
記住我



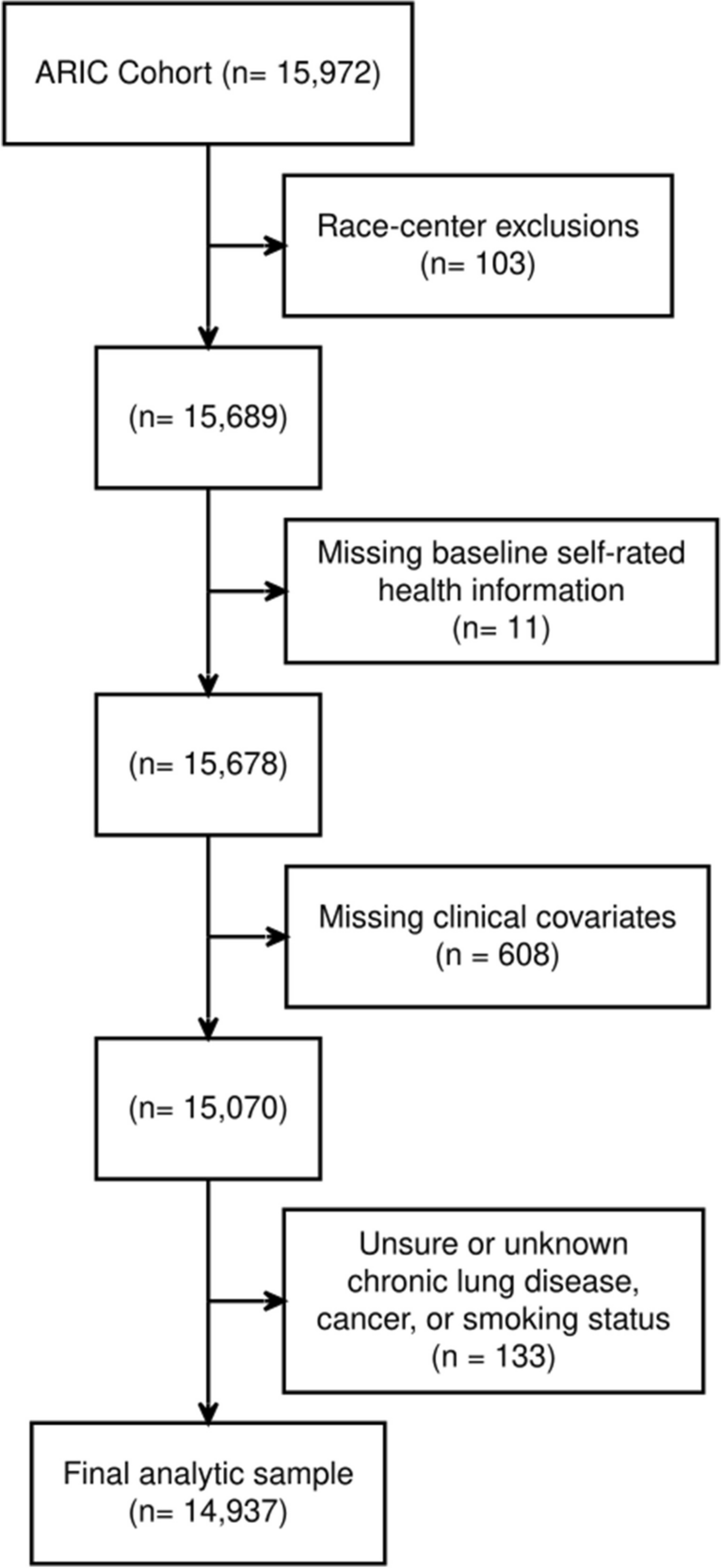

Recruitment flow is presented in Fig. 1. We identified 42 patients engaged in longitudinal follow-up for the parent cohort study and were approximately 1-year post-hospital discharge. We successfully contacted 27 patients, of whom 24 consented to participate. Thematic saturation was achieved after 24 interviews. Participant demographic and clinical characteristics are presented in Table 1 and Appendix C. The majority of participants (71%) identified as Black. Median ADI was 82.5 (interquartile range 50.5, 91), corresponding to severe neighborhood-level disadvantage, with over half of participants (54%) living in neighborhoods with the highest ADI. Baseline comorbidities were reflective of known risk factors for developing severe COVID-19. During hospitalization, most participants (75%) required some form of respiratory support and 33% were admitted to an ICU. Among the 19 participants who completed full functional assessments 1 year after hospital discharge, 15 (79%) reported moderate to severe dysfunction or persistent symptoms on the EQ-5D, WHODAS-2, or MRC, thereby meeting criteria for long COVID.21
Fig. 1
Recruitment of study participants. While the MESSI-COVID study continued to enroll and engage participants in follow-up, recruitment for this qualitative study was stopped at the time of confirming data saturation. Recruitment flow includes only those participants eligible at the conclusion of this qualitative study. *Exclusion criteria for the MESSI-COVID parent cohort included no proxy or necessary interpreter available at time of recruitment (n = 39), desire for exclusively palliative care (n = 38), active enrollment in a clinical trial (n = 14), age under 18 (n = 2), pregnancy (n = 2), severe anemia (n = 2). **Reasons for declining qualitative study participation: “not interested” (n = 1), “insufficient time” (n = 1), “not ready to tell my story” (n = 1).
Table 1 Participant CharacteristicsQualitative findings are organized into four major sections: (1) persistent symptoms, (2) impact on well-being, (3) longitudinal assessments of recovery, and (4) barriers to and facilitators of recovery.
Persistent SymptomsThe majority of participants (88%) described limitations in physical, cognitive, and psychological function during semi-structured interviews. New physical symptoms or changes in functional status included breathlessness, mobility limitations, and fatigue. Some participants also experienced new sexual dysfunction, such as lack of interest in sexual activity, following their COVID-19 hospitalization. Participants described how new symptoms made it difficult to carry out tasks they had easily performed before COVID-19 hospitalization.
The other day, I was sitting down trying to prepare food, and I ran out of breath. I can’t stand at the sink and do my dishes, I run short of breath. These are all common things that I never thought I would have a problem with. (Participant 7)
Ongoing cognitive symptoms, such memory deficits and “brain fog,” were also common. Memory deficits included problems recalling specific information.
I can’t remember stuff at all…If somebody told me something 10 minutes ago, I may forget until they bring it back to my attention. (Participant 15)
“Brain fog” included difficulty focusing and processing new information.
Even now, as you can tell in my conversation, the focus is really bad. You can’t focus. It does something to your mind with focusing. (Participant 22)
Psychological changes included new depressive symptoms such as hopelessness, sadness, and irritability. Others described new feelings of fear, worry, and anxiety. Participants discussed fears specific to their health and mortality and broader fears about the spread of COVID-19. Some participants also described frustration over how changes in their physical and psychological health resulted in lifestyle and relationship changes.
Impact on Well-beingWhen exploring how physical, cognitive, and psychological changes impacted current life and well-being, analysis yielded three major themes: financial hardship, loss of a sense of self, and loss of social connectedness (Table 2).
Table 2 Relationship Between Persistent Symptoms and Domain of Well-beingNew physical and cognitive limitations often resulted in financial challenges. For many participants, absence from work during the acute illness and increased medical bills negatively impacted financial well-being. Participants who were able to return to work felt optimistic their financial hardships would be temporary. However, some participants described ongoing inability to work the job they had before hospitalization due to lingering health effects (often, breathlessness or memory deficits). This resulted in more persistent and profound financial impact and worries about the future.
I still have issues and there’s no way I could do my job right now…Because the focus isn’t there. And as you saw, I just automatically blank out sometimes. (Participant 12)
Participants also described changes in their sense of self. Physical health impairments, like decreased mobility or low energy, and cognitive impairments, like brain fog, meant participants could no longer function in the same occupational or social roles they held before their hospitalization.
I had to have a talk with my children like, I need you all to pick up more and help me out. I just can’t do it. I just don’t have it in me anymore. I’m not the same woman I was before COVID. (Participant 5)
This loss resulted in downstream effects on participants’ occupations and personal lives. For example, one participant who used to take pride in organizational and communication skills described how cognitive changes resulted in feeling out of place and insecure at work. Although they described a supportive work environment in which accommodations could be made, the newly reduced level of function was nonetheless unsettling and insurmountable.
While many participants spoke positively of how their loved ones supported them through recovery, COVID-19 negatively impacted social and relational health for others. This was often because physical and cognitive symptoms limited participants’ ability to interact meaningfully with others.
It’s like [I’m] fearful. I’ve been feeling so [fearful] in my friendships. I have girlfriends, but everybody backed off because I can’t do as much as they do. It’s a little depressing. (Participant 3)
Longitudinal Assessments of RecoveryParticipants described various trajectories of recovery over the year since hospitalization. While many emphasized that they had not fully recovered, most reported they were getting better overall, albeit slowly.
Like I said, I have been getting stronger. I can walk a little more than I used to be able to and so I am getting better. It’s just such a slow process. It’s frustrating. (Participant 13)
Notably, five participants described complete recovery and no persistent impact on their lives. These participants’ EQ-5D, WHODAS-2, and MRC dyspnea scale scores aligned with these qualitative findings.
I don’t have any long lasting [impacts] from physical issues because I worked very hard to resolve them. (Participant 8)
Barriers to and Facilitators of RecoveryParticipants described factors that either hindered or helped recovery. These barriers and facilitators were grouped into system-, clinician-, and individual-level factors (Table 3).
Table 3 Barriers and Facilitators of Recovery at the System-, Clinician-, and Individual-Levels with Exemplary QuotesSystem-level barriers to recovery included social infrastructure deficiencies, such as difficulty securing transportation to appointments and concerns about office accessibility. A main system-level facilitator to recovery was the coverage afforded by participants’ insurance plans, private and public alike, that enabled participants to seek and access necessary healthcare services. Participants also valued the convenience of the hospital system’s patient e-messaging platform during the recovery process.
Many participants felt their clinicians did not address their COVID-19-specific concerns appropriately, communicate with them clearly, or help them to identify effective resources (e.g., diagnostic testing or rehabilitation for persistent symptoms) for follow-up care. There was a general sense that more information should be shared by health professionals about what to expect and how to manage the recovery process, leaving participants feeling alone in seeking out external support. In particular, participants reported their cognitive and psychological needs were under-prioritized relative to their physical health needs.
I don’t know how to access [the care I need]... And I think it’s important this neurological piece, I don’t know in a general sense who would be appropriate or how to access that. (Participant 24)
Some participants reported a high degree of trust in a specific clinician as a facilitator. For such participants, this positive relationship with an individual provider was an outlier relative to their other interactions with the healthcare system. This relationship was critical to their recovery and ability to navigate an otherwise unwelcoming healthcare system.
Participants also reported experiencing stigma about having had COVID-19 in their social circles and skepticism about the legitimacy of persistent symptoms. Some noted that family members lacked consideration for their health. For others, positive family and social relationships facilitated recovery. Positive relationships provided both emotional support and assistance with basic needs and activities of daily living. Out of necessity, many participants took an active role in their own healthcare as a strategy for coping physically and psychologically during their recovery, which involved close monitoring of their own symptoms and intentional engagement with healthcare providers.
Having COVID made me more conscious of my health. I make sure I make appointments that I probably would never have made before…I have to stay up on my health because I want to live... It’s my responsibility. You can’t put that on anyone else. (Participant 5)
Some drew on faith and spirituality as sources of comfort and strength through recovery. Others adopted new mindsets or attitudes which helped them process and cope with their experiences, most notably increased gratitude for life and loved ones.
It made you look at life where you appreciate, and you don’t take anything for granted...I want to experience some things on my bucket list…It’s no more, ‘I’ll get around to it.’ It’s no more going to bed angry... Because you just might not wake up. (Participant 21)
Across participants, there was an emphasis placed on the importance of the individual-level facilitators, as these were the only facilitators to recovery that participants felt they had any control over.
留言 (0)