We have demonstrated for the first time that a phantom which is capable of mimicking differential radiotracer uptake by normal and tumoral pituitary tissue can be created using radioactive 3D printing. Importantly, the model allowed the phantom tumors to be placed in direct contact with the phantom normal gland, thereby replicating the situation found in patients where tumors are often embedded within the normal gland. In addition, we housed these pituitary gland phantoms in a MEX 3D printed skull that approximated the attenuation properties of surrounding bone and soft tissue. Using this bespoke phantom, we were able to optimize parameters for pituitary gland imaging using a well-defined ground truth.
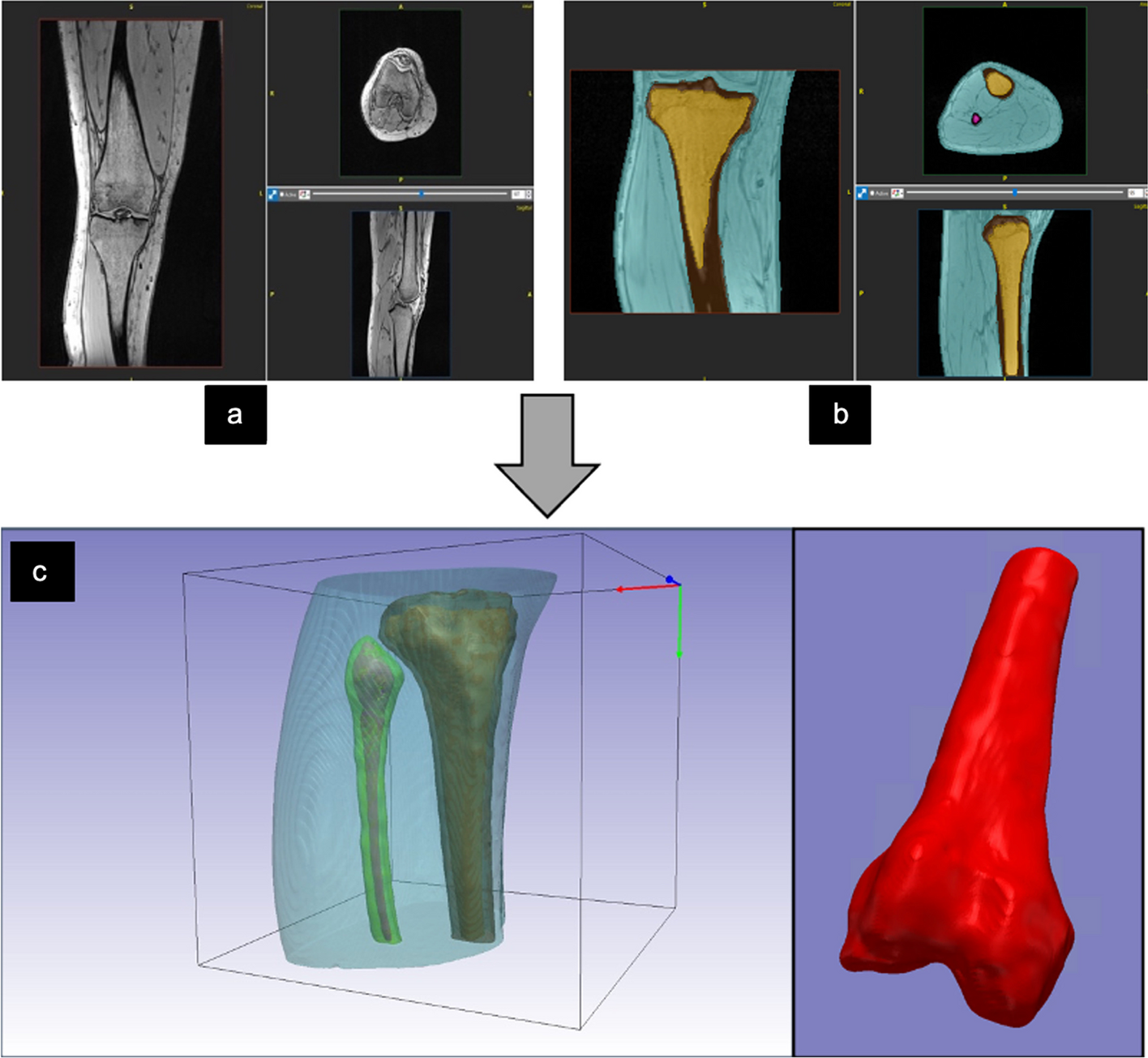
Three-dimensional printing of the pituitary gland and tumors using radioactive resin (Fig. 1) has a number of advantages over traditional fluid-filled phantoms. In particular, the absence of an inactive boundary (between the pituitary gland and tumor) improved our confidence when optimizing image parameters beyond what is possible using patient data alone (where the radioactive concentrations are unknown). Another advantage is that filling a sphere with radioactive liquid is difficult when using very small volumes (e.g., 34 μl for a sphere 2-mm in diameter), and is coupled with the potential for unwanted elongation of the sphere (along the filling tube). Moreover, filling small volumes is more challenging when using liquids with a high surface tension (such as water) because air may become trapped.
A potential disadvantage of radioactive 3D printing is occasional printing failure as experienced in this study, where one of the nine phantoms (5:1 6-mm lesion) did not print. This is a recognized issue with 3D printing and can, to some degree, be overcome by printing multiples of objects in different locations on the build plate.
At our center, PET imaging of the pituitary gland is usually performed using 11C-methionine, and therefore, the use of 18F in the phantom could have had an effect on the results. The reason for this is because 18F has a shorter mean positron range of 0.6 mm in water compared to 11C, which has a mean range of 1.2 mm [20]. However, the very short half-life of 11C (20 min) made it impractical to use this radiotracer in this work due to the large amounts of activity that would have been required to enable the same radioactive 3D printing.
Creating the phantom using patient images was relatively simple and the methodology described here (Fig. 2) could be applied to other similar phantoms (e.g., a small parathyroid adenoma embedded in the thyroid gland). A further improvement might be to split the phantom in a non-horizontal plane, thus avoiding the creation of an air gap which correlates with just one or two slices of the CT. Printing the surrounding anatomy using two materials was successful and enabled us to approximate the attenuation properties of the adjacent structures (Fig. 3). Other workers have recently demonstrated that the use of alternative materials (such as wood filled filaments) may provide attenuation properties that even more closely approximate those of soft tissues [21].
The Prusa MMU2 uses one nozzle and switches between materials by automatically extracting the filament and loading another; this is known as a tool change. During the printing of the phantom, almost every layer contained both materials and therefore approximately every other layer required a tool change. Accordingly, there were approximately 100 tool changes during the printing of each half of the phantom and, due to the complex nature of these changes, these accounted for the majority of the printing errors which occurred during the early phase of the project. Most of these errors could be rectified and the print could continue, but in some cases they necessitated abandoning the printing. In the majority of cases, the error occurred while the concrete-filled filament was either being loaded or unloaded, reflecting the brittle nature of the concrete-filled filament. Two changes to the printing setup reduced the frequency of these errors: firstly, ensuring the concrete filament was very dry and, secondly, that the tension on the filament gears was not too high. An alternative to the MMU2 would be a 3D printer that had two or more separate extruders.
Material extrusion 3D printing is commonly done using an infill percentage of approximately 20%; therefore, 80% of the internal volume is empty. This saves material, lowers costs and shortens print times significantly. However, a large proportion of our phantom required printing solid (effectively an infill of 100%) and therefore used a large amount of filament and was time-intensive. Using the default printer nozzle diameter of 0.4 mm and a layer height of 0.2 mm, each half of the phantom took approximately 60 h to print. These settings are optimized for printing aesthetically pleasing objects (e.g., 3D printing of a pituitary gland containing a tumor for educational and surgical planning purposes) [22]. Therefore, we elected to use a 0.8-mm nozzle and a layer height of 0.4 mm. These changes reduced the printing times for each half of the phantom to around 24 h because more material could be laid down per unit of time and, because there were fewer layers, there were also fewer tool changes. However, one disadvantage of printing with thicker layers is that making watertight printed objects is more challenging. As such, the final object had to be sealed after printing and a gel was used instead of water to mitigate the risk of leaking from the phantom.
Blinded review of the images was carried out using a purpose-built web-based tool (Fig. 3), which allowed us to assess both accuracy and confidence for each reconstruction type. In a clinical context, confidence when interpreting and reporting Met-PET is an important factor in key decision-making, e.g., when considering whether repeat surgery should be offered to a patient who has persistent disease despite primary surgery. Overall the confidence ratings for true positives were higher than for true negatives and, importantly, than for false positives and false negatives (Table 3). This finding likely reflects the way Met-PET is most commonly deployed in clinical practice, where it is used as a tool to confirm that a suspicious area on MRI is indeed the site of active disease; however, equally importantly, the false positive rate must be kept low so as to avoid recommendations for inappropriate surgery. Accordingly, a balance must be struck between the highest sensitivity without a detrimentally higher false positive rate, especially one with a high confidence rating. The optimal reconstructions for sensitivity, specificity and accuracy were all different. As anticipated, the highest sensitivity and highest specificity reconstructions were at the highest and lowest noise levels, respectively. The optimal combination of accuracy and confidence was achieved with BPL reconstructions and β values of 300, 400 and 500. Combining the metrics in this way, ensured that reconstructions which performed well but had low confidence would not score as highly as true calls that were made with confidence. Confidence ratings were recorded on a scale from 0 to 4 thus ensuring that “not confident at all” ratings did not contribute to the combined score, i.e., the nature of the call was not relevant when the call was made with no confidence.
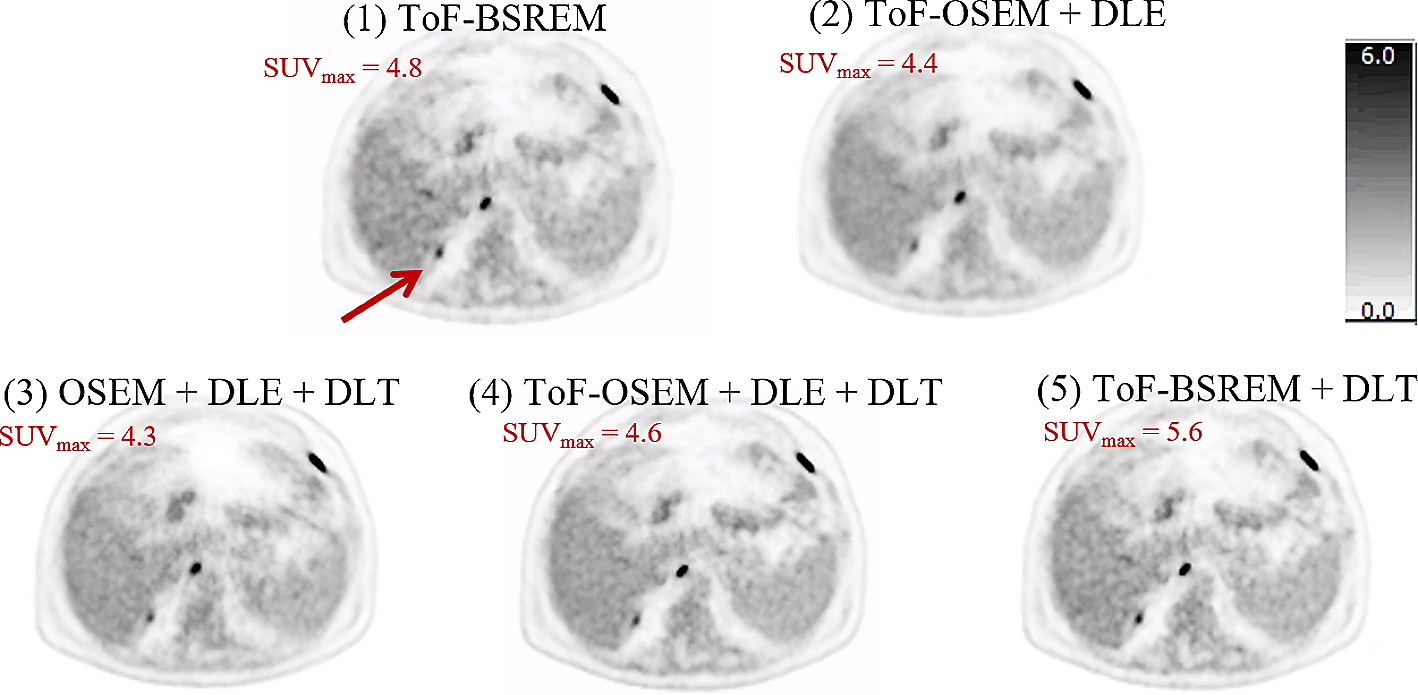
The implementation of TOF made an important difference in the visual appearance of the images as well as quantitatively (Fig. 4). In some cases, tumors were only visible when TOF information was used. The most likely reason for this is that the OSEM reconstruction converges more quickly when the TOF information is included. The observed differences suggest that using TOF is an important factor when imaging the pituitary gland, especially when tumors are small. However, in systems without TOF capabilities this deficiency may be partly overcome by allowing the reconstruction algorithm to converge more fully. However, as we have demonstrated here, noise increases with the number of iterative reconstruction updates.
The use of point spread function correction increased signal in the tumor but did not have detrimental effects on the appearance of the normal pituitary gland without a tumor (Fig. 5). The profiles that can be seen in Fig. 5 highlight that PSF could make an important contribution in clinical cases where a tumor is not seen clearly.
The two voxel sizes examined in this work yielded similar findings: qualitatively, especially with visual interpolation, only a subtle difference was observed; quantitatively, the smaller voxel size increased maximum signal and contrast (reflecting the partial volume effect having less influence). Importantly, noise was not increased by the smaller voxels. Therefore, based on these marginal improvements, the smaller voxel size has been adopted for use in clinical practice in our center. Another area of potential improvement might be to use smaller slice intervals. Unfortunately, the scanner was unable to reconstruct in thinner slices, which precluded such comparison, but if the same pattern was seen as with the voxel size then this may also improve signal and contrast. Caution would need to be applied here though, as the levels of noise may become problematic if the voxels were made smaller again.
The use of a post-reconstruction filter is ubiquitous when using OSEM and its effect can be significant. It is therefore crucial to optimize the parameters of the filter to achieve a compromise between images that are too noisy or too smooth. In this study, we used three Gaussian filters with FWHMs of 1, 2 and 3 mm. The 1-mm filter did not smooth the noise sufficiently to be used clinically (Figs. 5 and 6), as non-tumoral areas that might be considered potential sites of increased tracer uptake could be seen. This appearance would be particularly problematic if encountered during optimization performed using datasets from patients or healthy volunteers because of the difficulty in establishing the veracity of such a finding without recourse to potentially inappropriate surgery. However, using the phantom, the nature of this positive signal is not in doubt (i.e., a false positive finding) and accordingly the 1-mm Gaussian filter would present challenges if adopted in clinical practice. On the other hand, while the 3-mm Gaussian filter was less likely to generate false positive results, the maximum signal over the tumor was notably diminished. Accordingly, a 2-mm Gaussian filter which balanced signal and noise was preferred.
We also investigated the impact of the number of OSEM iterations, comparing 3, 5, 7 and 9, each with 24 subsets. Signal and contrast were enhanced with increasing iterations; however, noise also increased. Despite this, increasing the number of iterations may potentially augment the detection of small tumors, and therefore, further work is required to explore the potential benefits and limitations of such an approach in clinical practice. For now, based on the preliminary findings reported here, the use of three iterations and 24 subsets is recommended to achieve both accuracy and confidence (Table 3).
The BPL algorithm gave rise to a wide range of results depending on the β values. When the β value was low, the signal was highest, but so was the noise. For some phantom setups, the lowest β value gave the highest contrast but, when compared with other β values in the blinded evaluation, also generated the highest false positive rate. A potentially important observation at low β values (and which was also noted at higher OSEM iterations) was the erroneous impression of increased tracer activity at the lateral margins of the pituitary phantom, (which were reported as potential tumor sites by several of the expert readers), and which is best appreciated in Figs. 10 and 11. The observed visual anomalies may be linked to edge artifacts, a type of distortion caused by reconstructed images that incorporate PSF correction, commonly referred to as Gibbs artifacts [23]. For the expert evaluations, the highest sensitivities were all observed at low β values, with the highest seen when β = 100. Specificity was highest when β was highest (1000), while accuracy was highest when β = 400. Accordingly, and depending on the imaging task in hand, it may be prudent to consider using different reconstruction parameters for different tasks.
In clinical practice, the most common reasons for performing molecular imaging of the pituitary gland are: (1) to confirm/reveal the site of a small tumor when anatomical imaging (e.g., MRI) is indeterminate; (2) to accurately localize site(s) of residual/recurrent tumor following primary therapy when further potentially curative treatment (e.g., surgery, stereotactic radiosurgery) is being considered. In these contexts, it is critically important that the reconstruction does not produce false positive findings that are held to be true with a high degree of confidence. Therefore, those parameters with the highest summed confidence (which applied a negative weighting to the false calls) are likely to represent the optimum reconstructions for confidently identifying tumor sites that are appropriate for targeted intervention.
Our results indicate that BPL reconstruction with a β value of 400 has the highest accuracy and one of the highest summed confidence scores. Another important factor is the sensitivity, and this was highest when BPL reconstruction had a β value of 100. Importantly, for those without access to BPL reconstruction, the OSEM reconstruction with TOF, PSF correction and nine iterations and 24 subsets had almost as high sensitivity.






留言 (0)