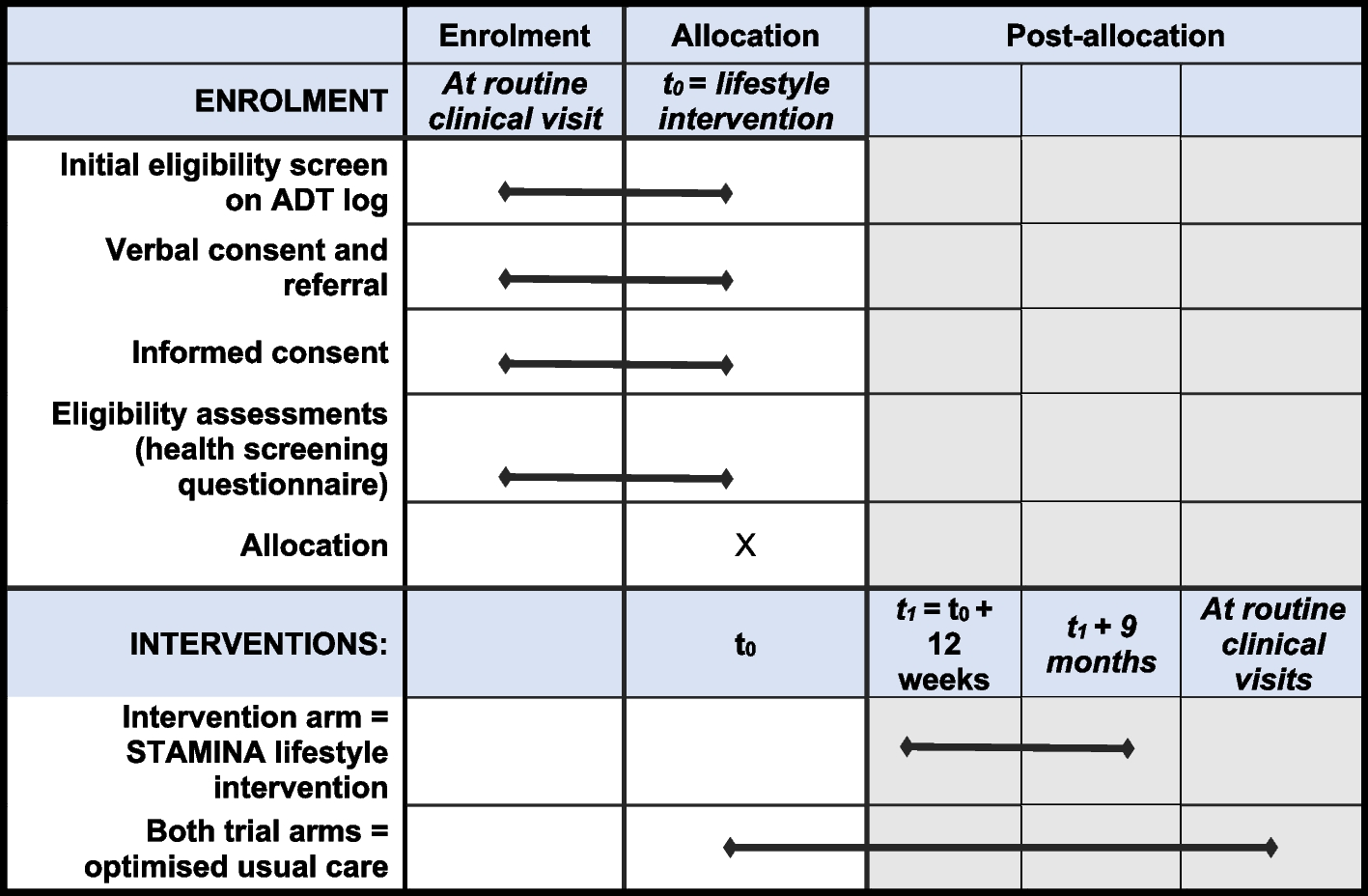
An overview of the primary and secondary outcomes, descriptive data and timing of assessment is displayed in Table 1.
Table 1 Assessment schedulePrimary outcomes
The primary outcomes are the differences in the number of subjects that will lose at least 50% of excess weight, as well as the number of subjects that will have glycated haemoglobin levels lower than 5.7%, between the probiotic and placebo groups, 1 year after the surgery. The rationale behind the primary outcomes is based on previous studies that have described the effect of Hafnia alvei HA4597™. In the preclinical study conducted by Legrand et al. [14], the effect of Hafnia alvei HA4597™ supplementation was assessed in two models of obesity, in leptin deficiency ob/ob mice and high-fat diet (HFD)-fed obese and overweight mice. Results showed that in both models’ body weight gain was significantly lower by the end of the study (50.1% ob/ob and 38.1% HFD), as well as fat gain (38.3% ob/ob and 51.9% HFD) [14]. In addition, loss of lean mass was 126.8% lower and food intake reduced 20.8% in the ob/ob mice [14]. A second trial was conducted by Lucas et al. [11] using a mice model of obesity characterized by a combination of a HFD-fed obese and a genetic ob/ob mice which closely represents the hyperphagia and diet-induced obesity in humans (compulsive eating behaviour combined with hypercaloric diet and functional leptin resistance). The authors observed that Hafnia alvei HA4597™ supplementation resulted in 58.1% lower body weight gain, decreased food intake and fat mass gain, and increased lean mass preservation, resulting in an improved lean/fat mass ratio [11]. Moreover, Hafnia alvei HA4597™ treatment also improved metabolic outcomes, including glycemia. Basal glucose levels decreased by 1.5-fold compared to standard diet HFD-fed controls [11]. Afterwards, the efficacy of Hafnia alvei HA4597™ supplementation was tested in humans [15]. A randomized, placebo-controlled, double-blind trial evaluated the effect of this probiotic (5 × 107 CFU of Hafnia alvei HA4597™) on 236 overweight men and women that were following a low-calorie diet [15]. After 12 weeks, significantly more subjects (+ 51%) lost at least 4% of their initial weight comparing to placebo [15]. Furthermore, compared to placebo, subjects in the treatment group had a significant reduction in hip circumference and glycemia, and increased feeling of fullness, which was assessed by a visual analogue scale [15].
Thus, preclinical and clinical results with Hafnia alvei HA4597™ are very promising in regard to weight loss and glycaemic levels reduction. Therefore, these outcomes are crucial to validate the effect of Hafnia alvei HA4597™ supplementation in an obese population and assess its contribution to the success of bariatric surgery.
Secondary outcomes
As secondary outcomes, the impact of Hafnia alvei HA4597™ supplementation will be assessed towards changes in gut microbiota composition, including diversity, richness, and characterization of microbes at phylum, class, order, family, genus, and species level at baseline, and 3, 6, 9, and 12 months. Alterations in the metabolites produced by gut microbiota that have already demonstrated a protective or a deleterious effect in obesity and type 2 diabetes conditions, namely short-chain fatty acids (acetate, propionate and butyrate), trimethylamine N-oxide, indole-3-propionic acid, imidazole propionate [18,19,20,21], will also be determined at the same timepoints. Another important gut metabolite that will be assessed is ClpB, which is specifically produced by Hafnia alvei strain and is related to its recognized metabolic effect on appetite regulation [22]. Changes in ClpB levels will be determined before (baseline and 3 months) and after the intervention (6, 9, 12 months).
Additionally, the trial will assess the effect of supplementation on inflammatory markers, including calprotectin, zonulin, c-reactive protein, lipopolysaccharides, transforming growth factor-β, monocyte chemoattractant protein-1, interferon gamma, IL-1 β, IL-6, IL-10, and on other important metabolic outcomes, such as fasting glucose, HOMA-IR, HOMA-S, HOMA-B, and c-peptide, total cholesterol, HDL cholesterol, LDL cholesterol, VLDL cholesterol and triacylglycerides, and vitamins and minerals status (iron, calcium, zinc, copper, magnesium, vitamin B6, vitamin B12, 25-hydroxy-vitamin D) on all visits. GLP-1 and GIP will also be determined at all visits. Lastly, gastrointestinal quality of life impact will be assessed at baseline, and 3, 6, 9, and 12 months.
Sample collection and follow-up
Eligible participants are assessed five times during the trial: at baseline (visit 1), 3 months (visit 2), 6 months (visit 3), 9 months (visit 4), and 12 months (visit 5) after bariatric surgery. Intervention (i.e. intake of probiotic or placebo) is administered 3 months after the surgery. All data is collected at Hospital CUF Tejo and the specific assessments carried out at each timepoint are identified in Table 1.
Before each visit, participants are contacted and reminded of their follow-up visits and necessary preparations via e-mails and text messages. Participants are asked to prepare for all the visits by following the instructions:
Fasting for 10–12 h (allowed to drink water 4 h before the visit)
Having a last meal similar to their usual habits
Avoiding alcohol and caffeine intake on the previous day
Avoiding vigorous physical exercise on the previous day
At baseline, participants respond to a questionnaire to provide sociodemographic characteristics, clinical history, and lifestyle practices. Information regarding changes in medication, supplementation and physical activity are continuously gathered throughout the trial through the electronic patient record.
At all visits, a venous blood sample is collected by a nurse/phlebotomist into sterile serum separator tubes and K2EDTA tubes. Subsequently, blood samples are centrifuged at 3000 rpm for 10 min at 4 °C, and aliquoted. For incretin hormones aliquot, DPP-IV inhibitor is added to plasma sample to a final concentration of 10 μL/mL of blood. Participants are also instructed to collect their own faecal samples in sterile tubes with RNAlater, provided by the research team. Subjects describe their stool frequency and consistency of evacuation using the Bristol stool scale [23]. All biological samples are stored at − 20 °C (faecal samples) or − 80 °C (plasma and serum samples) until further analysis.
Anthropometry and body composition
Height is measured to the nearest 0.1 cm with a wall stadiometer (SECA®, Hamburg, Germany), following the Directorate-General for Health protocol [24]. Participants remove their clothes, socks, and any metal objects prior to measurement of body weight and body composition (including percentage of fat mass, fat mass, fat-free mass and skeletal muscle mass) by tetrapolar bioimpedance (Inbody®, model 770, Seoul, Korea). Body mass index is also obtained by the device report and percentage of excess weight loss is calculated as: \(\frac\left(\mathrm\right)-\mathrm-\mathrm\,(kg)}\left(\mathrm\right)-\mathrm25\mathrm/\mathrm m^2}\times100\) [25]. Weight and body composition is measured at all visits.
Gastrointestinal quality of life
Previous studies have shown that the administration of probiotics may improve symptomatic gastrointestinal episodes after gastric bypass surgeries and improve quality of life [26, 27]. Therefore, to assess the gastrointestinal quality of life before and after intervention participants fill out a self-reported questionnaire [Gastrointestinal Quality of Life Index (GIQLI)] at all visits. GIQLI questionnaire includes 36 items divided between five domains: symptoms, physical dysfunction, emotional dysfunctions, social dysfunction, and effect of treatment. The total score is computed as the sum of the response option to each of the 36 items, ranging from 0 (least desirable option) to 4 points (most desirable option). The total score is the sum of item points and ranges from 0 to 144, with higher scores indicating more favourable conditions [28].
Dietary intake
Dietary intake in the previous 12 months is evaluated by a validated food frequency questionnaire [29] at baseline. Throughout the trial, between visits 2 and 5, subjects complete 2-day food records to describe all foods and fluids consumed in detail including brand names, types of foods and culinary methods. Quantities are described using standard household measures and the information from food labels (where appropriate). A trained dietitian gives the standardised instructions for completing the food diaries and is also responsible for reviewing each record with the participants to clarify errors, omissions, questionable entries, or unclear descriptions. These dietary records will be entered into Food Processor SQL software V.11.1 (ESHA Research, Salem, OR, USA) also by a trained dietitian.
Glycaemic control, lipid profile, and other blood tests
Routine parameters, including fasting blood glucose, insulin, glycated haemoglobin, c-peptide, triacylglycerides, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, very-low-density lipoprotein (VLDL) cholesterol, alanine transaminase, aspartate transaminase, alkaline phosphatase, gamma-glutamyl transpeptidase, vitamins and minerals (iron, calcium, zinc, copper, magnesium, vitamin B6, vitamin B12, 25-hydroxy-vitamin D) are measured by an outsourced certified medical laboratory. Insulin resistance and sensitivity, and β-cell function are estimated by Homeostatic Model Assessment (HOMA) [30]. GLP-1 (Glucagon Like Peptide 1 (Active) ELISA, Merck®, Darmstadt, Germany) and gastric inhibitory polypeptide (GIP) (Human GIP (total) ELISA, Merck®, Darmstadt, Germany) are measured by ELISA procedure.
Gut microbiota composition and gut metabolites
Genomic DNA will be extracted and purified from faecal samples using NZY Tissue gDNA Isolation Kit (NZY Tech, Lisboa, Portugal), as described by Marques et al. [31]. Whole-metagenome shotgun sequencing will be performed on the Illumina HiSeq3000 platform to characterize gut microbiota composition as previously described [32, 33]. Gut metabolites [short-chain fatty acids (acetate, propionate, and butyrate), trimethylamine N-oxide, indole-3-propionic acid and imidazole propionate] will be evaluated by targeted metabolomics in serum and faecal samples [34]. ClpB will be assessed in serum and faecal samples by ELISA [Human Caseinolytic peptidase B protein homolog (CLPB) ELISA Kit (MyBioSource, San Diego, CA, USA)], according to manufacturer’s procedures.
Lipopolysaccharides and inflammatory markers
Quantification of lipopolysaccharide in serum samples will be performed using the Chromo-Limulus Amoebocyte Lysate (Chromo-LAL) reagent (Associates of Cape Cod, Inc., Falmouth, MA, USA), according to manufacturer’s procedures. Faecal calprotectin and zonulin levels will be measured as surrogate markers of intestinal permeability [35] by ELISA kit (IDK ® Calprotectin (stool) and IDK® Zonulin (stool) ELISA kits; Immundiagnostik, Bensheim, Germany). Moreover, c-reactive protein will also be determined in plasma samples as a marker of systemic inflammation by ELISA kit (Human C-Reactive Protein ELISA Kit; Sigma-Aldrich, St. Louis, MO, USA), according to manufacturer’s protocol. Inflammatory mediators including transforming growth factor-β, monocyte chemoattractant protein-1, interferon gamma, IL-1 β, IL-6, and IL-10 will be measured in plasma samples in batch by bead-based LEGENDplex™ analysis (Biolegend, San Diego, CA, USA)] and reactions will be run in duplicate with a BD FACSCantoII flow cytometer (BD-Biosciences San Jose, CA, USA) as described by Castela et al. [36] in a certified medical laboratory (Laboratório de Imunologia e Imunodeficiências Primárias @ NOVA Medical School, Lisboa, Portugal).









留言 (0)