


記住我








Increased cardiovascular risk is found in the pediatric and adult populations with chronic kidney disease (CKD) (1, 2). Patients with impaired renal function are exposed to a higher incidence of both classic risk factors, such as hypertension, and non-traditional ones such as anemia, oxidative stress, chronic inflammation and others (3, 4). Damage to the heart and vessels is already observed in the early stages of CKD - in children and adolescents it manifests itself in the form of thickening of the intima media (IMT) and left ventricular hypertrophy (LVH) (5). Both IMT, as a marker of atherosclerosis, and LVH are associated with increased risk for cardiovascular events (6). Despite the undoubted progress in the detection of significant cardiovascular risk factors in the population of patients with CKD, it has not been possible to significantly reduce this risk. In addition to the known difficulties in obtaining good blood pressure (BP) control, compensation of calcium and phosphate metabolism disorders or effective treatment of overhydration in dialyzed patients, new points of prophylaxis and treatment are sought. In recent years, more attention has been paid to the frequency and role of lipid disorders in children (7).
In the general population, the occurrence of MS is associated with obesity (8). In children and adolescents with CKD, overweight and obesity are less common, while other components of MS are frequent, and the postulated common pathomechanism in both groups is hyperinsulinism and insulin resistance. Various definitions are used to diagnose MS in children - some of them require the presence of obesity as the main pathomechanical factor (IDF), in others it is enough to meet any 3 or more of the 5 factors (9, 10). It remains an open question whether the metabolic syndrome itself plays a major role in increasing cardiovascular risk or whether this risk is related to the number of MS components or the severity of CKD.
In our study, we compared the associations of metabolic syndrome and the clustering of its components with target organ damage - LVH in children and adolescents with chronic kidney disease.
2 Materials and methodsThe prospective study was conducted between January 2016 and March 2017. The study was performed in accordance with the Declaration of Helsinki of 1975 for Human Research and approved by the Bioethical Committee of Jagiellonian University no. 122.6120.280.2015. The parents and patients were educated as to the objective and method of performing the study and gave their written informed consent.
2.1 SubjectsPatients aged 0-18 years with diagnosed chronic kidney disease were included. The exclusion criteria were lack of consent of the patient or parents, congenital heart defects or other primary heart diseases, acute infections during measurements, acute damage or failure of other organs.
2.2 Blood sampling and biochemical analysisBlood samples for basic research were taken on routine admission for diagnostic check-up in all patients (fasting for 12 hours). Biochemical analyses were performed and blood count, electrolytes, urea, creatinine, cystatin C, glucose, insulin, parathormone (PTH), venous blood gas, and lipids were measured. HOMA index was calculated. 24-hour urine collection with the albumin and protein concentrations were performed. Based on serum creatinine estimated glomerular filtration rate (eGFR) with the Schwartz (11) and Filler (12) formulas was calculated. Patients were divided into groups depending on CKD stage [group 1: CKD stage 1 + 2 (GFR≥ 60 ml/min/1.73m2), group 2: CKD stage 3 + 4 (GFR=15-59), group 3 - dialyzed children].
2.3 Metabolic syndrome definitionMetabolic Syndrome (MS) was diagnosed according to De Ferranti (DF) when ≥3 from the 5 following criteria were met: High glucose >110 mg/dl (6.1 mmol/l); Waist circumference >75 pc; triglycerides (TGL) >100 mg/dl (1.13 mmol/l); Low high density lipoprotein (HDL) ≤50 mg/dl (1.3 mmol/l); High blood pressure (BP)>90th pc (13).
2.4 Anthropometric and blood pressure measurementsAnthropometric measurements of patients such as weight, height and waist circumference were measured during each visit and body mass index (BMI) was calculated. Growth age was calculated. Ophthalmological examination with fundus assessment was done. Ambulatory blood pressure measurements (ABPM) with SpaceLabs 90207 device and cuff of appropriate size were performed. BP was measured every 20 minutes during the day and every 30 minutes during the night. Mean values of systolic (SBP), diastolic (DBP) and mean BP (mean arterial pressure - MAP) were calculated. Hypertension was defined as BP values equal to or exceeding the 95th percentile for gender, age and height. BMI and BP values were analyzed and expressed in standard deviations (SD).
2.5 EchocardiographyEchocardiographic examinations were performed by an experienced cardiologist using HP 5500 unit with S4 and S8 variable frequency probes. In children on chronic hemodialysis echocardiography was performed on the day between two hemodialysis procedures, while in children on peritoneal dialysis, it was performed during the daily exchange, with a low volume of dialysate in the peritoneal cavity. LV mass (LVM) was calculated using the formula described by Devereux and Reichek (14). LVM index (LVMI) was obtained by dividing LVM by height2.7 to normalize and linearize the relationship between LVM and height (15). LVH was defined as ≥95th percentile of LV mass index related to height and age. LVMI was also expressed as a z-score on the basis of age and sex (16).
2.6 Statistical analysisData were collected in MS Excel database and analyzed with Statistica 13 StatSoft. Clinical and biochemical parameters of CKD, LVH and MS as continuous or categorical variables were compared. Because data of the majority of variables did not show normal distribution, they are presented as median and interquartile range [IQR, 25th–75th percentile]. In statistical analysis nonparametric tests were used (MANOVA, Chi2, Kruskal-Wallis, U-Mann Whitney test). Univariate and multivariate regression for LVH were performed. A value of p <0.05 was considered significant in all statistical analyses.
A univariate regression analysis of risk factors for LVH was performed for every clinical and biochemical parameter with calculation of Odds ratio (OR), 95% Confidence Interval (CI), with significance p<0.05.
In a stepwise multiple logistic regression analysis (logit model) with LVH as dependent variable and all important multiple variables of clinical interest as predictors, including those with borderline p value of 0.05. Collinearity was excluded for any multivariable logistic regression covariates.
3 ResultsGroup of 71 children (28 girls, 43 boys) with CKD stage 1 to 5 was enrolled in the study. The patients’ median age was 14.05 (IQR:10.03-16.30) years and median eGFR based on serum creatinine (11) was 66.75 (32.76-92.32) ml/min/1.73m2.
Stage 1 CKD was observed in 18 (25.4%) patients; stage 2 in 23 (32.4%), stage 3 in 14 (19.7%), stage 4 in 5 (7%) patients. CKD stage 5 was diagnosed in 11 pts (15.5%).
Statistical analysis was performed in 3 defined groups according to eGFR value as follows:
≥60 ml/min/1.73m2 in 41 pts (57.7%); 15-59 ml/min/1.73m2 in 19 pts (26.8%) and <15 ml/min/1.73m2 in 11 pts (15.5%).
Clinical data and basic kidney function parameters depending on eGFR group are presented in Table 1.
Table 1 Characteristics of patients: Basic clinical parameters according to eGFR group.
Patients with eGFR <15 ml/min/1.73m2 (stage 5 CKD) had decreased hemoglobin [10.8 (9.5-12) vs 12.60 (11.80-15.00) vs 13.8 (13.5-14.6) g/dl, p<0.001] and increased phosphates [2.18 (1.35-2.76) vs 1.58 (1.30-1.60) vs 1.52 (1.42-1.70) mmol/l, p=0.002], albuminuria [87.5 (34.6-222) vs 53.4 (6.7-285.2) vs 5.75 (3.6-16.8) mg/24h, p=0.036], urine albumin/creatinine ratio [404.69 (108.91-523.08) vs 66.99 (5.08-233.53) vs 9.16 (3.32-28.22) mg/g, p=0.017], parathormone [258.2 (118.3-340.1) vs 48.1 (32.5-91.8) vs 18.4 (13.6-23.9) pg/ml, p<0.001] and calcium times phosphate product [63.29 (41.18-80.43) vs 47.41 (39.17-50.63) vs 45.83 (42.32-51.01), p=0.018] compared to pts with eGFR 15-59 and ≥60 ml/min/1.73m2, respectively (Supplementary Table 1). The frequency of other conditions according to eGFR is presented in Supplementary Table 2.
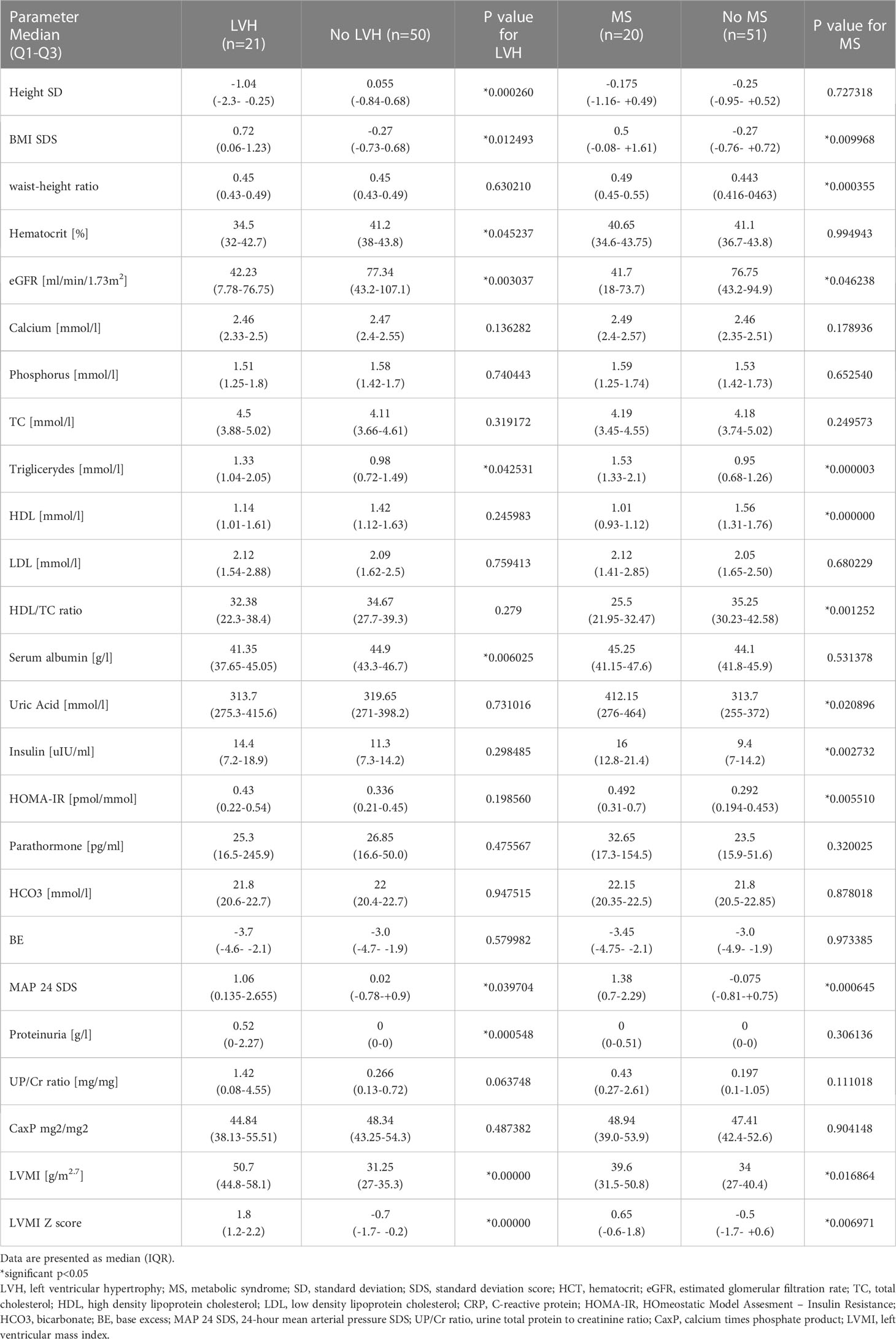
LVH was detected in 21 (29.6%) children. Patients with LVH had significantly higher BMI SDS (p=0.012), TGL level (p=0.04), proteinuria (p=0.0005), and MAP 24 SDS (p=0.04), and lower height SDS (p=0.00026) (Table 2).
Table 2 Important biochemical and clinical parameters in the study group in relations to left ventricular hypertrophy (LVH) and metabolic syndrome (MS).
MS (DF) was diagnosed in 20 pts (28.2%). High glucose ≥ 110 mg/dL was present in 3 pts (4.2%); Central obesity based on waist circumference >75th pc in 16 pts (22.5%); triglycerides > 100 mg/dL in 35 pts (49.3%); decreased high-density lipoprotein (HDL) ≤ 50mg/dL in 31 pts (43.7%) and high blood pressure > 90th pc in 29 pts (40.8%) were found, respectively. Hypertensive retinopathy (Ist degree) was present in 8 patients (11.3%).
In our study 13 pts (18.3%) were overweight (4 male, 9 female). Obesity was found in 4 pts (5.6%; 3 male, 1 female). All obese patients were diagnosed with MS. Among overweight children 8 out of 13 did not meet the criteria for the metabolic syndrome. In obese children 2 (50%) – 1 female and 1 male had LVH in echocardiography.
Patients with MS had lower eGFR, more pronounced lipid abnormalities, and increased uric acid, insulin, HOMA-IR, 24-hour mean arterial pressure and LVMI compared to those without (Table 2).
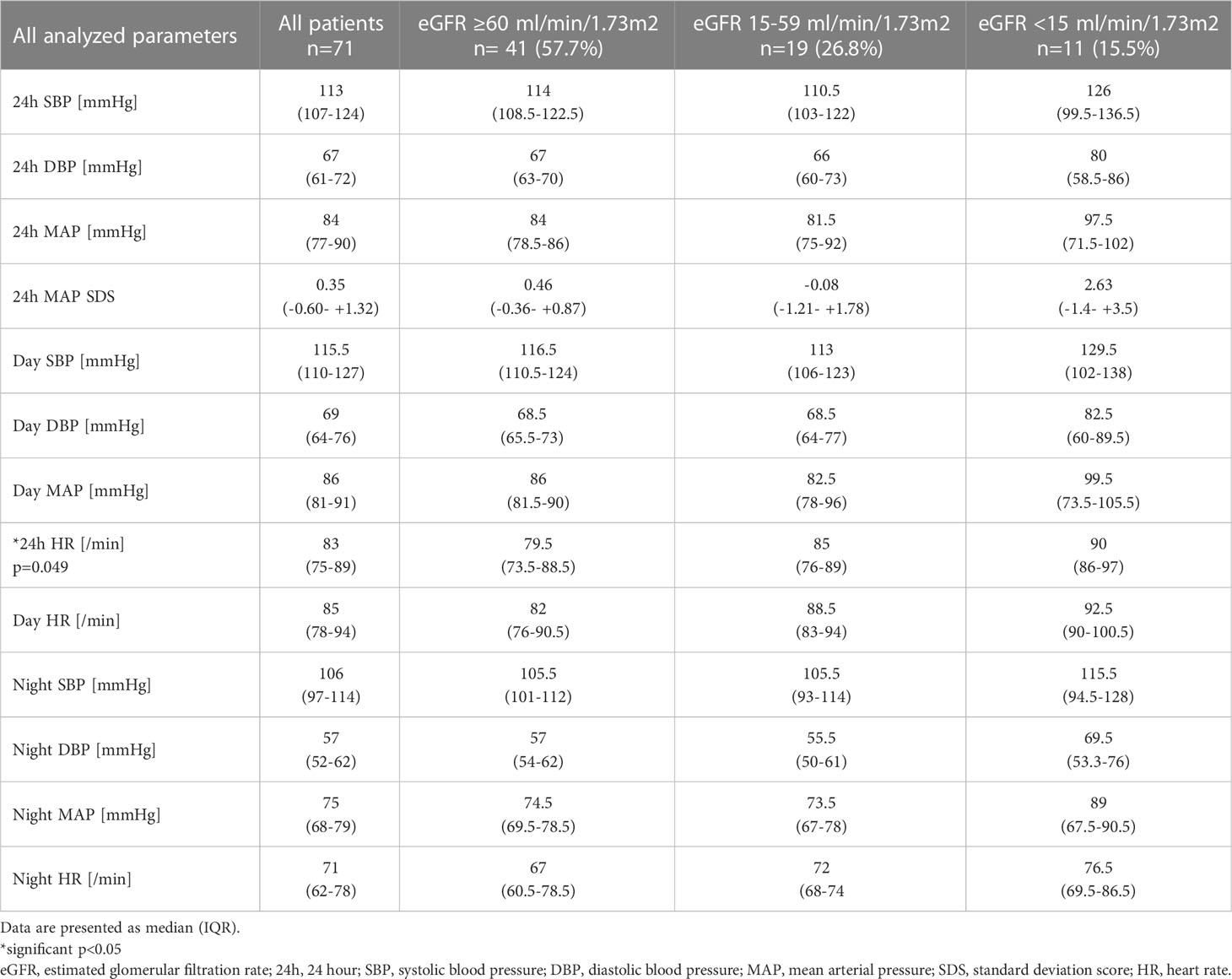
ABPM was performed in 62 patients. Due to young age ABPM was not used in 9 children. The analyzed parameters of arterial blood pressure and heart rate in the studied groups are provided in Table 3.
Table 3 Analyzed parameters of blood pressure and heart rate in the study groups.
LVH patients significantly more often presented with MS (48% vs 20%, p=0.018), as for low HDL-DF (62% vs 36%, p=0.045), high TGL-DF (67% vs 42%, p=0.0578 - borderline significance), presence of HT- DF (62% VS 32%, P=0.0193) or cluster of low HDL+ high TGL+HT (33.2% vs 12%, p=0.0339). In LVH patients CKD stage 5 occurred significantly more often (38% vs 0.06%, p=0.006).
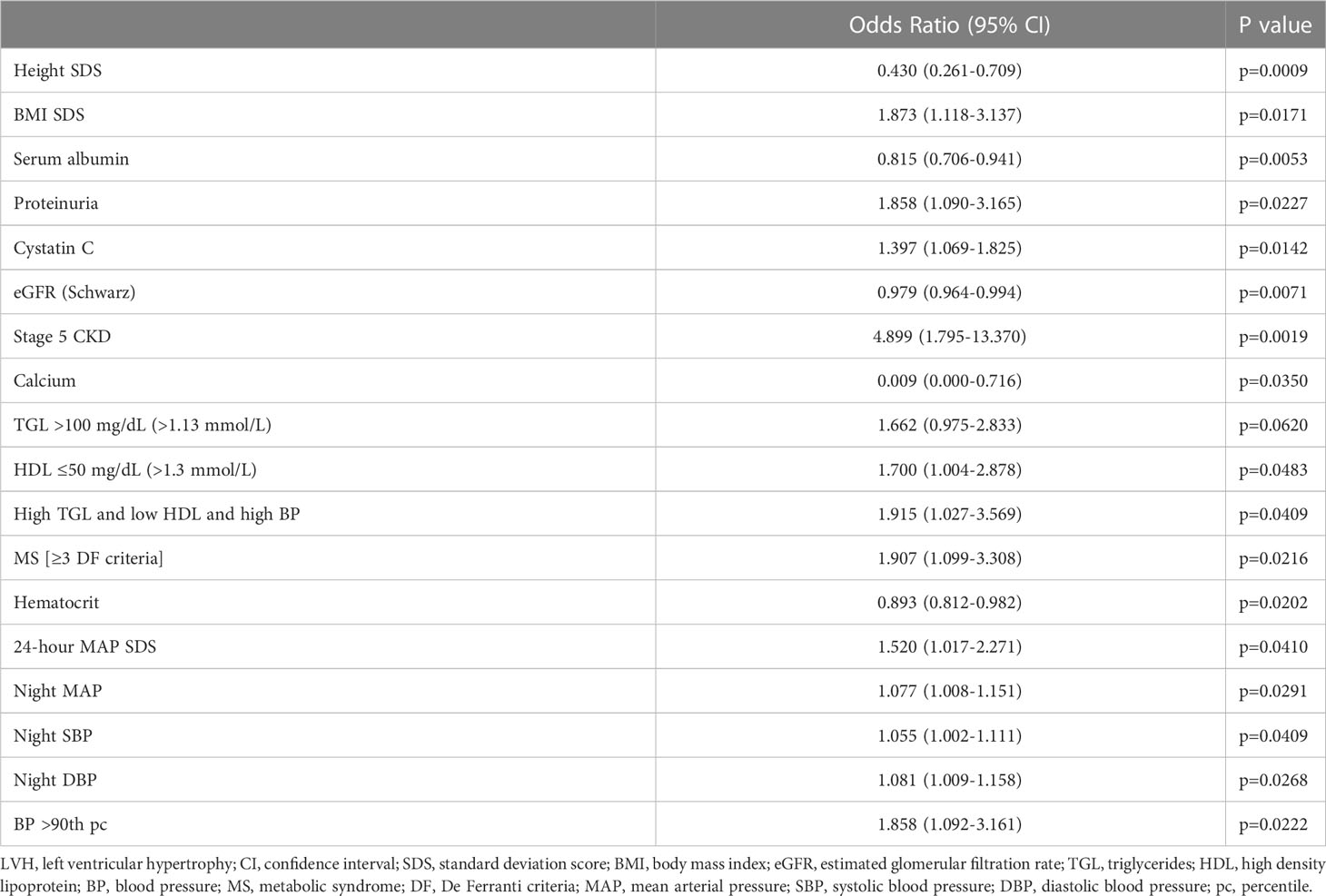
In univariate regression analysis the strongest risk factor for LVH was CKD stage 5 (OR 4.9, p=0.0019) and low height SDS (OR 0.43, p=0.0009). Among other LVH risk factors significant associations for diagnosis of MS according to DF (≥3 DF criteria; OR 1.91, p=0.0216), BMI SDS (OR 1.87, p=0.0171);, proteinuria (OR 1.86, p=0.0227), HDL ≤50 mg/dl/1.3 mmol/l (OR 1.70, p=0.0483) and 24-hour MAP SDS (OR 1.520, p=0.0410) were found (Table 4).
Table 4 Parameters significant for risk of LVH in univariate regression analysis.
In a stepwise multiple logistic regression analysis (logit model) of all important risk factors for LVH in CKD children, only three of them were statistically significant predictors (Table 5):
1. diagnosis of MS based on DF criteria (OR= 24.11; 95%CI 1.1-528.7; p=0.043; Chi2 = 8.38, p=0.0038);
2. high mean arterial pressure SDS (MAP SDS) in 24hABPM (OR=2.812; 95%CI 1.057-7.48; p=0.038; Chi2 = 5.91, p=0.015)
3. low height SDS (OR=0.078; 95%CI 0.013-0.486; p=0.006; Chi2 = 25.01, p<0.001).
Table 5 The significant risk factors for LVH in stepwise multiple logistic regression analysis (logit model).
The diagnosis of metabolic syndrome (DF criteria) increased 24 times the risk of left ventricular hypertrophy in CKD patients diagnosed with height deficit and high MAP in in 24 hours ambulatory blood pressure monitoring.
4 DiscussionIn the study population, metabolic syndrome was diagnosed based on the De Ferranti definition in as many as 28.2% of children with chronic kidney disease and LVH in 29.6%.
Cardiovascular risk factors defined as metabolic syndrome in children are most often associated with obesity. However, they can also occur in patients with CKD regardless of body weight. As such, they seem to be an important factor influencing myocardial remodeling and LVH. Left ventricular hypertrophy is an established cardiovascular risk factor and an important intermediate step in the cardiovascular continuum. Both obese children and CKD patients are at risk of developing LVH, which is confirmed by data from clinical trials. In obese children without hypertension, LVH was found in 47.2% and correlated with WHtR (17). In a large group of children from the Chronic Kidney Disease in Children study, higher BMI also significantly increased the risk of LVH (18). The high prevalence of overweight and obesity in the North American population should be emphasized - nearly one-third of children with CKD were overweight or obese. In the study population central obesity was found in 22.5%. In addition, children with CKD had increased prevalence of lipid disorders.
In an important, long-term study evaluating the impact of risk factors in childhood on cardiovascular complications in adults, it was shown that each of the 5 tested factors: BMI, systolic blood pressure, total cholesterol level, triglyceride level, and youth smoking significantly increased its risk. In addition, it should be emphasized that the change in the combined-risk z score between childhood and adulthood were associated with fatal and non-fatal cardiovascular events in midlife (19). This confirms the importance of the synergistic effect of various risk factors on the development of cardiovascular complications.
In the adult population, CKD significantly increases the risk of cardiovascular morbidity and mortality. In the pediatric population, this risk is also elevated, and LVH is found not only in children with end-stage renal disease, but also in the early stages of the disease (20, 21). Therefore, the importance of early diagnosis of LVH and early treatment should be emphasized.
In the present study a univariate analysis revealed that an eGFR below 15 was the strongest factor increasing the risk of LVH in children with CKD. Despite modern conservative treatment, children with eGFR <15 ml/min/1.73 m2 were characterized by severe metabolic disorders increasing the cardiovascular risk, such as anemia, elevated phosphate levels, CaxP product, proteinuria, albuminuria and increased heart rate in ABPM.
It is noteworthy that the simultaneous presence of lipid disorders in the form of high TGL and low HDL with hypertension increased the risk of LVH to a similar extent as MS (OR 1.915 vs 1.907). Among the single LVH risk factors: hypertension, BMI and proteinuria significantly correlated with an increase in left ventricular mass. The search for modifiable factors influencing the development of LVH is important for reducing the risk of cardiovascular morbidity. Data from clinical trials indicate the possibility of LVH regression, e.g. in the case of effective antihypertensive treatment (22). Numerous studies have confirmed the key role of hypertension in the development of LVH, both in the general population and in patients with impaired renal function (23). In the studied group of children with impaired renal function, as shown in a stepwise multiple logistic regression analysis, MS increased the risk of LVH up to 24 times. Although the LVMI assessment is commonly used to diagnose LVH in children with CKD based on indexing to height to the power of 2.7, other indices, e.g. LVM/height 2.16 + 0.09) have been proposed (24). Ruebner et al. drew attention to the need to use the LVM index to estimated lean body mass in children with CKD. In the studied population of 681 children, the authors found a higher incidence of LVH in girls with the use of LVMI (indexed to height) despite a lower number of cardiovascular risk factors. The use of the LVM/eLBM index leveled the differences in the frequency of LVH due to gender (25). Interestingly, a significant risk factor for LVH was short stature, increasing the risk by 12.8 times with a SD of -1. Because LVMI is indexed to height, LVMI was also expressed as a z-score on the basis of age and gender and presence of LVMI >95pc was analyzed. The dependence of LVH on growth retardation may result from the increased uremic toxemia in these patients and the influence of various compounds and their metabolites that accumulate in advanced renal failure. Adjustments or different formulas for LVH may be required for children with short stature due to chronic kidney disease (26). Potentially modifiable risk factors in CKD children which influence growth impairment and also play a role in the development of LVH could be focused on by clinicians to improve outcomes of their patients.
The most important limitations of the study is the small size of the group and the case-control study design. Furthermore, the lack of healthy controls is an additional limitation of the study.
5 ConclusionIn children with chronic kidney disease LVH is associated with the cluster of multiple factors, among them the components of MS, hypertension, stage 5 CKD and growth deficit were the most significant.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving human participants were reviewed and approved by Bioethical Committee of Jagiellonian University no. 122.6120.280.2015. Written informed consent to participate in this study was provided by the participants and their legal guardian/next of kin
Author contributionsThe study was designed by MD and DD. AR performed echocardiography. Data was collected by MD. MD and AM contributed to analysis and interpretation of data, or both. All authors contributed to the article and approved the submitted version.
FundingThe publication of this manuscript has been funded as part of the scientific and research activities of the Jagiellonian University Medical College.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1215527/full#supplementary-material
References2. Tunbridge MJ, Jardine AG. Cardiovascular complications of chronic kidney disease. Medicine (2019) 47(9):585–90. doi: 10.1016/j.mpmed.2019.06.014
CrossRef Full Text | Google Scholar
3. Wilson AC, Schneider MF, Cox C, Greenbaum LA, Saland J, White CT, et al. Prevalence and correlates of multiple cardiovascular risk factors in children with chronic kidney disease. Clin J Am Soc Nephrol (2011) 6(12):2759–65. doi: 10.2215/CJN.03010311
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Drożdż D, Kwinta P, Sztefko K, Kordon Z, Drożdż T, Łątka M, et al. Oxidative stress biomarkers and left ventricular hypertrophy in children with chronic kidney disease. Oxid Med Cell Longev (2016) 2016:7520231. doi: 10.1155/2016/7520231
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Brady TM, Schneider MF, Flynn JT, Cox C, Samuels J, Saland J, et al. Carotid intima-media thickness in children with CKD: results from the CKiD study. Clin J Am Soc Nephrol (2012) 7(12):1930–7. doi: 10.2215/CJN.03130312
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Sorof JM, Alexandrov AV, Cardwell G, Portman RJ. Carotid artery intimal-medial thickness and left ventricular hypertrophy in children with elevated blood pressure. Pediatrics (2003) 111(1):61–6. doi: 10.1542/peds.111.1.61
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Drozdz D, Alvarez-Pitti J, Wójcik M, Borghi C, Gabbianelli R, Mazur A, et al. Obesity and cardiometabolic risk factors: from childhood to adulthood. Nutrients (2021) 13(11):4176. doi: 10.3390/nu13114176
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med (2004) 350(23):2362–74. doi: 10.1056/NEJMoa031049
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Cruz ML, Goran MI. The metabolic syndrome in children and adolescents. Curr Diabetes Rep (2004) 4(1):53–62. doi: 10.1007/s11892-004-0012-x
CrossRef Full Text | Google Scholar
11. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol (2009) 20(3):629–37. doi: 10.1681/ASN.2008030287
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Filler G, Foster J, Acker A, Lepage N, Akbari A, Ehrich JH. The cockcroft-gault formula should not be used in children. Kidney Int (2005) 67(6):2321–4. doi: 10.1111/j.1523-1755.2005.00336.x
PubMed Abstract | CrossRef Full Text | Google Scholar
13. de Ferranti SD, Gauvreau K, Ludwig DS, Neufeld EJ, Newburger JW, Rifai N. Prevalence of the metabolic syndrome in American adolescents: findings from the third national health and nutrition examination survey. Circulation (2004) 110(16):2494–7. doi: 10.1161/01.CIR.0000145117.40114.C7
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man. Anatomic validation method. Circ (1977) 55(4):613–8. doi: 10.1161/01.cir.55.4.613
CrossRef Full Text | Google Scholar
15. de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, de Divitiis O, et al. Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweight. J Am Coll Cardiol (1992) 20(5):1251–60. doi: 10.1016/0735-1097(92)90385-z
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Khoury PR, Mitsnefes M, Daniels SR, Kimball TR. Age-specific reference intervals for indexed left ventricular mass in children. J Am Soc Echocardiogr (2009) 22(6):709–14. doi: 10.1016/j.echo.2009.03.003
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Giannisi F, Keivanidou A, Sakellari I, Balala S, Hassapidou M, Hitoglou-Makedou A, et al. Anthropometric and biochemical markers as possible indicators of left ventricular abnormal geometric pattern and function impairment in obese normotensive children. Diagnostics (Basel) (2020) 10(7):468. doi: 10.3390/diagnostics10070468
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Brady TM, Roem J, Cox C, Schneider MF, Wilson AC, Furth SL, et al. Adiposity, sex, and cardiovascular disease risk in children with CKD: a longitudinal study of youth enrolled in the chronic kidney disease in children (CKiD) study. Am J Kidney Dis (2020) 76(2):166–73. doi: 10.1053/j.ajkd.2020.01.011
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Jacobs DR Jr, Woo JG, Sinaiko AR, Daniels SR, Ikonen J, Juonala M, et al. Childhood cardiovascular risk factors and adult cardiovascular events. N Engl J Med (2022) 386(20):1877–88. doi: 10.1056/NEJMoa2109191
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Bakkaloglu SA, Borzych D, Soo Ha I, Serdaroglu E, Büscher R, Salas P, et al. Cardiac geometry in children receiving chronic peritoneal dialysis: findings from the international pediatric peritoneal dialysis network (IPPN) registry. Clin J Am Soc Nephrol (2011) 6(8):1926–33. doi: 10.2215/CJN.05990710
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Melhem N, Savis A, Wheatley A, Copeman H, Willmott K, Reid CJD, et al. Improved blood pressure and left ventricular remodelling in children on chronic intermittent haemodialysis: a longitudinal study. Pediatr Nephrol (2019) 34(10):1811–20. doi: 10.1007/s00467-019-04272-0
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Udine ML, Kaltman JR, Li Q, Liu J, Sun D, Cheung MC, et al. Effects of blood pressure percentile, body mass index, and race on left ventricular mass in children. Cardiol Young (2022) 32(6):855–60. doi: 10.1017/S1047951121004960
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Chinali M, Emma F, Esposito C, Rinelli G, Franceschini A, Doyon A, et al. Left ventricular mass indexing in infants, children, and adolescents: a simplified approach for the identification of left ventricular hypertrophy in clinical practice. J Pediatr (2016) 170:193–8. doi: 10.1016/j.jpeds.2015.10.085
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Ruebner RL, Ng D, Mitsnefes M, Foster BJ, Meyers K, Warady B, et al. Cardiovascular disease risk factors and left ventricular hypertrophy in girls and boys with CKD. Clin J Am Soc Nephrol (2016) 11(11):1962–8. doi: 10.2215/CJN.01270216
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Cho H, Choi HJ, Kang HG, Ha IS, Cheong HI, Han KH, et al. Influence of the method of definition on the prevalence of left-ventricular hypertrophy in children with chronic kidney disease: data from the know-ped CKD study. Kidney Blood Press Res (2017) 42(3):406–15. doi: 10.1159/000478867
留言 (0)