
記住我
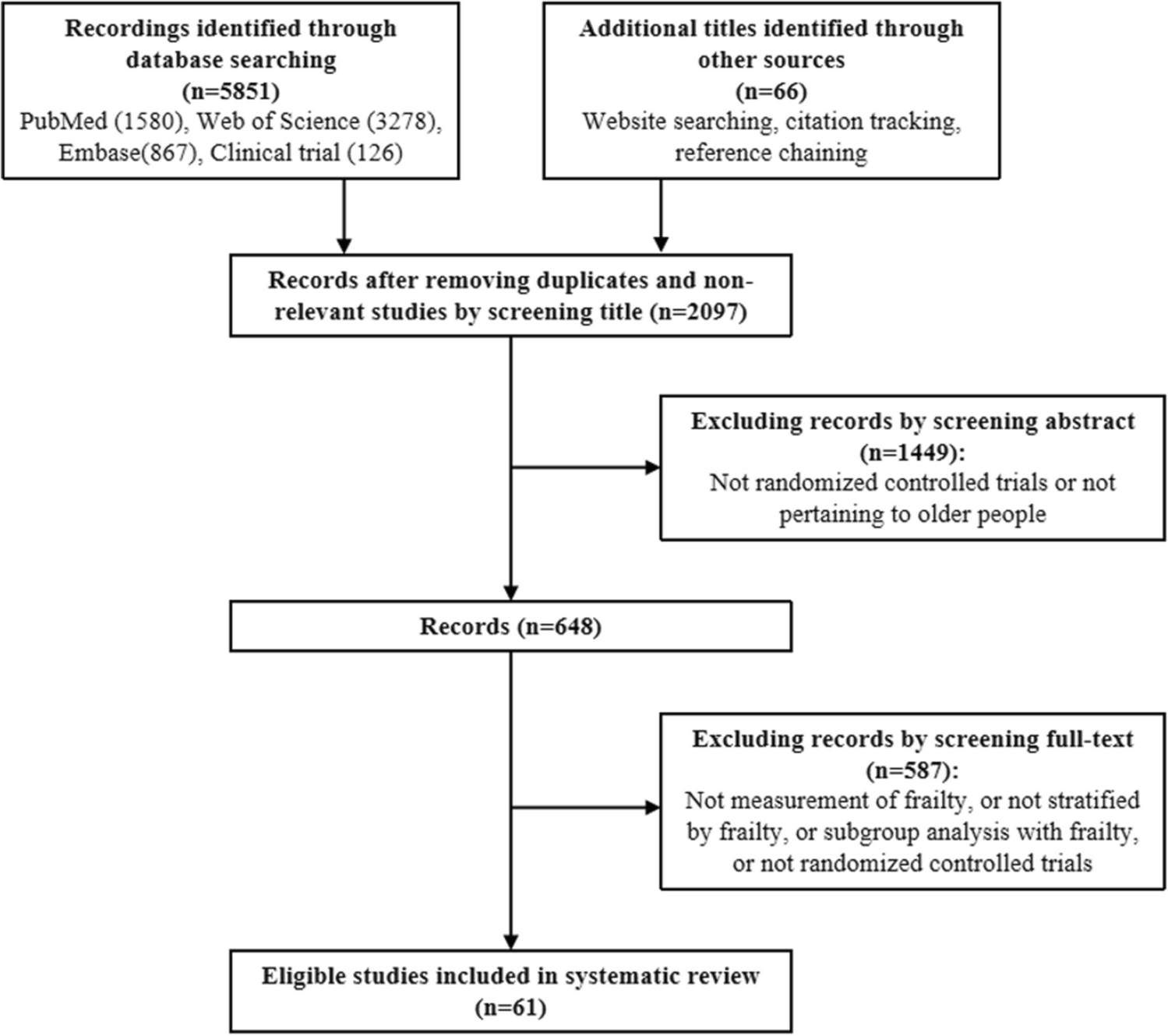



The PRISMA chart is presented in Figure S1. Overall, 26 studies were included in this meta-analysis 11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36. Overall, there were 26 studies involving 8,968,085 participants that were included (Table 1). Sample sizes ranged from 98 to 2,413,356 participants with age ≥ 60 years old and the proportions of men in study populations ranged from 30 to 95%. Of the 26 included studies, 21 studies were prospective or retrospective cohort studies, 5 case–control studies and no randomized controlled trials (RCTs). Included studies came from the US, UK, Qatar, Israel, Spain, Italy, Pakistan, France, Denmark, China, Portugal, Hungary, and Sweden.
Table 1 Characteristics of 26 studiesRelative risks for breakthrough SARS-CoV-2 infection, hospital admissions, and all-cause mortality after one dose of vaccine in the elderlyCompared to unvaccinated elders, one dose did not reduce risk of breakthrough SARS-CoV-2 infection in the first 14–20 days (RR = 0.81, 95% CI 0.63–1.05, I2 = 87%, n = 2 studies). However, by 28–34 days (RR = 0.42, 95% CI 0.37–0.49, I2 = 0%, n = 3 studies) and 35–60 days (RR = 0.49, 95% CI: 0.37–0.62, I2 = 47%, n = 4 studies), one dose decreased risk of breakthrough SARS-CoV-2 infection (Fig. 1A).
Figure 1
RRs for breakthrough SARS-CoV-2 infection, hospital admissions, and all-cause mortality after the first dose of vaccine (A) RRs for breakthrough SARS-CoV-2 infection associated with the first dose of vaccine (B) RRs for hospital admissions and all-cause mortality associated with first dose of vaccine. (Both: BNT162b2 and mRNA-1273; Any: BNT162b2 or ChAdOx1 or mRNA-1273, et al.)
One dose also reduced the risk of hospital admissions (RR = 0.43, 95% CI 0.37–0.51, I2 = 72%, n = 4 studies; (Fig. 1B)) and all-cause mortality (RR = 0.59, 95% CI 0.47–0.74, I2 = 68%, n = 3 studies; (Fig. 1B)).
Relative risks for breakthrough SARS-CoV-2 infection, hospital admissions, the severity of disease and all-cause mortality after two doses of vaccine in the elderlyThose receiving two doses had decreased breakthrough infections compared with the one or no doses (RR = 0.37, 95% CI 0.32–0.42, I2 = 59%, n = 9 studies; (Fig. 2)). Compared to the first-dose vaccine or unvaccinated group, the two-dose vaccine group also decreased hospital admissions (RR = 0.25, 95% CI 0.14–0.45, I2 = 86%, n = 10 studies; (Fig. 2)), disease severity (RR = 0.38, 95% CI 0.20–0.70, I2 = 47%, n = 4 studies; (Fig. 2) and mortality(RR = 0.21, 95% CI 0.14–0.32, I2 = 53%, n = 3 studies; (Fig. 2).
Figure 2
RRs for breakthrough SARS-CoV-2 infection, hospital admissions, the severity of disease, and all-cause mortality after two-dose of the vaccine
Relative risks of breakthrough SARS-CoV-2 infection, hospital admissions, and all-cause mortality after three doses of the vaccine in the elderlySimilarly, the three-dose vaccine group showed a decreased risk of breakthrough infection (RR = 0.14, 95% CI 0.10–0.20, I2 = 82%, n = 3 studies), hospital admissions (RR = 0.11, 95% CI 0.07–0.17, I2 = 76%, n = 4 studies), and all-cause mortality (RR = 0.10, 95% CI 0.02–0.48, I2 = 74%, n = 3 studies) compared to the two-dose vaccine or less group in the elderly (Fig. 3).
Figure 3
RRs for breakthrough SARS-CoV-2 infection, hospital admissions, and all-cause mortality after three-dose of the vaccine
Relative risks for breakthrough SARS-CoV-2 infection, hospital admissions, the severity of disease, and all-cause mortality after four vaccine doses in the elderlyThe four-dose vaccine group was associated with decreased breakthrough infections when compared with the three-dose vaccine group (RR = 0.46, 95% CI 0.40–0.53, I2 = 78%, n = 4 studies; (Fig. 4)). Compared with the three-dose vaccine group, the four-dose vaccine group also showed a decreased risk of hospital admissions (RR = 0.42, 95% CI 0.32–0.55, I2 = 87%, n = 4 studies; (Fig. 4)) and disease severity (RR = 0.44, 95% CI 0.35–0.57, I2 = 83%, n = 4 studies; (Fig. 4)). Similarly, pooled results from four studies indicated that a four-dose vaccine was associated with a decreased risk of mortality compared with the three-dose or fewer vaccine group (RR = 0.48, 95% CI 0.28–0.84, I2 = 88%, n = 4 studies; (Fig. 4)).
Figure 4
RRs for breakthrough SARS-CoV-2 infection, hospital admissions, the severity of disease, and all-cause mortality after four-dose of the vaccine
Subgroup and meta-regression analysis of relative risks for hospital admissions, the severity of disease and all-cause mortalityAge, sex, comorbid conditions, and vaccination type were potential confounders related to hospital admission, disease severity and all-cause mortality. As shown in Figure S2, the estimated RR indicated that age groups 60–74 years and ≥ 75 years experienced a decreased risk of hospital admissions in the vaccinated group (RR = 0.42, 95% CI 0.33–0.53; RR = 0.33, 95% CI 0.16–0.65, respectively) compared to the unvaccinated group. Similarly, the estimated RR indicated that age groups 60–69 years and 70–79 years were also associated with a decreased risk of the severity of disease (RR = 0.45, 95% CI 0.30–0.68; RR = 0.53, 95% CI 0.36–0.79, respectively; Figure S3). Furthermore, in the vaccinated groups, it was found that age groups 60–79 years (RR = 0.59; 95% CI, 0.47–0.74), age groups ≥ 80 years (RR = 0.76; 95% CI, 0.59–0.98), female (RR = 0.66; 95% CI, 0.50–0.87), male (RR = 0.58; 95% CI, 0.44–0.76), and coexistence with CVD (RR = 0.69; 95% CI, 0.52–0.92) and DM (RR = 0.59; 95% CI, 0.39–0.89) showed a significantly lower risk of all-cause mortality in comparison with the unvaccinated group (Figure S4). The meta-regression demonstrated that sample size and comorbid conditions influenced the hospital admissions, vaccine dose and comorbid conditions influenced the severity of disease, and study design and comorbid conditions influenced all-cause mortality. The summary of the meta-regression of the hospital admissions, the severity of disease and all-cause mortality among vaccinated groups can be found in the Supplemental Table 2.
Comparison of efficiency of homologous and heterologous vaccinationAll two dose studies were homologous vaccinations. Only three trials reported on heterologous vaccination after three or four doses of vaccination. Both of the homologous and heterologous vaccination had similar effects in the prevention of hospital admission and mortality due to SARS-CoV-2 infection (Figure S5).
Sensitivity analysis and publication biasNo study was overly influential, excluding any single study did not change our results. We also found no evidence of publication bias was found in the pooled studies on breakthrough infection, breakthrough infection (p = 0.17), disease severity (p = 0.77) or all-cause mortality (p = 0.53). However, there was a significant publication bias in hospital admissions (P = 0.03). After adjustment for potentially missing studies, hospital admissions was reduced among those who were vaccinated (RR: 0.346, 95% CI 0.285–0.420).
Risk of bias assessmentThe detailed risk assessment for the included studies using the ROBINS-I tool is shown in the Supplemental Table 3. Eight studies were assessed as low risk of overall bias; 18 studies were graded as of moderate risk of overall bias. No studies were assessed to have severe or critical bias.
留言 (0)