We aimed to identify factors associated with the choice of treatment modality in the treatment of locally advanced oesophageal cancer. The overall clinical status of the patients and the stage of cancer guide the choice of treatment modalities, leading to overtreatment.
General condition of the patient, the extent of the disease, the location of the tumour in the oesophagus, weight loss, but not age or gender, were associated with the choice of the treatment modality. Thus, patients with better prognoses were more likely to be operated after chemoradiation.
In the present study population, surgery was performed on 42.7% of patients after CRT, which is consistent with the previously reported 27–58% [5, 12, 14]. Surgery was planned for 61% of the patients, but due to advanced disease or poor performance status, not implemented for all of those. After nCRT + S, pCR was achieved in 28 patients (44%). The mOS of 60 months after nCRT + S in the present study was better than in most previously reported studies, where mOS has been 16–62 months [3, 4, 11, 12]. For patients with pCR mOS was yet not reached, raising the question whether surgery was needed for all cases. However, as stated in a recent review [17], these complete responders are difficult to identify before surgery.
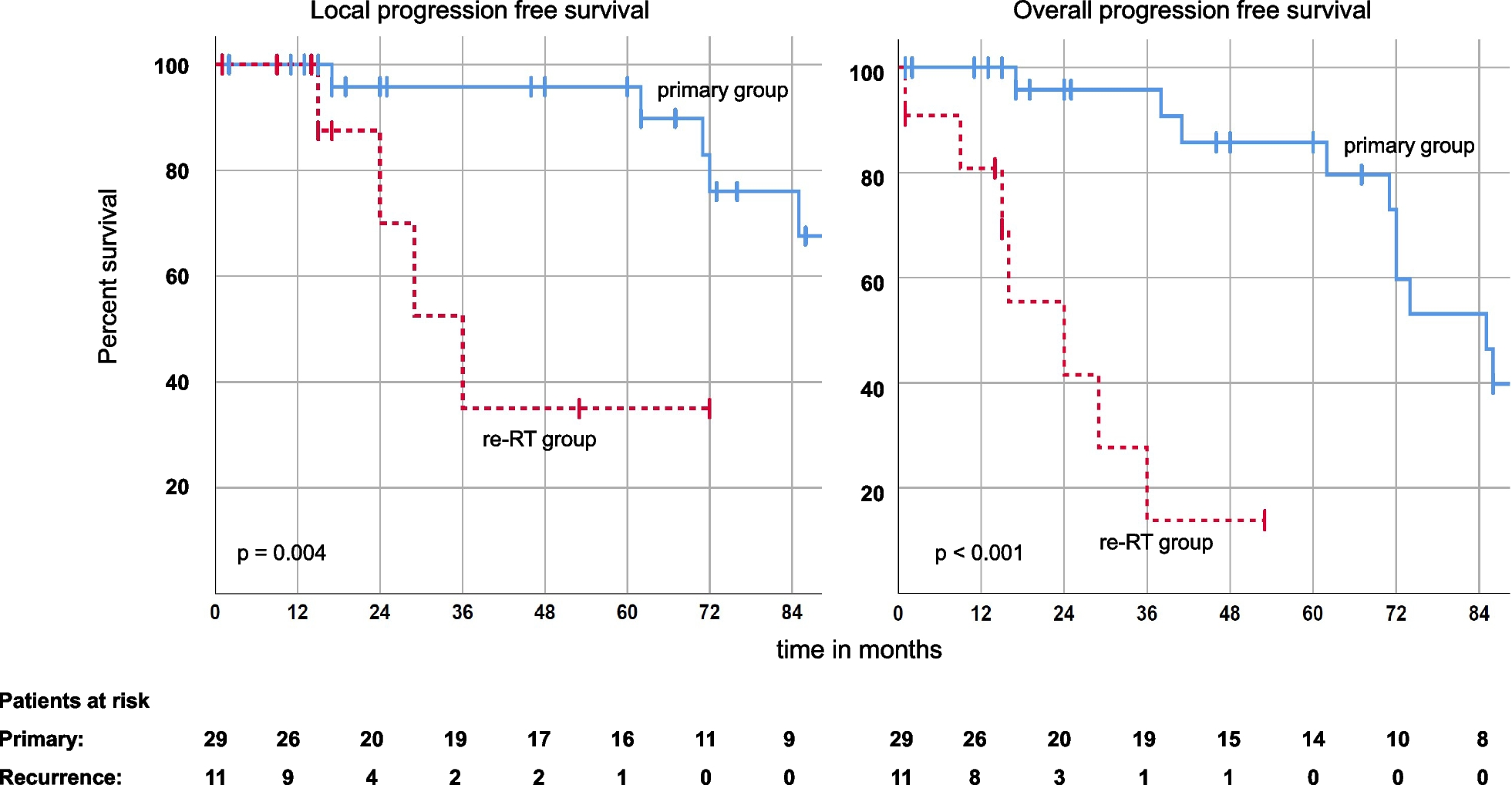
In two previous randomized studies [3, 4] of mostly squamous cell carcinomas patients like in the present study, no superiority of nCRT + S over dCRT in OS was found, but [3, 4] the local recurrence rate was lower after nCRT + S. In our study, both mOS and median local recurrence free survival were better after surgery, apparently due to selection of the patients. It seems that surgeries were performed on all eligible patients, even though according to the randomized studies [3, 4], these patients did not necessarily benefit from surgery. In contrast, mOS after CRT was poorer in our study (10 months) when compared with the previously reported 11–28 months [3, 4, 11,12,13]. Our population differed from the previous ones, that we also included stage IVb patients. In addition, in our cohort some patients received only the preoperative dose of 41.4 Gy, which is below the recommended radiation dose in definitive setting [1], because the planned surgery was nor performed. This highlights the importance of initial clinical evaluation, to avoid too low radiation doses, when the probability of surgery is minimal. However, considering the fact that 10 patients (12%) died within 3 months after completion of CRT, patient selection for CRT was likely not optimal. It is likely that the patients were too fragile, and the cancers were too advanced. The rather large percentage of chemotherapy interruptions (33% in the whole cohort) and the 12 patients who were excluded from this study after interrupting radiotherapy may also indicate that some patients were overtreated.
At the time of the study, multidisciplinary teams (MDT) were not involved in the decision making. MDT are essential part of treatment, especially in gastroesophageal cancers, as stated in recent ECCO guideline [16]. The purpose of MDT is to evaluate treatment plans multidisciplinary together with oncologists, radiation oncologists and surgeons to optimise the treatment. Extended MDT with geriatricians and palliative specialists is needed to plan treatment for patients with poor performance status and advanced disease to avoid overtreatment.
In multivariate analysis, the only other significant association with mOS besides surgery was current smoking, which increased the risk of death by 2.02-fold compared to never-smokers. The impact of smoking on the poorer prognosis of patients treated with CRT has also been shown in a previous study [15]. This emphasizes the importance of smoking cessation.
Lung radiation dose was associated with survival outcomes in a previous study[10]. In our study although patients with smaller lung and heart radiation doses seemed to have better mOS, the differences were not statistically significant. The positive association between lung dose and T stage could at least partly explain this difference.
After surgery, almost half (48%) of the patients had pulmonary complications (e.g., pneumonia or pleural effusion) and 28% had gastrointestinal complications (e.g., anastomosis leakage, ileus). This is consistent with previous studies (pulmonary complications in 25–63% and gastrointestinal complications in 22–23%) [2, 8, 9, 18]. We did not find a correlation between complications and dosimetric factors. Previous studies suggested a correlation between lung radiation dose and postoperative pulmonary complications and heart radiation dose and cardiac complications [8, 10, 19]. Despite these reported complications, postoperative mortality remained low.
There are some limitations of this study. This includes the retrospective design and therefore the lack of more detailed information of the decision making. Of note, for the generalizability of our finding, our cohort consists of only a few patients with adenocarcinoma, based on the clinical practice of treatment of adenocarcinoma with neoadjuvant chemotherapy instead of chemoradiation. Propensity score matching was not possible due to patient heterogeneity and the small number of patients. The strength of this study is its population-based real-life data that demonstrate how treatment modalities are chosen outside of the RCTs.








留言 (0)