Linea alba hernias are rare in Japan. Less than 100 cases have been reported since Kumagaya et al. first reported it in 1923 [1]. The etiology of linea alba hernias is likely multifactorial. It may include (i) a congenitally weak portion of the linea alba; (ii) increased intra-abdominal pressure due to obesity, pregnancy, or ascites; (iii) pre-peritoneal fat tissue causing a defect in the linea alba; (iv) anatomical variants of the abdominal wall musculature; and (v) trauma [2, 3].
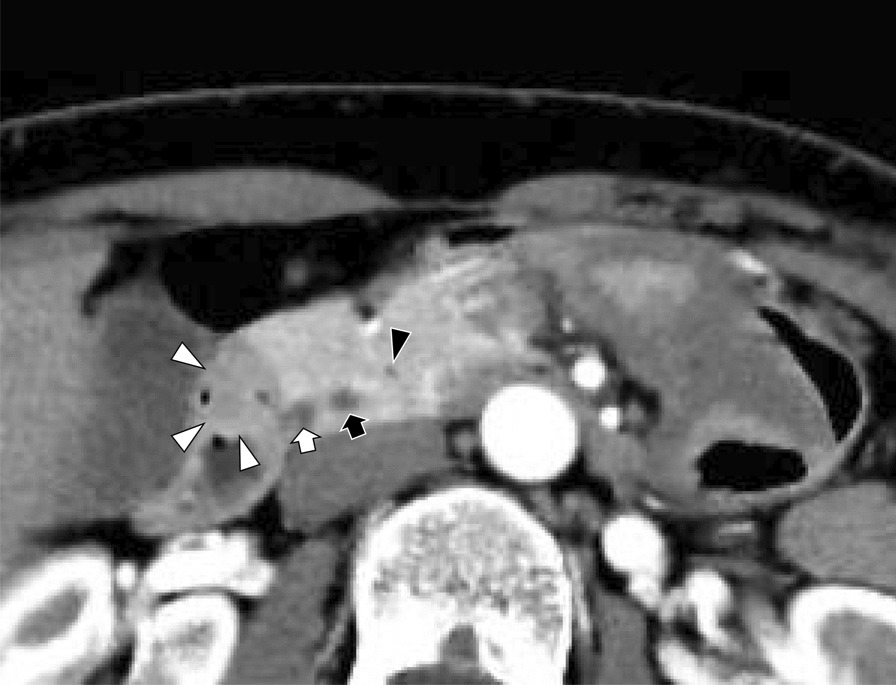
The patient exhibited mild obesity with a BMI of 26.3 kg/m2. She had a history of a single pregnancy and delivery, without a history of trauma. Intraoperatively, the hernia’s development was considered to be primarily due to the abnormal proliferation of pre-peritoneal adipose tissue and resultant defect in the linea alba, rather than obesity or pregnancy history. Linea alba hernias contain the pre-peritoneal fat, omentum, and small intestine in 30.6% of cases, colon in 11.8%, stomach in 7.1%, and falciform ligament in 2.4% [4]. Multiple hernial orifices have been reported in approximately 20% of patients with linea alba hernias [5]. To our best knowledge, among linea alba hernias, there are few cases of hernias involving the hepatic round ligament.
Linea alba hernias in the upper abdominal region are sometimes classified as epigastric hernias. We searched PubMed using the terms “linea alba hernia”, “epigastric hernia”, “hepatic round ligament, and “fibrolipoma”, and identified no publications with those terms. To our best knowledge, except for our case, we found no cases of fibrolipoma of the hepatic round ligament with herniated content in linea alba hernias.
In Japan, there have been nine cases [4, 6,7,8,9,10,11,12] in which the hernia contents included the hepatic round ligament, including our case (Table 1); the average age was 68.4 years and eight patients were female. The average size of the hernial orifice was 19.4 mm. Four patients underwent open repair, and five underwent laparoscopic repair. Repaired with mesh in four cases and without mesh in five cases, hernia was not reported to recur in any of the cases.
Table 1 Cases of linea alba hernia caused by hepatic round ligamentLaparoscopic surgery necessitated the insertion of at least two ports, with one serving as a camera port. Because the patient was not in the postoperative phase and CT imaging suggested the unlikelihood of presence of multiple hernia sacs, intra-abdominal observation using a laparoscope was deemed superfluous. Single-port laparoscopic surgery in linea alba hernia has become reported in recent years [10]. There are some limitations to single-port laparoscopic surgery, such as reduced instrument mobility, it has been shown that single-port laparoscopic surgery group had a lower rate of postoperative complications, higher rate of intraoperative complications rather than conventional laparoscopic surgery group in colorectal surgery [13]. Single-port laparoscopy was deemed a viable alternative, if the institution possessed proficient practitioners in the technique, specifically for linea alba hernias. However, the author’s lack of familiarity with single-port laparoscopy for linea alba hernias precluded its use in this instance. Consequently, open surgical repair was selected because the experience gained from treating abdominal incisional hernias and similar conditions can be applied.
Regarding the use of mesh in abdominal wall hernias, there have been reports of significantly fewer recurrences with the use of mesh than with simple suture closure in cases of small hernia orifices of less than 20 mm [14]. Based on this evidence, we elected to incorporate mesh during the closure procedure. A meta-analysis between the laparoscopic and open groups for abdominal wall hernias found no significant difference in recurrence between the two groups [15].
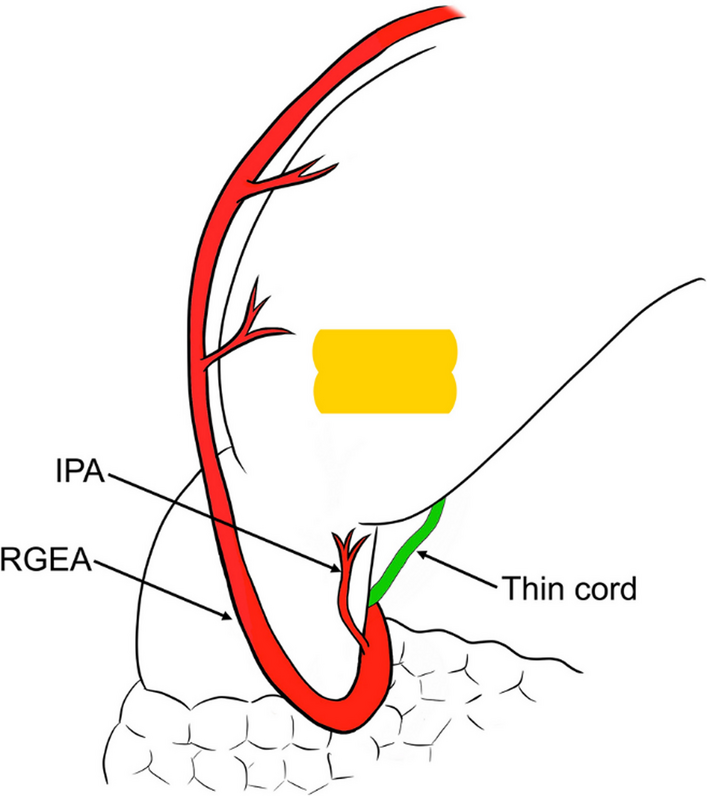
Among the primary tumors of the hepatic round ligament, there are several reported cases of tumors such as cystic lymphangioma [16], fibroma [17, 18], hemangioendothelioma [19], hepatocellular carcinoma [20], leiomyoma [21], leiomyosarcoma [22], and liposarcoma [23]. Since tumor is often malignant, its resection, including the round hepatic ligament, is preferred. In this case, considering the possibility of malignancy, the tumor, including the round hepatic ligament, was resected. The specimen was pathologically diagnosed as a fibrolipoma of the hepatic round ligament.
If a tumor of the hepatic round ligament is noted intraoperatively, resection of the hepatic round ligament is considered necessary, and a pathological diagnosis of the specimen is required.









留言 (0)