
記住我









Hypoparathyroidism is an abnormality of calcium metabolism characterized by low serum levels of parathyroid hormone leading to hypocalcemia. The most common cause of hypoparathyroidism in adults is postoperative hypoparathyroidism (1), which can lead to hypocalcemia. The symptoms of hypocalcemia can be subtle, such as perioral or digital paresthesia, muscle cramp, or anxiety, but sometimes, it results in serious or life-threatening symptoms such as tetany, cardiac arrhythmia, heart failure, and laryngospasm (2–4); all of these would impact the patient’s quality of life.
Multivariate analysis by various authors confirmed that extent of resection, such as total thyroidectomy (TT) and central-compartment (level VI) neck dissection (CND), is a major risk factor for both transient and permanent hypoparathyroidism after thyroid surgery (5–7). However, there are still some debates on postoperative hypoparathyroidism. Since the risks of postoperative hypoparathyroidism are high when surgeries are performed by low-volume surgeons (fewer than 50 cases/year) (8), can the risks decline when surgeries are performed by experienced surgeons? When conservative initial treatment leads to reoperation, is there a higher risk of postoperative hypoparathyroidism?
The objective of this retrospective analysis was to investigate the risk factors, discuss the prevention of hypoparathyroidism following thyroid surgery in patients with thyroid benign or malignant nodules, and explore permanent postoperative hypoparathyroidism evaluation (PPHE), which can forecast the risk of permanent postoperative hypoparathyroidism.
Materials and methodsPatient characteristicsThis retrospective analysis enrolled 2,903 patients with thyroid nodules who were admitted to the Sun Yat-Sen University Cancer Center and underwent thyroid surgery between October 2012 and August 2015. Intact parathyroid hormone (iPTH) and serum calcium (sCa) were assessed in all patients. iPTH (normal range, 15–65 pg/ml) was assessed using a commercially available iPTH assay (Elecsys 1010; Roche Diagnostics, Mannheim, Germany). sCa (normal range, 2.00–3.00 mmol/L) was measured on a conventional standard autoanalyzer. The diagnosis of hypoparathyroidism was established based on the iPTH and sCa on the morning of postoperative day 1 (12–24 hours postoperatively). Within this cohort, iPTH and sCa on the morning of postoperative day 1 of all patients were below the lower limit of the normal range. The patients were diagnosed with benign or malignant thyroid nodules. The patients with a diagnosis of primary parathyroid diseases or laryngeal cancer with thyroidectomy were excluded.
Patient data regarding the surgical procedure, the change in parathyroid function, and the management of hypoparathyroidism were reviewed. To patients with benign thyroid nodules >4 cm, lobectomy or total/near-total thyroidectomy was offered; to patients with malignant thyroid nodules, lobectomy/TT alone or lobectomy/TT with central-compartment (level VI) neck dissection was offered. Types of reoperation included lobectomy/TT alone, lobectomy/TT with CND, or unilateral/bilateral CND alone. All surgeries were performed by experienced surgeons with high-volume surgeries (more than 100 cases/year).
Long-term biochemical follow-up tests were performed 1, 6, and 12 months postoperatively. The diagnosis of permanent hypoparathyroidism required that features of hypoparathyroidism have persisted for at least 6 months after surgery (9).
Prophylactic intravenous calcium was routinely administered after bilateral thyroid surgery. Usually, 1 to 3 g of elemental calcium with active vitamin D3 and calcitriol orally divided was administered if the iPTH on the morning of postoperative day 1 was <15 pg/ml. The doses of calcium and active vitamin D3 would be increased when hypoparathyroid patients also had malabsorption syndrome. Calcium supplementation was stopped if the iPTH level exceeded 15 pg/ml no matter what the sCa level was.
Statistical analysesAll data were collected for statistical analysis using the SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). The unifactorial analysis of variance (ANOVA) and chi-square test were used to examine the difference between groups. The logistic regression analysis model was fitted for transient and permanent hypoparathyroidism. The level of significance was set at 0.05.
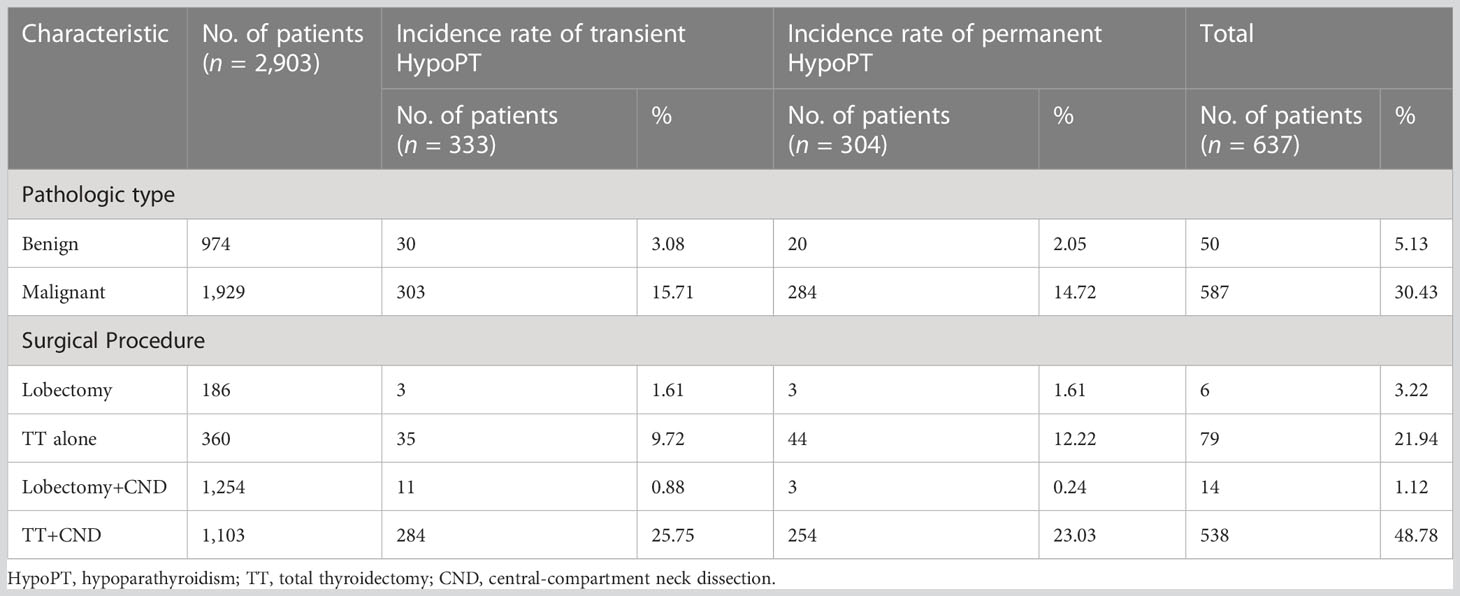
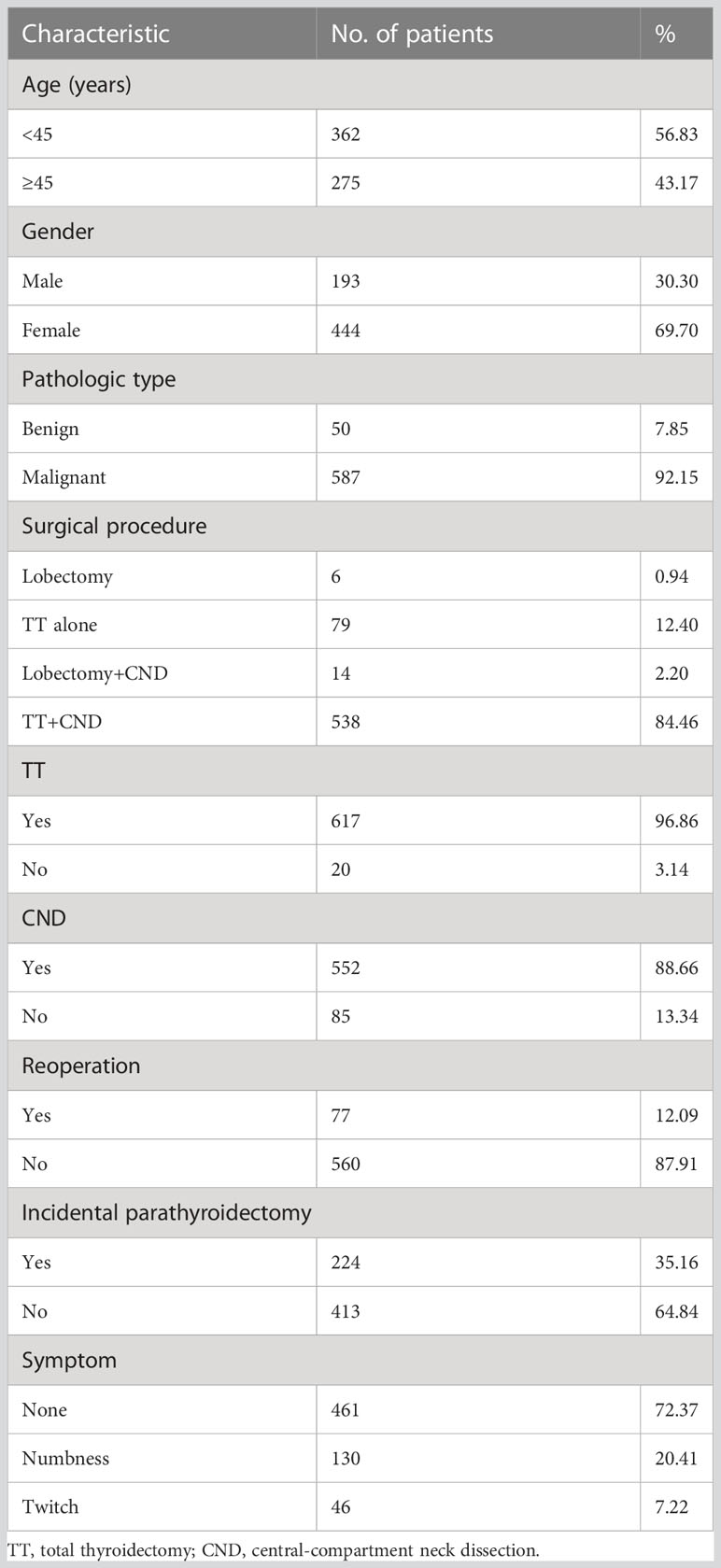
ResultsIncidence rate of postoperative hypoparathyroidismThis retrospective analysis enrolled 2,903 patients who had thyroid surgery. Within this cohort, 637 patients (mean age 42.5 years; range 9–82) developed postoperative hypoparathyroidism, and the incidence rate of postoperative hypoparathyroidism was 21.94% (637/2,903). A total of 333 patients developed transient hypoparathyroidism, and the incidence rate of transient hypoparathyroidism was 11.47% (333/2,903). In addition, 304 developed permanent hypoparathyroidism, and the incidence rate of permanent hypoparathyroidism was 10.47% (304/2,903). The incidence rates of postoperative hypoparathyroidism under the clinicopathological characteristics of patients who had thyroid surgery are summarized in Table 1. The differences between incidence rates of transient and permanent hypoparathyroidism under several pathologic types and surgical procedures were statistically significant (p < 0.001). The main characteristics of the patients with postoperative hypoparathyroidism are summarized in Table 2.
Table 1 The incidence rate of postoperative hypoparathyroidism under the clinicopathological characteristics of patients who had thyroid surgery (n = 2,903).
Table 2 Characteristics of patients with postoperative hypoparathyroidism (n = 637).
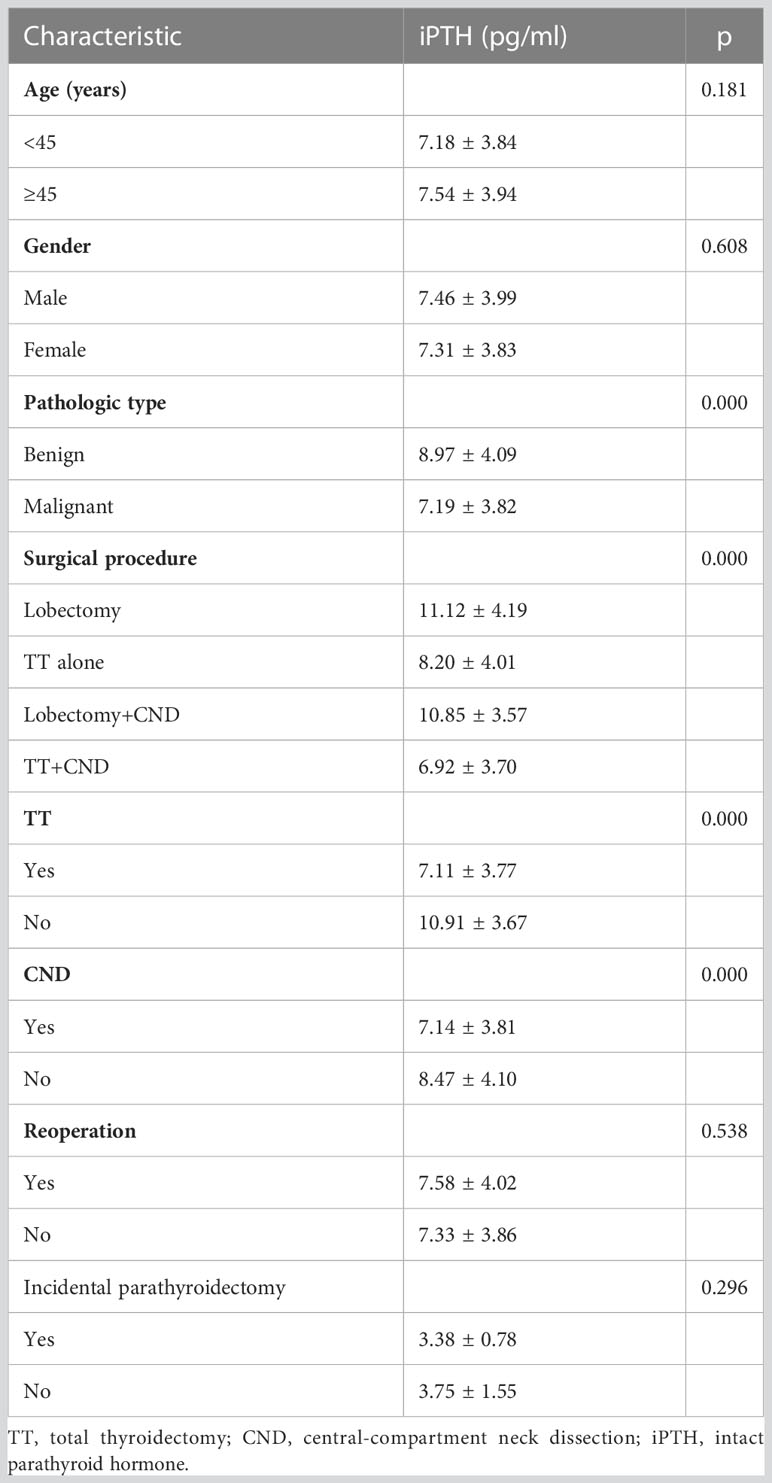
Measurement of iPTHiPTH on the morning of postoperative day 1 of all patients ranged from 1.20 to 14.98 pg/ml (mean ± SD, 7.34 ± 3.89 pg/ml). The differences in iPTH in various diagnoses and surgical procedures were statistically significant (p < 0.001). The iPTH was lower in patients with malignant thyroid nodules or who underwent TT and CND. The difference in iPTH between the TT+CND group and TT alone group was statistically significant (p = 0.001), but the difference was not statistically significant (p = 0.823) between the lobectomy+CND group and the lobectomy group. The study revealed that reoperation was not associated with iPTH (p = 0.538). The differences in iPTH under clinicopathological characteristics are summarized in Table 3.
Table 3 The difference in iPTH under their clinicopathological characteristics.
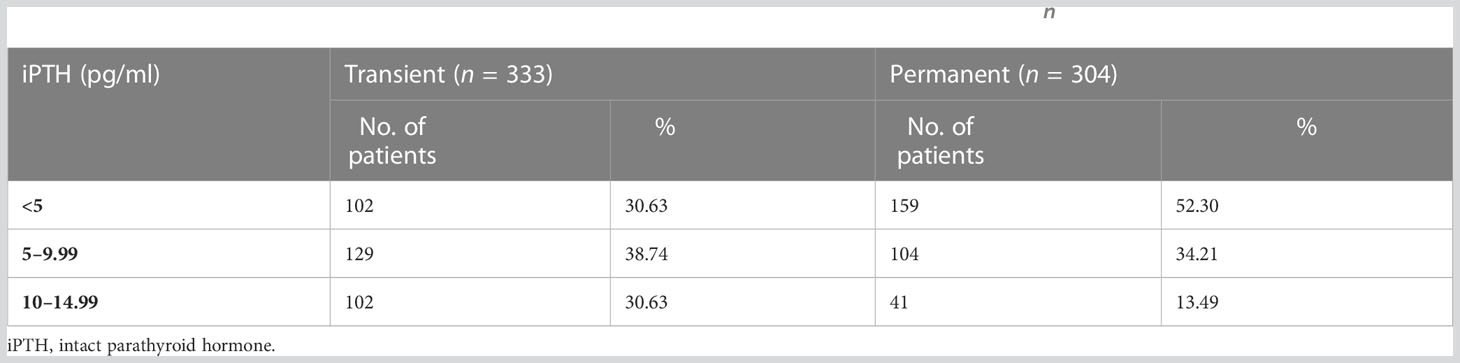
The difference in iPTH between transient hypoparathyroidism and permanent hypoparathyroidism was statistically significant (p < 0.001) on the morning of postoperative day 1. The iPTH was higher in patients whose parathyroid function returned to normal (8.34 ± 3.95 vs. 6.08 ± 3.39 pg/ml). The iPTH on the morning of postoperative day 1 of transient and permanent hypoparathyroidism is summarized in Table 4.
Table 4 The iPTH on the morning of postoperative day 1 of transient and permanent hypoparathyroidism (n = 637).
Measurement of sCaThe values of sCa ranged from 1.00 to 1.99 mmol/L (mean ± SD, 1.81 ± 0.17 mmol/L). Hypocalcemia led to numbness in the hands or feet of 130 patients (20.41%, 130/637) and twitching in the hands or feet of 46 patients (7.22%, 46/637), and 461 patients (72.37%, 461/637) had no signs and symptoms. The difference in sCa between patients with different symptoms was statistically significant (p < 0.001). The value of sCa was 1.80 ± 0.18 mmol/L in the no-symptom group, 1.77 ± 0.16 mmol/L in the numbness group, and 1.81 ± 0.15 mmol/L in the twitch group.
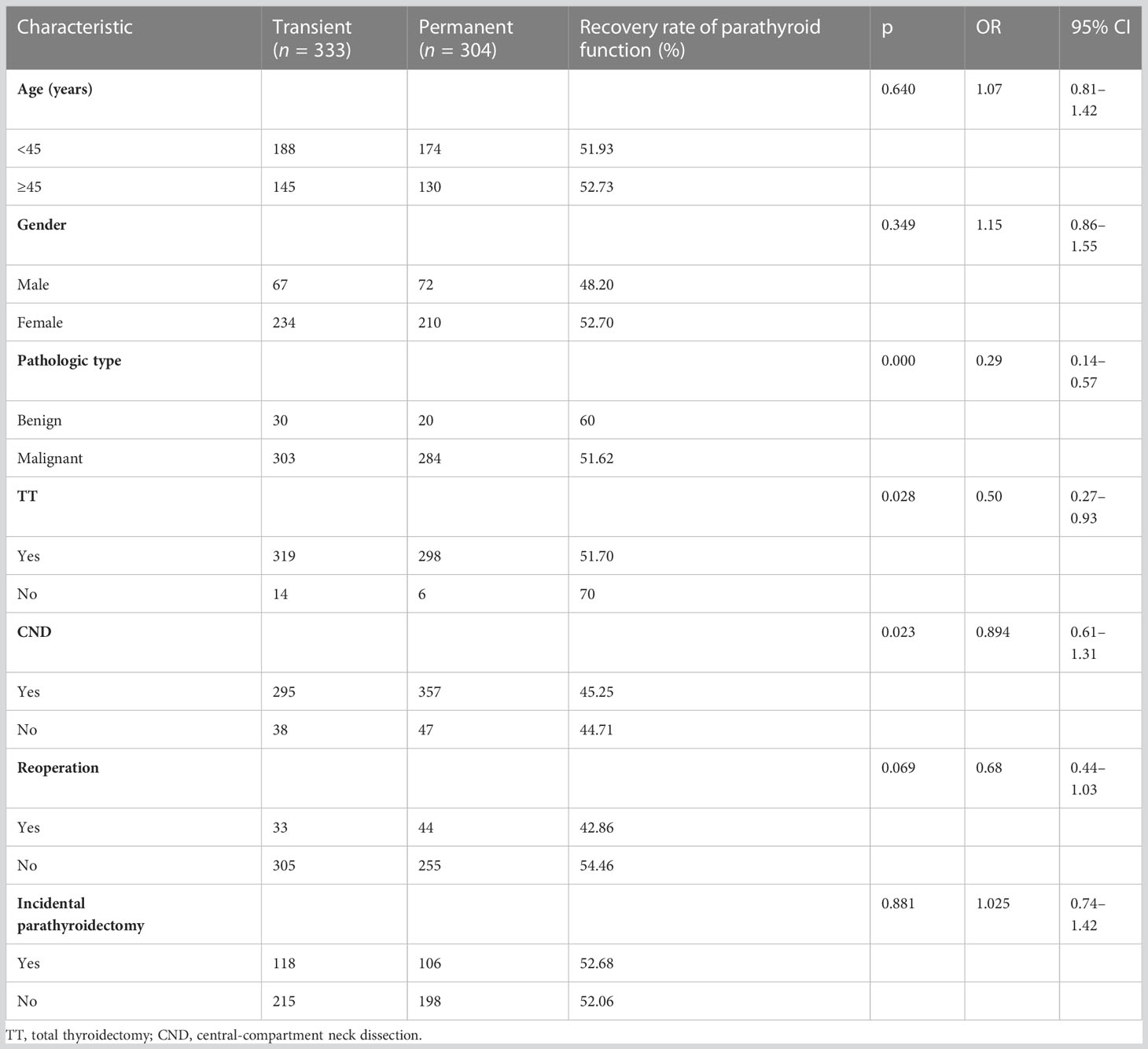
Recovery rate of parathyroid functionThe parathyroid function of 52.28% (333/637) patients was restored. In the logistic regression analysis model, the pathologic type (p = 0.000), TT (p = 0.026), and CND (p = 0.022) were independently associated with the recovery of parathyroid function. Patients who were diagnosed with malignant thyroid nodules or had undergone TT and CND had higher risks of developing permanent hypoparathyroidism than others. No association was observed in other factors including age, gender, reoperation, or incidental parathyroidectomy. The recovery rates of parathyroid function according to the clinicopathological characteristics of patients with postoperative hypoparathyroidism are summarized in Table 5.
Table 5 The recovery rate of parathyroid function under the clinicopathological characteristics of patients with postoperative hypoparathyroidism (n = 637).
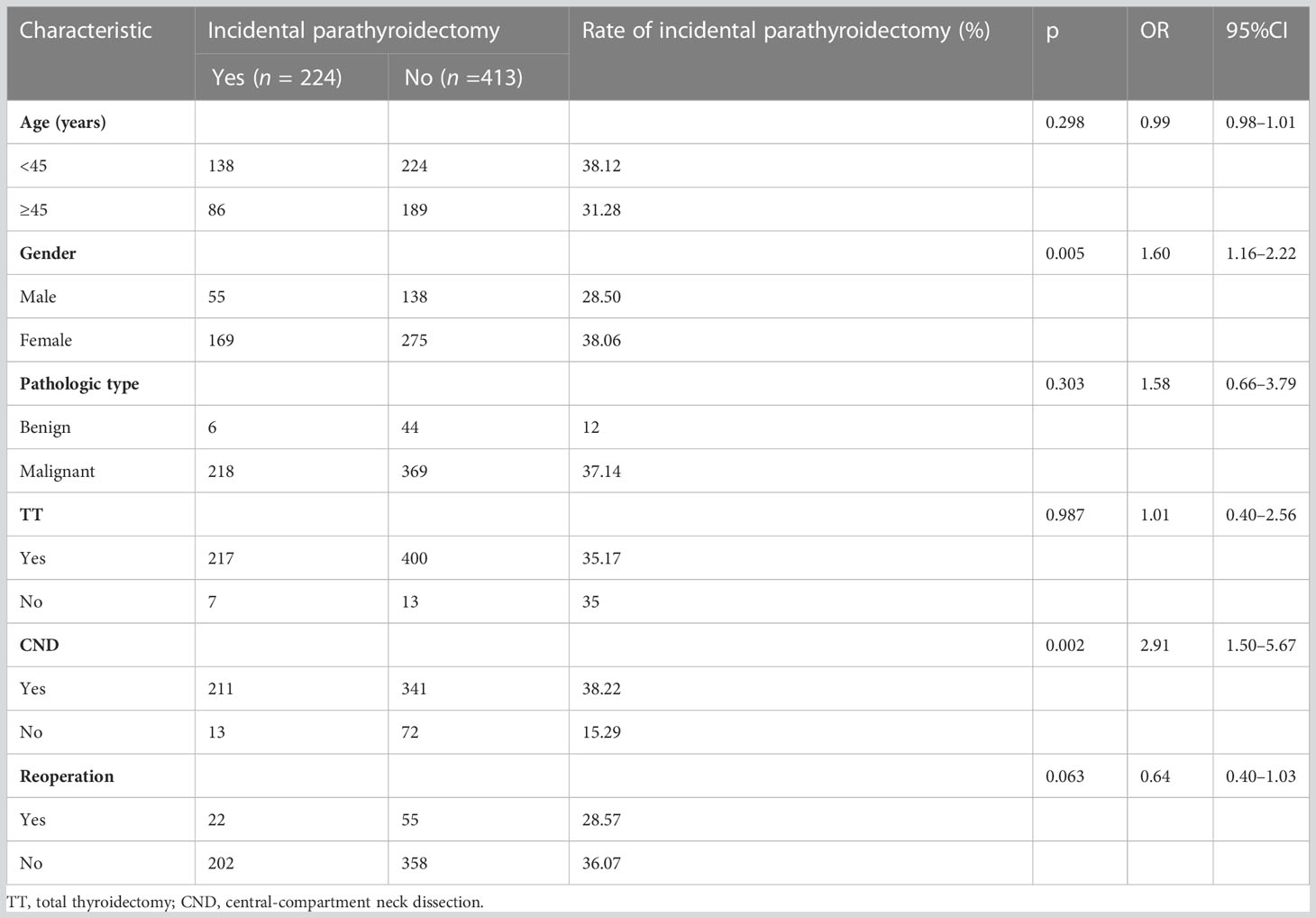
Rate of resection of parathyroidIt was confirmed that parathyroid glands in the thyroid gland and CND specimens were excised from 224 (35.16%, 224/637) patients with postoperative hypoparathyroidism by postoperative pathology. The rate of inadvertent parathyroid gland removal after a thyroid operation was 7.72% (224/2903). There was no correlation between the parathyroid gland removal and the recovery of parathyroid function independently (p = 0.881). In the logistic regression analysis model, gender (p = 0.005) and CND (p = 0.002) were independently associated with the resection of parathyroid. Female patients who underwent CND had a higher risk of resection of parathyroid than others. No associations were observed in other factors including age, pathologic type, TT, or reoperation. The rate of resection of parathyroid under the clinicopathological characteristics of patients with postoperative hypoparathyroidism is summarized in Table 6.
Table 6 The rate of incidental parathyroidectomy under the clinicopathological characteristics of patients with postoperative hypoparathyroidism (n = 637).
Permanent postoperative hypoparathyroidism evaluationThe PPHE was established on the risk factors and clinical practice. The iPTH, sCa, surgical procedure, reoperation, and pathologic type were selected as the reference indexes for PPHE. The scores of each reference index are shown as follows:
iPTH (pg/ml): = 1, = 2, = 3;
sCa (mmol/L): = 1, = 2, = 3;
Surgical procedure: = 1, = 2, = 3, = 4;
Reoperation: = 0, = 1;
Pathologic type: = 1, = 2.
The formula for PPHE is as follows: + + + + . The scoring system was developed, and we scored low, middle, and high risk of permanent postoperative hypoparathyroidism as 4–6, 7–9, and 10–13, respectively.
The scores for PPHE of all patients ranged from 4 to 13 (mean ± SD, 9.28 ± 1.64). The recovery rate of parathyroid function was 75% (18/24) in the low-risk group, 61.27% (193/315) in the middle-risk group, and 40.94% (122/298) in the high-risk group. The differences in the recovery rates of parathyroid function in distinct risk groups were statistically significant (p < 0.001).
DiscussionPostoperative hypoparathyroidism caused by temporarily “disturbed” parathyroid metabolism is a clinically relevant complication that can occur after thyroid surgery. It usually is due to inadvertent or unavoidable removal of or damage to the parathyroid glands and/or their blood supply. Earlier reports had suggested that after thyroid surgery, transient hypoparathyroidism range from 6.9% to 53.6% (10–13), and permanent hypoparathyroidism range from 0.4% to 33% (5, 12, 14–16). In our study, the incidence rate of transient hypoparathyroidism was 11.47%, and the incidence rate of permanent hypoparathyroidism was 10.47%.
Pathologic type and postoperative hypoparathyroidismOf the 637 patients with postoperative hypoparathyroidism, 92.15% were diagnosed with malignant thyroid nodules. However, the patients were treated in local clinics instead of our center when they were diagnosed with benign thyroid nodules. These may be the main reason for the low constituent ratio of benign thyroid nodules to malignant ones in our study.
Surgical procedure and postoperative hypoparathyroidismBilateral thyroid surgery is a major risk factor for both transient and permanent hypoparathyroidism (5–7). The results of our study were consistent with the findings of others. The iPTH on the morning of postoperative day 1 and recovery rate of parathyroid function were lower than in patients with unilateral (lobectomy ± CND) thyroid surgery. These can be explained by the fact that bilateral thyroid surgery may increase the risk of traumatic or ischemic damage to parathyroid glands caused by surgical manipulation on both sides (17). However, postoperative hypoparathyroidism after unilateral thyroid surgery had little been reported in the literature. The incidence rates of transient and permanent hypoparathyroidism of unilateral thyroid surgery were 0.97% (14/1440) and 0.42% (6/1440), respectively. In the 20 patients with unilateral thyroid surgery, the iPTH of six patients was under 10 pg/ml. This may be because some people only have two parathyroid glands.
The role of central-compartment neck dissection in the treatment of cN0 papillary thyroid carcinoma is debatable. It has been repeatedly emphasized that the procedure increases the risk of parathyroid-related complications, with rates of permanent hypoparathyroidism of 4%–11% (18–21). As previously reported, rates of transient hypoparathyroidism were also higher in patients who had CND compared to patients who had TT alone (21–27). In our cohort, the difference in iPTH between the TT+CND group and TT alone group was statistically significant (p = 0.001), and undergoing CND in the same period was independently associated with the recovery of parathyroid function (p = 0.023, OR = 0.894) and the resection of parathyroid (p = 0.002, OR = 2.91). It also may be because that normal parathyroid tissue has an appearance similar to that of enlarged lymph nodes, and another reason may be due to injury of vascular pedicles when parathyroid glands share the same blood supply as the thyroid (28).
Reoperation and postoperative hypoparathyroidismPatients who have undergone primary surgery for either benign or malignant disease may subsequently be indicated for a further thyroid procedure. Removal of all or part of the gland at the primary procedure leads to gross anatomical disruption. Further disruption results from postoperative tissue change through fibrosis and scarring (29). Combined, these effects may account for the higher rates of complications seen in previous case series of reoperative thyroid surgery (30–34). However, the difference between the primary surgery group and the reoperation group was not statistically significant within our cohort. It may be because patients have sufficient time to recover their blood supply to the parathyroid gland by collateral regeneration of the vessels from relatively undamaged surrounding tissues and scar tissue of the previous surgery, and the parathyroid gland may be more resistant to ischemic injury in a reoperative procedure even though fibrotic scar tissue makes sharp dissection difficult.
Prevention of hypoparathyroidismIn our study, the rate of resection of parathyroid was only 35.16% (224/637) in the patients with postoperative hypoparathyroidism. The other two-thirds of postoperative hypoparathyroidism might be due to damage to the blood supply of parathyroid glands. Identification and preservation of the parathyroid glands in situ and avoidance of injury to their vascular pedicles were key factors in managing hypoparathyroidism. Rapid intraoperative parathyroid hormone (rIO-PTH) assay levels were used to identify parathyroids as a parameter in thyroid surgery (35, 36). Carbon nanoparticles (CNs) can be injected as a suspension (China Food and Drug Administration approval H20041829; Lai Mei Pharmaceutical Co., Chongqing, China) that can enter the lymphatic capillaries. After the injection of CN suspension into thyroid parenchyma, the CNs will penetrate and diffuse the whole thyroid lobe, enter the lymphatic vessels rapidly, accumulate in the lymph, and stain them back thereby. However, the parathyroid glands have no lymph–vessel connections to the thyroid to be stained black. CN suspension injection has been applied recently to help identify parathyroids during thyroid surgery (37–40). Angiography with the fluorescent dye indocyanine green (ICG) was performed to visualize the vascularization of identified parathyroid glands (41). Every effort must thus be made to preserve vascular supply to the superior parathyroid gland. However, it is often difficult to do so for the inferior parathyroid gland, as it is more prone to ischemic injury during CND.
Under the premise that it was confirmed on intraoperative frozen-section pathology to avoid autograft of a lymph node metastasis, any parathyroid gland that looks likely to be totally devascularized can be removed during the operation and autotransplanted into well-vascularized muscles such as the sternocleidomastoid muscle or the forearm muscles (42). The thyroid gland and CND specimens excised should also be examined carefully to discover any inadvertently removed parathyroid glands, and these should be autotransplanted (43).
Permanent postoperative hypoparathyroidism evaluationIt is a very significant topic in clinical research to evaluate the surgical risk level of patients objectively. Glasgow coma scale (GCS), acute physiology and chronic health evaluation II (APACHE II), and physiological and operative score for the enumeration of mortality and morbidity (POSSUM) are widely used in the prognosis evaluation of surgical patients. However, there are few scoring models for the incidence of postoperative complications in patients with thyroid nodules.
According to the results of multivariate analysis, we established the risk function of permanent postoperative hypoparathyroidism and used the ROC curve test to evaluate the efficacy. The area under the ROC curve was 0.7, and the efficacy evaluation was moderate. We thought that it might be limited to evaluating permanent postoperative hypoparathyroidism only by risk factors. Therefore, according to the characteristics of thyroid surgery, combined with the results of multivariate analysis and clinical practice, iPTH, sCa, surgical procedure, reoperation, and pathologic type were selected as the reference indexes for PPHE. We distributed the score into the low, middle, and high risks to evaluate permanent postoperative hypoparathyroidism. The differences in the recovery rates of parathyroid function in distinct risk groups were statistically significant (p < 0.001).
PPHE can forecast the risk of permanent postoperative hypoparathyroidism well. According to it, the patients can be monitored and treated individually, which has important clinical application value. Prospective studies that are multicenter and larger are required to continuously improve PPHE.
ConclusionsIn conclusion, hypoparathyroidism occurs due to thyroid surgery, especially in patients with malignant thyroid nodules. In patients with bilateral thyroid surgery and CND in the same period, there are more postoperative hypoparathyroidism and more resection of the parathyroid. The reoperation for recurrence is not associated with hypoparathyroidism. Identification and preservation of the parathyroid glands in situ and avoidance of injury to their vascular pedicles are key factors in managing hypoparathyroidism. PPHE can forecast the risk of permanent postoperative hypoparathyroidism well.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statementEthical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients was not required to participate in this study in accordance with national legislation and institutional requirements.
Author contributionsXW performed the methodology, data analysis, and writing. SW performed the formal analysis and writing. YC and ZG performed the validation. CL and WH performed the project administration. All authors contributed to the article and approved the submitted version.
FundingThis work was supported by the National Natural Science Foundation of China, No. 82071024.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1182062/full#supplementary-material
References3. Patil NJ, Yadav SS, Gokhale YA, Padwa N. Primary hypoparathyroidism: psychosis in postpartum period. J Assoc Physicians India (2010) 58:506–8.
PubMed Abstract | Google Scholar
4. Ilveskoski E, Sclarovsky S, Nikus K. Severe hypocalcemia simulating ST-elevation myocardial infarction. Am J Emerg Med (2012) 30:3–6. doi: 10.1016/j.ajem.2010.10.021
CrossRef Full Text | Google Scholar
5. Wingert DO, Friesen SR, Iliopoulos JI, Pierce GE, Thomas JH, Hermreck AS. Post-thyroidectomy hypocalcemia. Incidence and risk factors. Am J Surg (1986) 152(6):606–10. doi: 10.1016/0002-9610(86)90435-6
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Mc Henry C, Speroff T, Wintworth D, Murphy T. Risk factors for postthyroidectomy hypocalcemia. Surgery (1994) 116:641–8.
PubMed Abstract | Google Scholar
7. Thomusch O, Machens A, Sekulla C, Ukkat J, Lippert H, Gastinger I, et al. Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg (2000) 24:1335–41. doi: 10.1007/s002680010221
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Percival RC, Hargreaves AW, Kanis JA. The mechanism of hypocalcemia following thyroidectomy. Acta Endocrinol (1985) 109:220–6.
12. Falk SA, Birken EA, Baran DT. Temporary postthyroidectomy hypocalcemia. Arch Otolaryngol Head Neck Surg (1998) 114:168–74. doi: 10.1001/archotol.1988.01860140066023
CrossRef Full Text | Google Scholar
13. Bilezikian JP, Khan A, Potts JT Jr, Brandi ML, Clarke BL, Shoback D, et al. Hypoparathyroidism in the adult: epidemiology, diagnosis, pathophysiology, target-organ involvement, treatment, and challenges for future research. Bone Miner Res (2011) 26:2317–37. doi: 10.1002/jbmr.483
CrossRef Full Text | Google Scholar
14. Thompson NW, Harness JK. Complications of total thyroidectomy for carcinoma. Surg Gynecol Obstet (1970) 131:861–8.
PubMed Abstract | Google Scholar
17. Promberger R, Ott J, Kober F, Karik M, Freissmuth M, Hermann M. Normal parathyroid hormone levels do not exclude permanent hypoparathyroidism after thyroidectomy. Thyroid (2011) 21:145–50. doi: 10.1089/thy.2010.0067
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Henry JF, Gramatica L, Denizot A, Kvachenyuk A, Puccini M, Defechereux T. Morbidity of prophylactic lymph node dissection in the central neck area in patients with papillary thyroid carcinomas. Langenbecks Arch Surg (1998) 383:167–9. doi: 10.1007/s004230050111
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Pereira JA, Jimeno J, Miquel J, Iglesias M, Munné A, Sancho JJ, et al. Nodal yield, morbidity, and recurrence after central neck dissection for papillary thyroid carcinoma. Surgery (2005) 138:1095–101. doi: 10.1016/j.surg.2005.09.013
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K, et al. Clinical significance of metastasis to the central compartment from papillary microcarcinoma of the thyroid. World J Surg (2006) 30:91–9. doi: 10.1007/s00268-005-0113-y
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Roh JL, Park JY, Park CI. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastasis, morbidity, recurrence,and postoperative levels of serum parathyroid hormone. Ann Surg (2007) 245:604–10. doi: 10.1097/01.sla.0000250451.59685.67
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Palestini N, Borasi A, Cestino L, Freddi M, Odasso C, Robecchi A. Is central neck dissection a safe procedure in the treatment of papillary thyroid cancer? our experience. Langenbecks Arch Surg (2008) 393:693–8. doi: 10.1007/s00423-008-0360-0
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Mazzaferri EL, Doherty GM, Steward DL. The pros and cons of prophylactic central compartment lymph node dissection for papillary thyroid carcinoma. Thyroid (2009) 19:683–9. doi: 10.1089/thy.2009.1578
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Moo TA, McGill J, Allendorf J, Lee J, Fahey T 3rd, Zarnegar R. Impact of prophylactic central neck lymph node dissection on early recurrence in papillary thyroid carcinoma. World J Surg (2010) 34:1187–91. doi: 10.1007/s00268-010-0418-3
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Iyer NG, Shaha AR. Central compartment dissection for well differentiated thyroid cancer and the band plays on. Curr Opin Otolaryngol Head Neck Surg (2011) 19:106–12. doi: 10.1097/MOO.0b013e328343af58
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Giordano D, Valcavi R, Thompson GB, Pedroni C, Renna L, Gradoni P, et al. Complications of central neck dissection in patients with papillary thyroid carcinoma: results of a study on 1087 patients and review of the literature. Thyroid (2012) 22:911–7. doi: 10.1089/thy.2012.0011
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Shen WT, Ogawa L, Ruan D, Suh I, Kebebew E, Duh QY, et al. Central neck lymph node dissection for papillary thyroid cancer: comparison of complication and recurrence rates in 295 initial dissections and reoperations. Arch Surg (2010) 145:272–5. doi: 10.1001/archsurg.2010.9
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Levin KE, Clark OH, Duh QY, Demeure M, Siperstein AE, Clark OH. Reoperative thyroid surgery. Surgery (1992) 111:604–9.
PubMed Abstract | Google Scholar
32. Menegaux F, Turpin G, Dahman M, Leenhardt L, Chadarevian R, Aurengo A, et al. Secondary thyroidectomy in patients with prior thyroid surgery for benign disease: a study of 203 cases. Surgery (1999) 126:479–83. doi: 10.1016/S0039-6060(99)70088-7
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Kim JH, Chung MK, Son Y-I. Reliable early prediction for different types of post-thyroidectomy hypocalcemia. Clin Exp Otorhinolaryngol (2011) 4:95–100. doi: 10.3342/ceo.2011.4.2.95
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Bian XH, Li SJ, Zhou L, Zhang CH, Zhang G, Fu YT, et al. Applicability of rapid intraoperative parathyroid hormone assay through fine needle aspiration to identify parathyroid tissue in thyroid surgery. Exp Ther Med (2016) 12(6):4072–6. doi: 10.3892/etm.2016.3896
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Ezzat WF, Fathey H, Fawaz S, El-Ashri A, Youssef T, Othman HB. Intraoperative parathyroid hormone as an indicator for parathyroid gland preservation in thyroid surgery. Swiss Med Wkly. (2011) 141:w13299. doi: 10.4414/smw.2011.13299
PubMed Abstract | CrossRef Full Text | Google Scholar
37. Bin W, Zhi-Peng D, Nian-Cun Q, Liu ME, Liu S, Jiang DZ, et al. Application of carbon nanoparticles accelerates the rapid recovery of parathyroid function during thyroid carcinoma surgery with central lymph node dissection: a retrospective cohort study. Int J Surg (2016) 36:164–9. doi: 10.1016/j.ijsu.2016.10.037
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Long M, Luo D, Diao F, Huang M, Huang KK, Peng X, et al. A carbon nanoparticle lymphatic tracer protected parathyroid glands during radical thyroidectomy for papillary thyroid non-microcarcinoma. Surg Innov (2017) 24(1):29–34. doi: 10.1177/1553350616668088
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Gao B, Tian W, Jiang Y, Zhang S, Guo L, Zhao J, et al. Application of carbon nanoparticles for parathyroid protection in reoperation of thyroid diseases. Int J Clin Exp Med (2015) 8(12):22254–61.
PubMed Abstract | Google Scholar
40. Huang K, Luo D, Huang M, Long M, Peng X, Li H. Protection of parathyroid function using carbon nanoparticles during thyroid surgery. Otolaryngol Head Neck Surg (2013) 149(6):845–50. doi: 10.1177/0194599813509779
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Vidal FJ, Belfontali V, Sadowski SM, Karenovics W, Guigard S, Triponez F. Parathyroid gland angiography with indocyanine green fluorescence to predict parathyroid function after thyroid surgery. Br J Surg (2016) 103(5):537–43. doi: 10.1002/bjs.10101
PubMed Abstract | CrossRef Full Text | Google Scholar
43. Abboud B, Sleilaty G, Braidy C, Zeineddine S, Ghorra C, Abadjian G, et al. Careful examination of thyroid specimen intraoperatively to reduce incidence of inadvertent parathyroidectomy during thyroid surgery. Arch Otolaryngol Head Neck Surg (2007) 133(11):1105–10. doi: 10.1001/archotol.133.11.1105
留言 (0)