Relevant clinical outcomes
Our results demonstrate the benefits of performing ESPB before spinal fusion surgery in terms of perioperative opioid consumption and pain control and improving the hospital experience of patients. These benefits come at no additional cost in terms of clinical safety or significant side effects. ESPB can be safely and rapidly performed, without causing any delay in the surgical schedule.
Spinal arthrodesis is one of the most painful surgeries among the procedures commonly performed. The requirement for this operation is increasing in recent years, with significant costs in terms of quality of life and economic impact on the health system. This study demonstrates how ESPB can reduce the pain and opioid consumption of patients, at the same time reducing the stress and discomfort of the hospital experience. The reduction of opioid consumption also potentially reduces the risk of adverse effects, such as PONV, constipation, delayed awakening and mobilisation and the risk of chronic abuse, although specific data on these aspects were not available for statistical analysis.
Covering a wide variety of surgical interventions, including thoracic levels and traumatic patients that have never been addressed in previous studies, our protocol is strongly suggestive that ESPB should be implemented in clinical practice not just for degenerative lumbar spinal diseases, but also for traumatic fractures. To date, limited scientific literature is available on this topic describing such a broad approach: our results suggest the need for further specific clinical trials.
LOS did not differ significantly between the groups, but we cannot consider it a reliable indicator of ESPB efficacy because of the lack of an implemented early recovery after surgery (ERAS) protocol for fast-track surgery in our hospital and due to the many different types of surgeries included in this study. LOS in our study is in agreement with that reported in the scientific literature [15]. Rethinking a more comprehensive ERAS approach to spinal surgeries, including the ESPB, might reduce the economic burden on health systems, but new studies are needed in this direction.
Reduced pain and opioid consumption, together with a comprehensive ERAS approach and reduced LOS, should theoretically hasten the mobilisation of the patients and reduce their need for thromboprophylaxis or risk for venous thromboembolism, which is a crucial issue in neurosurgery [18, 19].
When this study was being planned, it was the only prospective randomised controlled study applying ESPB in spinal fusion surgery in western Countries. The only European study at that time was a retrospective registry analysis in the Netherlands [20] on patients undergoing posterior lumbar arthrodesis. That study only detected a slight reduction of NRS with ESPB and no differences in terms of opioid consumption and LOS, despite describing a clinical protocol similar to that of our study (ropivacaine 0.375%, in prone position after GA induction).
A recent study by Avis et al. [21] performed in France investigated a slightly larger sample size (50 patients), concluding that ESPB has no efficacy in terms of NRS and morphine consumption despite a similar locoregional protocol (ropivacaine 0.375% 20 mL per side, performed after GA induction). GA was maintained with ketamine and sufentanil and the total dose did not differ between the two study groups. This opposes our findings in the unblinded part of the study, that demonstrated improvements in the intraoperative analgesia due to ESPB. The analgesic effects of ketamine and a more complete multimodal analgesia (as supported by ERAS protocols) approach were adopted in the Avis study, probably diluting the effect of ESPB, which was just a single component of a comprehensive approach. They included lumbar spinal fusions of 2 or more levels exclusively, excluding spinal arthrodesis at thoracic levels; our inclusion criteria were wider and focused on the most common multi-level spinal surgeries involving traumatic fractures of the thoracolumbar spine. Interestingly, Avis et al. [21] assessed the three months postoperative pain and no long-term benefits from ESPB were detected.
Studies reporting ten other clinical trials developed in Asia were available and retrieved. The cultural approach and clinical susceptibility to pain of the different ethnicities involved, together with the differences in healthcare systems could limit their significance in Western Countries. The extreme variability of GA methods, ESPB techniques, and postoperative analgesia protocols and drugs used might limit their reproducibility and increase the number of possible confounders. Most of these studies did not include thoracic levels nor ASA III patients, focusing on different types of lumbar surgeries. Only the studies by Singh et al. [8], Zhang et al. [9], and Yayik et al. [10] included ASA III patients, while only three studies [7, 10, 20] used ropivacaine as a local anaesthetic for ESPB with a concentration similar to our study (0.3–0.4%, 20–25 mL per side), but without the addition of dexamethasone (4 mg per side).
Overall, these studies revealed similar results, with significant benefits in terms of pain scores and opioid consumption during the first 12–24 h following ESPB, but these beneficial effects faded in a shorter time than in our study. Only a few authors assessed the intraoperative use of opioids [12] showing lower pain scores in the ESPB group, and detected benefits in terms of decreased incidence of PONV, [12, 22, 23] need of rescue doses, [23] decreased incidence of LOS, [22] and reduced blood loss. [24] None has evaluated the satisfaction of the patients at the end of the 48 h-postoperative period.
As reported by the analysis of De Cassai et al., [25] the safety profile of the ESPB is extremely encouraging also at the thoracic level. The present study has not detected an increased rate of adverse effects. Further studies on ESPB and its implementation in ERAS protocols for spine surgery in degenerative and traumatic disease at thoraco-lumbar levels should not be delayed by unjustified concerns.
Potential limitations and biases
The major limitations of our study are mostly due to the loss of clinical information. It was not possible to collect data about the exact duration of ESPB performance, the duration of GA, and surgical intervention from the operation theatre;. From the ward it was not possible to collect or retrieve data about PONV, rescue ketoprofen doses, required PCA doses (not just dispensed) and NRS on movement; considerable data were missing at 48 h, limiting their relevance. This was probably due to the non-academic nature of our institution, lacking dedicated research facilities and personnel, but this did not affect the measurement and reliability of primary and secondary outcomes. Anyway, this could also be interpreted as a strength of this study: the positive outcomes recorded were measurable and significant already during the everyday clinical practice, with no extra-fundings required, and presumably impact the real postoperative process of the patients.
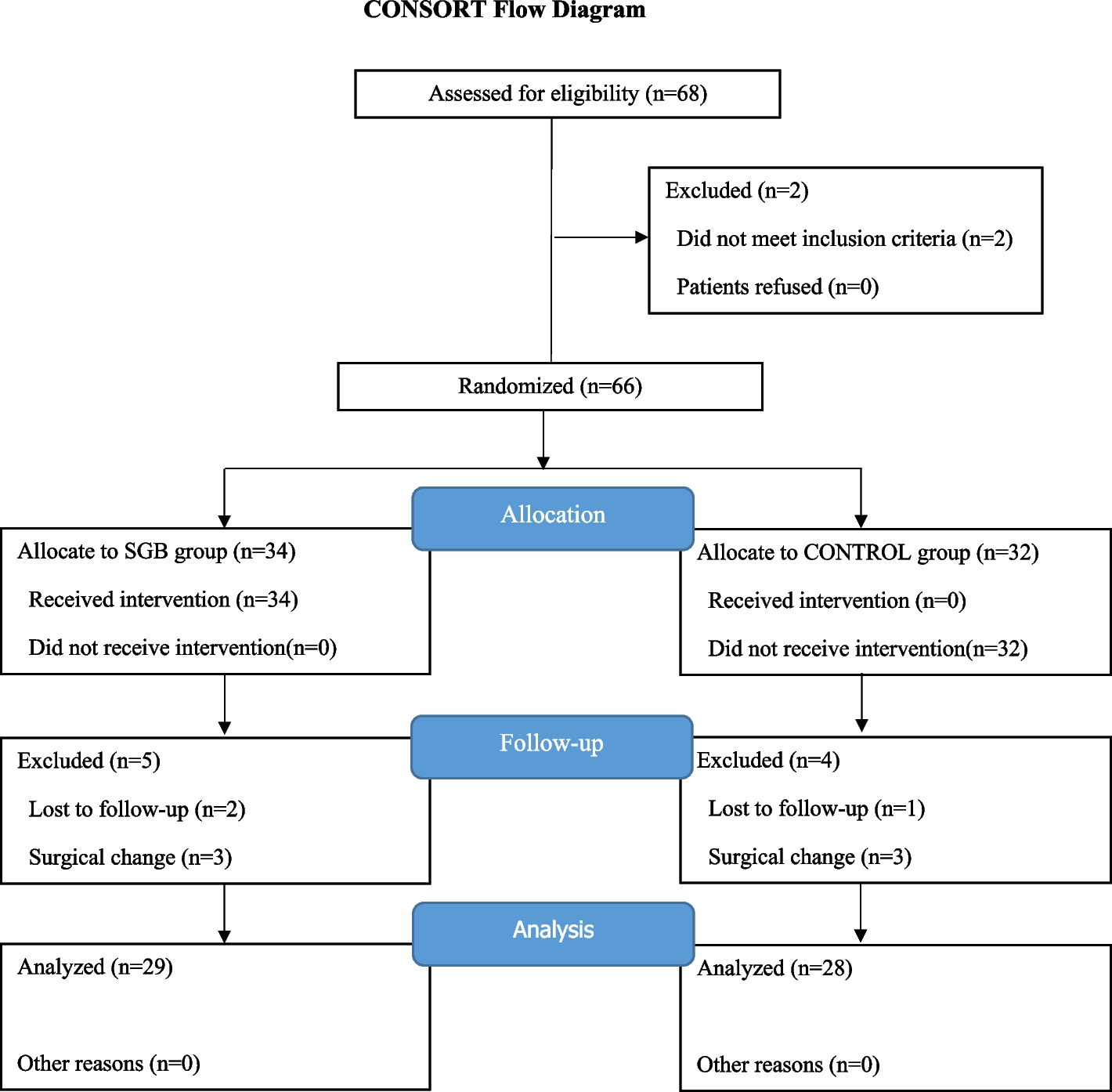
The limited sample size was a consequence of the COVID-19 pandemic and the slowing down of daily clinical practice:. despite a 6-month extension of the study insurance, it was not possible to respect the expected enrolment pace.
Another possible source of bias was regarding the intraoperative use of fentanyl: the unblinding of the anesthesiologists to the ESPB procedure, might affect their propensity to administer the drug. All the other steps have been standardised and are reproducible by other authors. Finally, due to the monocentric nature of the study, the reproducibility might be reduced and the results affected by local practices.

留言 (0)