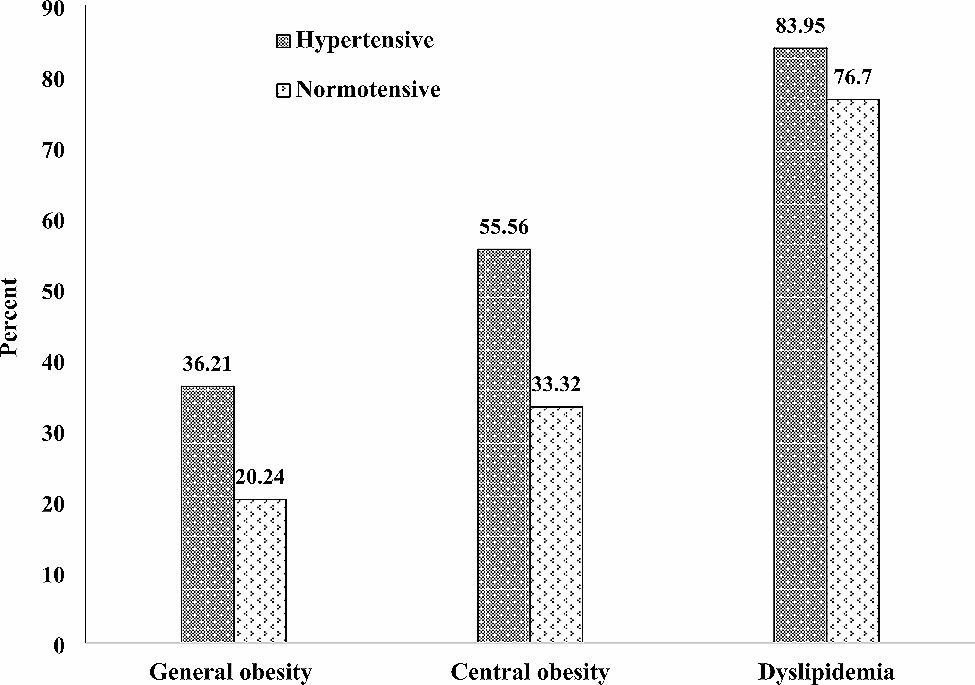
Lastly, our study highlights the use of the demethylated amylin cfDNA index to detect β cell death. Until date, only one study has reported the use of this measurement as biomarker of β-cell loss[14]. We observed the same trend in the demethylation index of Amylin than the Insulin, although none significant associations with other parameter were found. Amylin index showed a more homogenous pattern among the different groups compared with the Insulin as we can observe in the Fig. 1. So, it is possible that a greater number of samples might be required to detect statistically significant differences with this marker.
This study has some limitations. The main one is the number of samples per group. Additionally, this is an observational study, therefore a follow-up to assess the evolution of these biomarkers along the time, would reinforce these results. Finally, it should be mentioned that cell free DNA from maternal plasma contain a small percentage of fetal DNA. However, only the 10% of the total cfDNA is fetal. So we assume that this amount of fetal DNA is minimal compared to the amount we detected from the mother, considering that our results are not influenced by fetal cfDNA fraction [32, 33].
In conclusion, we investigated the use of two potential biomarkers of β cell death in a group of subjects with different type of diabetes. We observed that both markers (INS and Amylin) presented the same trend in the studied groups. The main finding was the detection of β cell death in pregnant women independently of their metabolic status. This rate of β cell loss was associated with increased insulin resistance and newborn weight in GDM women.

留言 (0)