
記住我
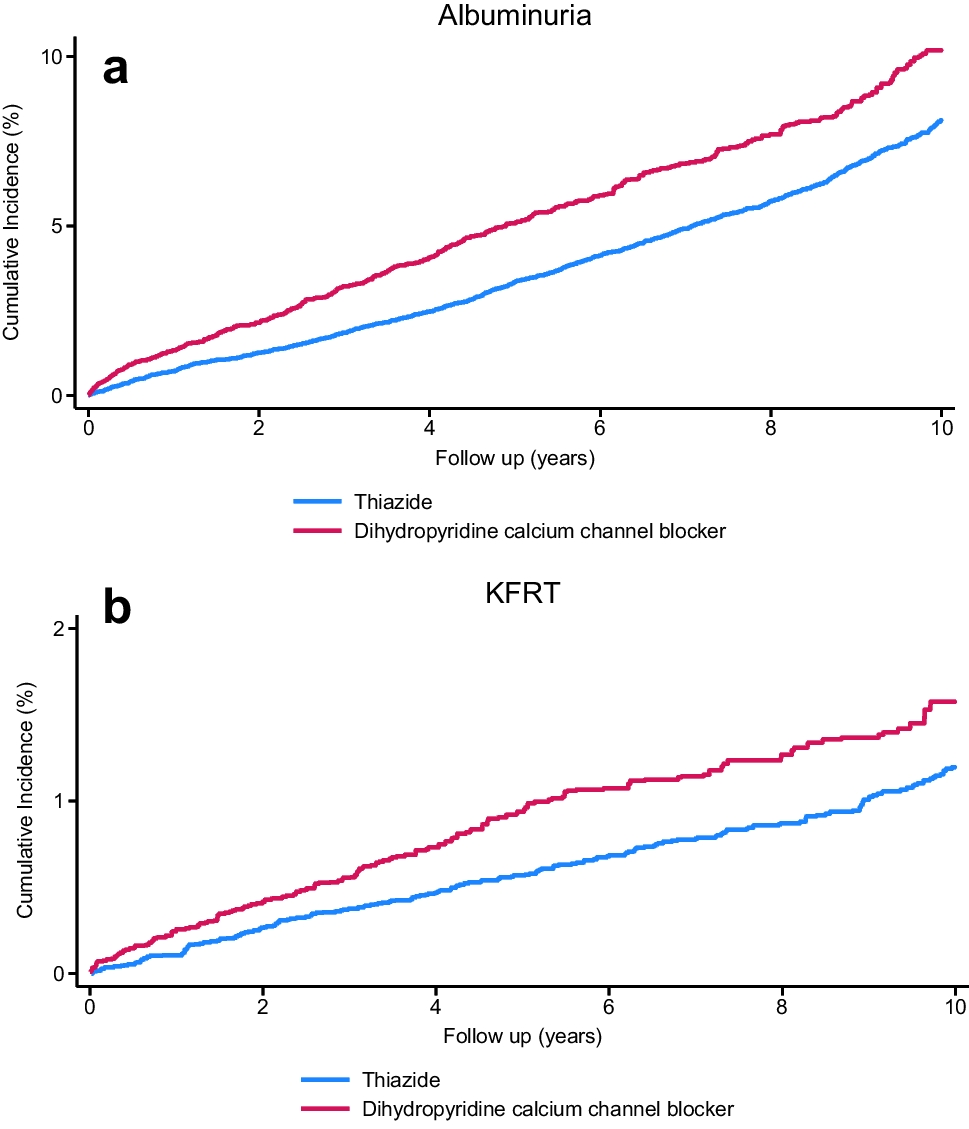



Semi-structured interviews were conducted with twenty-one individuals (Table 1). Participants were predominantly male (65.0%) with a mean age of 51.0 years (standard deviation 10.4 years). Participants were involved in the process of accepting or declining inter-hospital patient transfers at fifteen hospitals, representing 45.5% of the 33 eligible hospitals contacted to participate in the state (Table 2). Twenty percent of participating hospitals are in rural areas, defined by the 2019 American Hospital Association Annual Survey17. A third (33.3%) serve a patient population consisting of greater than 20% Medicaid-insured patients.
Table 1 Characteristics of Decision-makers Involved in Inter-hospital Transfer Decision-makingTable 2 Characteristics of Michigan Level I and Level II Trauma Center Hospitals by Participant Inclusion Using 2019 American Hospital Association DataWe identified three domains of factors impacting transfer decision-making: decision-maker factors, patient factors, and environmental factors (Fig. 1). Domains were organized based on an existing framework of ICU admission triage23. We compared our findings to this existing ICU triage framework and expanded upon the framework to describe the impact of triage on the decision-maker. Participants described substantial moral distress related to the decision-making process, defined as the experience of wanting to do what one believes to be right but being constrained from doing so26.
Fig. 1
Patient transfer decision-making framework.
Decision-maker FactorsDecision-maker Professional BackgroundEleven participants were physicians primarily responsible for making final transfer acceptance decisions based on patient factors. Physician participants were from Emergency Medicine, Critical Care Medicine, and Internal Medicine/Hospital Medicine. About half (45.5%) of physicians held administrative roles to oversee transfer acceptances as part of a multidisciplinary team and more commonly considered hospital capacity when making decisions. Nurses working on transfer teams communicated with other healthcare workers requesting to transfer patients and were involved in information-gathering, initial triaging, and coordinating transfers. For example, nurses were involved in declining transfers due to limited capacity and discouraging family-initiated transfers. Non-clinician administrators were involved in overseeing teams managing transfer intake and collaborated with physicians to make final decisions. Many participants noted a switch in their usual roles during the pandemic. New responsibilities included dedicated transfer triage roles as opposed to having transfer triage responsibilities along with clinical care duties.
Lack of Guidance for Transfer Decision-makingParticipants were not aware of any guidelines outside their institution or system for how to approach transfers. As one participant remarked, “if something was out there that would help guide us in how to best approach transfer process in a pandemic…I think that information would be crucial to the success of providing patients with quality healthcare” (participant (P) 11). Decision-makers sought support from their colleagues. A participant described how they would “talk with [their] partners in the office…talk with our managers…and sometimes our hospitalist team is super amazing because you’ll call them and say, ‘Help me out here. Let’s talk about these two cases. What do you see or what do you think?’” (P6). Another participant discussing their hospital’s future plans for developing guidelines and creating an interdisciplinary team to make transfer decisions remarked: “…just people feeling more comfortable about the decisions that are made, ‘cause that’s hard for the supervisors right now, to make that decision on their own” (P5). Participants were unaware of any state, national, or professional recommendations for the transfer triage process and often sought support from colleagues.
Patient FactorsPatient Preferences for Medical CarePatient preferences to avoid escalation of medical care such as intubation and mechanical ventilation impacted transfer decisions. One participant recalled how patient preferences factored into their decision to decline a patient transfer request: “We’ve had a couple of patients that were do not resuscitate, do not intubate…well, there’s no reason for us to move that person. Just be supportive care [sic] and hopefully they’ll get better at that location” (P8).
Severity of IllnessTransfer requests for more severely ill patients were prioritized over patients with less severe illness. One participant described how their hospital was a “safety net for a lot of small rural hospitals to send their sickest patients…we’re picking and choosing the sickest of the bunch to come in” (P20). Patients with a higher severity of illness were more likely to be accepted for transfer.
Predicted Chance of SurvivalDecision-making was often based on the expected chance of patient survival with escalated medical care. Patients estimated to have a higher likelihood of survival based on age or comorbidities were prioritized for transfer. For example, a participant described how “we might have 10 [hospitals] that are calling to transfer a patient for possible ECMO for COVID…how do we decide?…We decide, based on data, we know younger patients do better. So the younger you are, the more likely you are to come in”. (P1). Another participant explained: “If you have a 500 pound patient with very bad diabetes, unvaccinated, lymphedema, coronary artery disease, CKD [chronic kidney disease], versus having a 26 year old, no past medical history, who has just single organ failure on the ventilator…you want to choose that person that has the highest chance of surviving…I’m gonna choose the 26 year old patient based on the fact that most likely this is the person that will make it” (P19). Participants considered a patient’s likelihood of survival with continued medical care when triaging patient transfer requests.
Need for Specialized Medical CarePatients who required specialty care were prioritized for transfer. Participants described acceptance of patients requiring specific medical interventions including acute stroke management, trauma services, extracorporeal membrane oxygenation (ECMO), and interventional cardiology services. For example, a participant described how their hospital had multiple “hospitals that routinely send [them] their stroke patients for a thrombectomy, and so they were always sort of a high priority for us…keeping a critical care bed open that could ensure that we served those patients, was definitely important” (P13). Patients requiring specialized medical intervention were preferentially accepted for transfer.
Interaction of Patient FactorsMost commonly, individuals described that an identified need for specialty care and patient severity of illness took precedence over other patient factors when triaging transfers. Assessing likelihood of survival frequently often arose in the context of transfer for ECMO consideration. When specific patient preferences including those to forego resuscitation were known, they appeared to impact decisions more broadly and carried more weight than other factors. We did not find explicit examples of healthcare insurance or other financial concerns impacting transfer acceptance at the level of the decision-maker. Additionally, patient and family requests for transfer did not often influence transfer decision-making. One participant commented that they were “filtering out the family requests and the patient requests…because those are just a request, it’s not a clinical picture if they need to be transferred” (P3).
Environmental FactorsImpact of Scarcity on Transfer AcceptancePatient transfer decisions were made within the context of environmental factors at the decision-maker’s hospital. All participants described capacity strain at their hospital impacting transfer acceptance at the time of the interview. For example, one participant noted how “the volume [of transfer requests] is much higher now, and I think that’s specifically ‘cause every hospital is full, pretty much across the state of Michigan, so it’s hard to find beds, so even our ICU and Critical Care Units are pretty much at capacity every day now, and actually our hospital system has been pretty much at or over capacity every single day” (P4). Scarce medical resources at participants’ hospitals frequently prevented patient transfers. Participants cited a lack of nurses; one explained how “there have been times where we have physical beds, but there’s not the nursing professionals available to care for the patients who would be laying (sic) on those beds” (P21). Lack of ward and intensive care unit space, as well as a shortage of ECMO circuits, also precluded transfers. As one participant questioned, “six or seven institutions [are] calling daily about an ECMO bed, and then one opens up, how do we make that decision of who gets that circuit potentially?” (P16). Scarce medical resources impacting patient transfer acceptance included clinical staff, hospital space, and medical equipment.
Restructuring of Transfer ProcessMost participants described changes to the transfer process related to the increased frequency of transfer requests during the pandemic. Some hospital networks created centralized transfer centers while others developed new transfer center roles, such as a dedicated “physician triage officer to make clinical [transfer] decisions” (P15). Hospital workers sometimes described using a multi-disciplinary approach. One participant explained their role as a “triage officer, like adding that additional voice, along with the receiving provider and the transfer center nurse, the hope is that I’m alleviating some of the moral distress they face, just because I’m really coming more at it from a capacity piece” (P16). Increased transfer requests also prompted the development of hospital-specific clinical criteria to inform triage decisions. One decision-maker explained how they would not accept patients for transfer with COVID-19 infection unless they exceeded a certain oxygen requirement threshold. They shared, “we were setting just sort of a generic oxygen requirement” as a prerequisite for transfer (P17).
Participants employed different strategies to support hospitals requesting patient transfers when transfers were not feasible. Hospital systems increased use of virtual support at community regional hospitals to provide advice when patient transfers were not feasible. For example, one participant described how their hospital assisted another hospital with managing a stroke remotely through the hospital’s “telestroke and tele-neurology program” (P20). Another described how their hospital’s tele-ICU facilitated triage of transfers: “we do a ton of telephone and peer-to-peer support …rather than transferring the patient to the main center ICU, we’ve been able to expand our ICU capacity in our smaller hospitals by providing a virtual ICU coverage” (P16).
Characteristics of Requesting HospitalsFactors outside the receiving hospital affected transfer decision-making, including requesting hospital specialty care availability, capacity, and hospital affiliation. For example, transfers were prioritized from hospitals with limited specialty care with one participant explaining “our teams really bend over backward because we recognize a resource…one bed for us is a lot different than one bed for those smaller facilities” (P8). Hospitals requesting transfer due to capacity constraints were variably considered, as one participant described “one [reason for transfer] would be technical expertise or procedural expertise, the other one was pure staffing shortages…or [the requesting hospital’s] bed availability” (P7). Transfers from affiliated hospitals were highly prioritized. One participant remarked, “we have had to remain relatively closed to non-affiliated hospitals” (P10).
Moral DistressDecision-makers frequently described considerable moral distress associated with the burden of choosing which patients to accept from a long list of transfer requests. When faced with the decision to choose between two critically ill patients, one participant asked, “how do you decide between two young healthy women? It’s just impossible, it’s impossible. It’s just impossible” (P1). Another described how to approach multiple extracorporeal membrane oxygenation (ECMO) transfers, explaining “this is a moral dilemma…how do you decide which ECMO patient you take?” (P2). Participants described frustration and exhaustion related to transfer decision-making. As one participant said, “it’s exhausting. It’s extremely stressful. I’ve…never experienced anything quite like this, frustrating, all of those things” (P18). Eighteen participants (85.7%) described the experience of moral distress associated with transfer decision-making.
Declining all transfers when hospital capacity was limited was a source of moral distress described by participants. One participant recalled that declining transfers was “frustrating…because it’s an uncomfortable and sort of new situation to not be able to help [other hospitals]” (P21). Another recalled, “I don’t want anybody to ever think that any of us don’t want to do what’s right for all of the patients, ‘cause we really do…We wanna do what’s right, but we know that inside these four walls, people are struggling as well” (P5). One healthcare worker described being unable to accept a severely ill patient “like a car crash in slow motion,” proceeding to explain “to know that one of your colleagues is in distress and their patient’s in distress, and all you can do is try to use what you have available to try and change their situation for them, and sometimes you literally can’t do anything” (P17).
Comparing Triage FrameworksMultiple factors impacting inter-hospital transfer decision-making were similar to those considered during ICU triage. Participants identified severity of illness, patient treatment limitations, and expected prognosis as key patient factors impacting transfer decision-making. These factors are also considered when making ICU triage decisions. However, key differences were identified between transfer decision-making about all adult patients during this pandemic surge and the existing ICU triage model in the context of severe resource strain. For example, environmental factors were considered less important than patient factors in the ICU triage framework, whereas resource constraints for both requesting and receiving hospitals were much more salient among our participants. While bed availability was the major environmental constraint identified in both ICU triage and transfer decision-making, our participants additionally noted staff shortages and medical equipment shortages (such as ECMO circuits). Lastly, participants described substantial moral distress related to decision-making. The emotional impact of decision-making is not described in the ICU triage framework.
留言 (0)