INTRODUCTION
Social support can provide empathy, tangible aid, advice, and encouragement and is associated with improvements in quality of life for patients with inflammatory bowel disease (IBD) (1). Social network diversity, the types of social relationships in which a person is actively embedded, is 1 way to describe a person's social connections and the means by which they can gain access to social support. We aimed to examine social network diversity as reported by patients with IBD and to examine the association between social network, daily IBD burden, and related cognitive factors such as loneliness and psychological well-being (2).
METHODS
Patients with IBD from a single center were recruited to complete a survey of validated instruments. The Social Network Index assesses one's participation in 12 types of social relationships (3). These include relationships with a spouse, parents, parents-in-law, children, other close family members, close neighbors, friends, workmates, schoolmates, fellow volunteers, nonreligious and religious group members. Social network diversity ranges from 1 to 12 types of social relationships in which a person is actively embedded (Supplementary Digital Content, see Table S1, https://links.lww.com/CTG/A915). The University of California, Los Angeles Loneliness Index assesses loneliness by “How often do you feel left out?” “How often do you feel isolation?” and “How often do you feel that you lack companionship?” (4). The Psychological Well-being Scale corresponds to autonomy, environmental mastery, personal growth, positive relations with others, purpose in life, and self-acceptance (5).
The primary outcome was daily IBD burden using a measure from the ulcerative colitis-patient reported outcome and Crohn's disease-patient reported outcome corresponding to how much a respondent's IBD affected their life in the past 7 days (6). We compared linear regressions that examined the relationship between social network diversity and daily IBD burden to determine which model fits the data best. In model 1, we adjusted a priori for age, sex, corticosteroid use, anxiety or depression, IBD type, and disease severity (defined by current corticosteroid use or immune-targeted therapy). However, heterogeneity in the need for social support is well described. People who are lonely or have low psychological well-being may benefit most from social network diversity. Therefore, we examined the moderating effects of psychological well-being (model 2) and loneliness (model 3) using interaction terms. The model with the smallest Akaike information criterion and Bayesian information criterion was considered the best fit.
RESULTS
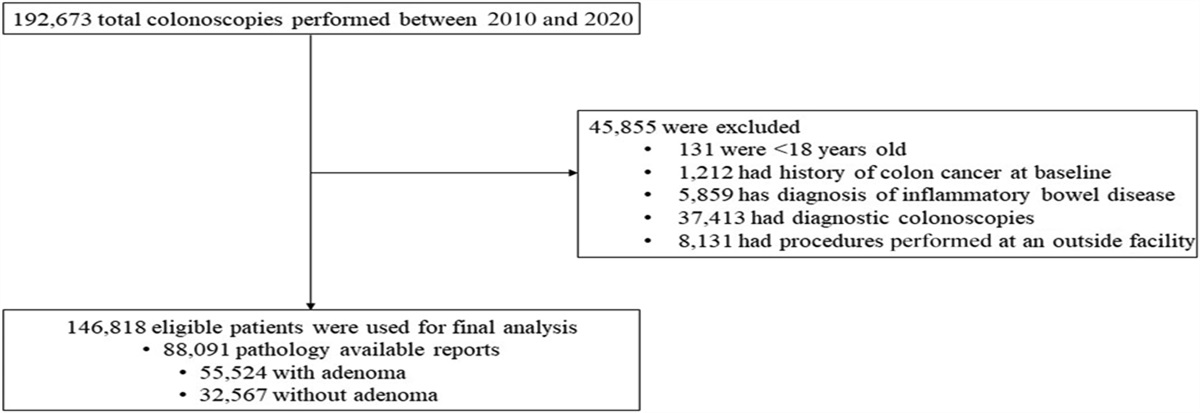
Participants were drawn from a sample of 701 patients with IBD followed at a single center. One hundred sixty-three patients with IBD completed the survey between April 2021 and 2022 (n = 152, 93.3% electronically, n = 11, 6.7% by phone) (Table 1). Respondents were of similar age (mean 41.2, SD 16.7 years) and sex (54.2% female) to our single-center population with similar diagnoses (47.8% Crohn’s disease), comorbid mental health disorders (33.8%), and biologic use (45.7%). A higher daily IBD burden was reported by participants with Crohn’s disease (mean 10.40, SD 9.64) or indeterminate colitis (mean 15.00, SD 10.58) over ulcerative colitis (mean 5.19, SD 7.02) (P = 0.032), anxiety (mean 12.80, SD 10.19, P < 0.001), or depression (mean 12.80, SD 10.19, P < 0.001) and those receiving corticosteroids (mean 12.59, SD 9.39, P = 0.023) (Table 2). Participants reported active participation in a mean of 5.61 (SD 1.72) types of social relationships. Most often these relationships were with friends (n = 135, 82.8%), relatives (n = 114, 69.9%), children (n = 103, 63.2%), or parents (n = 103, 63.2%).
Table 1. -
Patient characteristics associated with social network connections
Patient characteristics
Overall
Social network diversity (mean, SD)
P value
Total (n)
163
5.61 (1.72)
Demographics
Age
0.190
40 yr or older
116 (71.6%)
5.72 (1.74)
Younger than 40 yr
46 (28.4%)
5.32 (1.67)
Sex
0.550
Male
71 (43.6%)
5.52 (1.65)
Female
92 (56.4%)
5.69 (1.78)
Education
0.141
High school diploma
11 (6.9%)
4.73 (1.10)
Some college
33 (20.8%)
5.85 (1.52)
Associate degree
17 (10.7%)
5.77 (1.44)
Bachelor degree
49 (30.8%)
5.55 (1.99)
Graduate degree
49 (30.8%)
5.78 (1.70)
Missing
4 (0.0%)
4.25 (2.06)
Location of residence
0.756
Urban
26 (16.4%)
5.27 (1.85)
Suburban
100 (62.9%)
5.66 (1.76)
Rural
33 (20.8%)
5.70 (1.61)
Missing
4 (0.0%)
6.0 (0.82)
Race
0.752
White
140 (85.9%)
5.73 (1.72)
Black
12 (7.4%)
5.50 (1.45)
Other
11 (6.8%)
4.27 (1.62)
Comorbid diagnoses
Depression
54 (33.1%)
5.00 (1.47)
0.001
No depression
109 (66.9%)
5.92 (1.77)
Anxiety
54 (33.1%)
5.00 (1.47)
0.001
No anxiety
109 (66.9%)
5.92 (1.77)
IBD-related details
IBD type
0.149
Ulcerative colitis
75 (46.3%)
5.55 (1.56)
Crohn's disease
73 (45.1%)
5.53 (1.83)
Indeterminate colitis
5 (3.1%)
5.60 (0.89)
Unknown
10 (5.6%)
6.56 (2.24)
Crohn's disease phenotype
Fistulizing
26 (35.6%)
5.96 (2.07)
0.262
Nonfistulizing
137 (64.4%)
5.55 (1.65)
Stricturing
33 (45.2%)
5.61 (1.50)
0.978
Nonstricturing
130 (54.8%)
5.61 (1.78)
Disease extent
Colonic involvement
108 (66.3%)
5.61 (1.72)
0.980
No colonic involvement
55 (33.7%)
5.62 (1.75)
Small bowel involvement
67 (41.1%)
5.43 (1.67)
0.265
No small bowel involvement
96 (58.9%)
5.74 (1.75)
Upper gastrointestinal involvement
24 (14.7%)
5.92 (1.72)
0.352
No upper gastrointestinal involvement
139 (85.3%)
5.56 (1.72)
Current medications
Systemic corticosteroids
17 (10.4%)
5.18 (1.47)
0.270
5-aminosalicylate
40 (24.5%)
5.43 (1.71)
0.427
Immune-targeted therapy
87 (53.4%)
5.39 (1.60)
0.077
Immunomodulator
43 (26.4%)
5.28 (1.49)
0.138
Biologic
70 (42.9%)
5.43 (1.65)
0.236
History of immune-targeted therapy
Immunomodulator
88 (54.0%)
5.51 (1.67)
0.414
Biologic
84 (51.5%)
5.43 (1.73)
0.158
IBD, inflammatory bowel disease.
Table 2. -
IBD daily life impact and patient characteristics
Demographics
Mean (SD)
P value
Age
0.071
40 yr or older
7.15 (8.49)
Younger than 40 yr
9.98 (9.99)
Sex
0.500
Male
7.35 (9.30)
Female
8.33 (8.79)
Education
0.517
High school diploma
10.82 (9.79)
Some college
9.55 (8.37)
Associate degree
8.77 (8.76)
Bachelor degree
8.25 (10.23)
Graduate degree
6.02 (8.05)
Missing
1.5 (2.38)
Location of residence
0.018
Urban
9.65 (10.08)
Suburban
7.87 (9.59)
Rural
7.24 (6.28)
Missing
2.75 (2.22)
Race
0.078
White
8.0 (8.94)
Black
9.5 (11.87)
Other
4.91 (5.67)
Comorbid diagnoses
Depression
12.80 (10.19)
<0.001
No depression
5.48 (7.25)
Anxiety
12.80 (10.19)
<0.001
No anxiety
5.48 (7.25)
IBD-related details
IBD type
0.032
Ulcerative colitis
5.19 (7.02)
Crohn's disease
10.40 (9.64)
Indeterminate colitis
15.0 (10.58)
Unknown
7.22 (11.23)
Crohn's disease phenotype
Fistulizing
12.92 (9.92)
0.002
Nonfistulizing
6.95 (8.52)
Stricturing
10.73 (10.25)
0.043
Nonstricturing
7.19 (8.55)
Disease extent
Colonic involvement
7.42 (8.49)
0.336
No colonic involvement
8.85 (9.93)
Small bowel involvement
10.79 (9.56)
0.001
No small bowel involvement
5.89 (8.04)
Upper gastrointestinal involvement
15.04 (10.17)
<0.001
No upper gastrointestinal involvement
6.67 (8.21)
Current medications
Systemic corticosteroids
12.59 (9.39)
0.023
5-aminosalicylate
3.85 (6.91)
0.001
Immune-targeted therapy
8.08 (8.97)
0.787
Immunomodulator
7.49 (9.64)
0.730
Biologic
9.00 (8.93)
0.177
History of immune-targeted therapy
Immunomodulator
8.86 (9.28)
0.140
Biologic
9.63 (9.02)
0.011
IBD, inflammatory bowel disease.
Model 3 was the best fit (Table 3; Supplementary Digital Content, see Table S2, https://links.lww.com/CTG/A916). Patients with higher social network diversity reported a lower daily IBD burden (beta −1.72, 95% confidence interval −3.24 to −0.20, P = 0.027) after adjusting for age, sex, corticosteroid use, anxiety or depression, IBD type, and disease severity. We found a positive interaction between loneliness and social network diversity on daily IBD burden. Respondents with a higher degree of loneliness were more likely to have a strong relationship between social network diversity and daily IBD burden than those with a low degree of loneliness (beta 0.36, 95% confidence interval 0.18, 0.71; P = 0.039).
Table 3. -
Social network diversity and IBD daily life impact
Daily life impact of IBD
Beta
95% confidence interval
P value
Social network diversity
−1.72
−3.24 to −0.20
0.027
Anxiety or depression
1.16
−1.88 to 4.21
0.451
Loneliness
0.40
−1.49 to 2.30
0.675
Social network diversity lonelinessa
0.36
0.02 to
0.70
0.040
Current systemic steroids
4.45
0.32 to
8.59
0.035
Age 40 yr or older
−1.42
−3.92 to 1.08
0.263
Female sex
−0.94
−3.52 to 1.63
0.472
Current immune-targeted therapies
−1.41
−4.32 to 1.50
0.339
IBD type
Ulcerative colitis
Ref
Ref
Ref
Crohn's disease
2.73
0.09 to
5.38
0.043
Indeterminate colitis
1.23
−6.94 to 9.39
0.767
Unknown
2.02
−3.95 to 7.98
0.506
Race
White
Ref
Ref
Ref
Black
−0.83
−6.22 to 4.56
0.761
Other
−3.85
−8.72 to 1.02
0.120
Bold signifies statistical significance.
aModel fit: Akaike information criterion, AIC 1113.72; Bayesian information criterion, BIC 1156.86.
IBD, inflammatory bowel disease.
DISCUSSION
Social network diversity refers to the types of social relationships in which a person is actively embedded. Patients with IBD with higher social network diversity reported a lower daily IBD burden. There are several possible reasons for why social network diversity is beneficial to IBD health (1). Certain social connections may address patients' specific needs (7). A person's parents might provide tangible aid, such as a ride to an infusion, while one's friend might better encourage symptom monitoring or advise on medication adherence. By contrast, relying on support from a single close contact may have its functional limitations or lead to caregiver burn out. A higher level of social network diversity may also indicate social integration, which could strengthen psychological well-being and reduce feelings of loneliness. The relationship between social network diversity and daily life impact of IBD differed across people with varying degrees of loneliness, but not varying degrees of psychological well-being; people with higher levels of loneliness experienced less of a beneficial effect of social network diversity on IBD daily life impact. This suggests that lonely patients may benefit most from interventions that target social network diversity.
The study strengths include the use of validated instruments to collect information on social and cognitive constructs, and patient-reported outcomes. However, study limitations include a cross-sectional design that does not allow for causal inference, selection bias, and potential unmeasured confounders. Furthermore, the relationship between depression, anxiety, social networks, and IBD health is likely complex and bidirectional and will need to be studied further.
Study findings suggest there is relevance to considering diverse social connections as an indicator of risk for higher IBD burden. This may help us identify patients at highest need for interventions that aim to expand social network diversity. Several successful self-management interventions that leverage the support of one's social network have been developed for patients with diabetes and depression. For example, a patient-supporter intervention that incorporated participation of a family member or friend in coaching sessions increased their involvement in the self-management for patients with diabetes (8). Similarly, a heart failure intervention targeting care partners in automated calls led to more active care partner engagement in supporting patients' self-care (9). We can adapt these interventions to develop interventions to support IBD patients with varying social network diversity.
CONFLICTS OF INTEREST
Guarantors of the article: Shirley Cohen-Mekelburg, MD, MS.
Specific author contributions: J.P., K.R., S.C.-M., P.H., A.W.: conceptualization. L.V., J.S., A.J., S.C.-M.: data curation. S.C.-M.: formal analysis. All authors: investigation; methodology. L.V., P.H., S.C.-M.: supervision. L.V., S.C.M.: writing (original draft). All authors: critical revision of the manuscript; final approval.
Financial support: Jessica Sheehan is supported through T32 DK062708.
Potential competing interests: This research was supported by Clinical and Translational Science Award UL1TR002240 through the Michigan Institute for Clinical and Health Research from the National Institutes of Health. S.C.-M. was supported by KL2TR002241 through the Michigan Institute for Clinical and Health Research from the National Institutes of Health. P.D.R.H. was supported by R01 DK125687, R01 DK118154, R01 DK109032, and T32 DK062708 through the National Institutes of Health. J.P. is a Research Career Scientist from the US Department of Veterans Affairs.
REFERENCES
1. Kamp KJ, West P, Holmstrom A, et al. Systematic review of social support on psychological symptoms and self-management behaviors among adults with inflammatory bowel disease. J Nurs Scholarship 2019;51(4):380–9.
2. Tougas ME, Hayden JA, McGrath PJ, et al. A systematic review exploring the social cognitive theory of self-regulation as a framework for chronic health condition interventions. PLoS One 2015;10(8):e0134977.
3. Cohen S, Doyle WJ, Skoner DP, et al. Social ties and susceptibility to the common cold. JAMA 1997;277(24):1940–4.
4. Perissinotto C, Holt-Lunstad J, Periyakoil VS, et al. A practical approach to assessing and mitigating loneliness and isolation in older adults. J Am Geriatr Soc 2019;67(4):657–62.
5. Ryff CD, Keyes CLM. The structure of psychological well-being revisited. J Personal Soc Psychol 1995;69(4):719–27.
6. Higgins PDR, Harding G, Leidy NK, et al. Development and validation of the Crohn's disease patient-reported outcomes signs and symptoms (CD-PRO/SS) diary. J Patient Rep Outcomes 2018;2(1):24.
7. Ali T, Nilsson CJ, Weuve J, et al. Effects of social network diversity on mortality, cognition and physical function in the elderly: A longitudinal analysis of the Chicago health and aging project (CHAP). J Epidemiol Community Health 2018;72(11):990–6.
8. Zupa MF, Lee A, Piette JD, et al. Impact of a dyadic intervention on family supporter involvement in helping adults manage type 2 diabetes. J Gen Intern Med 2022;37(4):761–8.
9. Piette JD, Striplin D, Marinec N, et al. A randomized trial of mobile health support for heart failure patients and their informal caregivers: Impacts on caregiver-reported outcomes. Med Care 2015;53(8):692–9.

留言 (0)