
記住我
In the United States, colorectal cancer (CRC) is the third most diagnosed cancer and the second most common cause of cancer-related mortality (1,2). According to the US Multi-Society Task Force (USMSTF), individuals with 1 first-degree relative (FDR) with CRC younger than 60 years or 2 FDRs with CRC at any age should start screening with colonoscopy at 40 years or 10 years before the age at which their earliest family member was diagnosed, whichever comes first, and at least every 5 years thereafter (3–9). The USMSTF also recommends that individuals with a FDR with CRC older than 60 years start screening at 40 years and follow average-risk screening intervals (7–9).
CRC incidence and mortality in the United States have decreased with the introduction of screening and population health strategies to increase screening participation, including mailed fecal immunochemical test (FIT) outreach (2,10,11). However, many current population health screening efforts, including mailed FIT outreach, focus on average-risk populations and exclude individuals with high-risk factors, such as a family history of CRC.
Meta-analysis data from 1995 to 2012 demonstrated that only 40% of individuals with a family history of CRC receive a screening colonoscopy and only 31% undergo subsequent colonoscopy at 5 years (3). Existing studies on barriers and facilitators to screening in this group focus on provider perspectives and electronic health record (EHR) data, which can be insufficient to understand the scope of this challenge (3,4,12). Few studies have sought to understand patient perspectives (13). Thus, we aimed to determine screening participation and patient perspectives regarding CRC risk and barriers and facilitators to screening among patients with a family history of CRC excluded from our mailed FIT outreach program. Findings would inform the development of interventions to increase screening participation in this high-risk group.
METHODS Study setting and populationWe performed a retrospective cohort chart abstraction and cross-sectional patient survey at UCLA Health, a large tertiary care academic health system. The primary care population includes over 380,000 patients, with assigned primary care providers (PCPs). CRC screening is offered by PCPs and documented in the EHR, and patients who are overdue for CRC screening receive mailed FIT outreach (14–16). To determine patients who receive mailed outreach, the EHR is queried biannually. Patients with EHR documentation of a family history of CRC in the active or resolved medical problem list or visit diagnoses list are excluded and do not receive further intervention. The overall CRC screening rate in the health system is 61.4%; it is higher among patients with a family history of CRC (68.9%) than among patients without a family history (53.3%). The 90-day return rate for mailed FIT outreach has been between 12.0% and 23.0% (mean 19.0%).
For this study, we determined the subgroup of patients excluded from mailed FIT outreach in Fall 2021 because of a family history of CRC. We further excluded patients with a personal history of inflammatory bowel disease, colectomy, and/or prior CRC diagnosis.
Retrospective chart abstractionWe performed a chart review of all eligible patients to confirm CRC family history status and degree (e.g., first and second). We also extracted sociodemographic and clinical data. Sociodemographic data included age, sex, race, ethnicity, marital status, insurance status/type, and social vulnerability index (SVI). SVI determines the relative social vulnerability of every US census tract based on socioeconomic status, vehicle access, housing, etc. Higher SVI values represent more social vulnerability. Clinical data included hemoglobin A1c, body mass index, tobacco use, alcohol use, last PCP visit, last gastroenterology visit, last breast and cervical cancer screening (if applicable), most recent colonoscopy, and the recommended screening interval at that time.
Cross-sectional patient surveyThe 15-question survey was developed based on a literature review, reviewed by 3 independent study personnel, and piloted before use (3,13,17–27). Survey questions asked about (i) the presence, degree, and age of family members with a history of CRC (2 questions), (ii) healthcare providers' past CRC-related recommendations (2 questions), (iii) patient's perceived CRC risk (1 question), (iv) CRC screening history (3 questions), (v) barriers to screening (if no prior colonoscopy) (1 question), (vi) recommended screening facilitators (1 question), and (vii) demographics (4 questions). Participants identified their barriers to and facilitators of screening from a list and could indicate “other” to add additional barriers or facilitators. The final survey question asked for participants' permission to contact their PCP to order a screening colonoscopy if they were overdue for screening.
In September 2021, we mailed the survey, a consent document with study personnel’s contact information, and a prestamped return envelope to all eligible patients. Patients who did not return the survey within 6 weeks were contacted by the study personnel (S.J.) to offer telephone administration of the same survey. The study personnel read the survey verbatim to ensure standardized delivery of the questions. All survey participants were offered a $5 gift card.
Statistical analysisChart review data analyses were limited to patients confirmed to have a family history of CRC. We used frequencies and percentages or means and standard deviations (SDs) to summarize study population sociodemographic and clinical data. To compare characteristics of patients with a confirmed family history of CRC who were overdue for screening with patients with a family history who were not overdue for CRC screening, we used the χ2 test (or the Fisher exact test where appropriate) and Student t test. These analyses were conducted in SAS version 9.4 (SAS Institute, Cary, NC), and P values <0.05 were considered statistically significant.
For survey data analyses, we included survey participants who indicated the presence of a family history of CRC in response to the first survey question and tabulated survey response frequencies for each survey item. For all survey participants with a family history of CRC, we calculated frequencies of facilitators of CRC screening. For those who had never completed a colonoscopy, we calculated frequencies of barriers to colonoscopy. Finally, we compared patient-reported family history of CRC and last colonoscopy with the documented family history of CRC and last colonoscopy in the EHR.
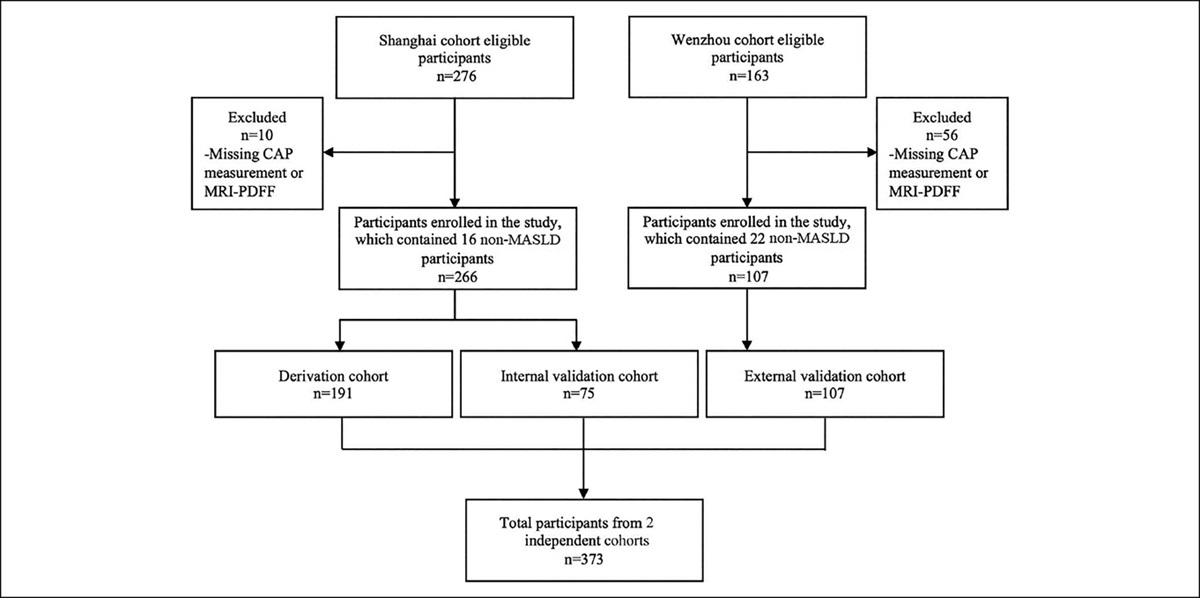
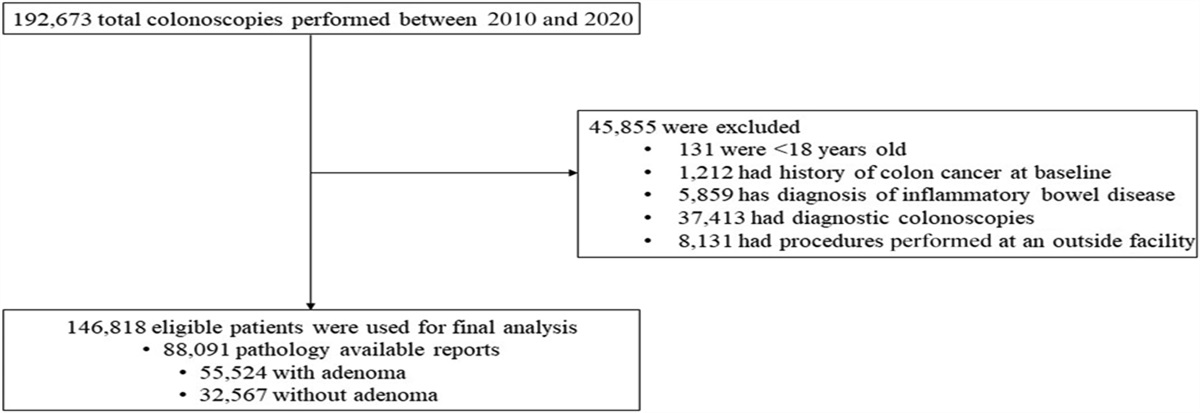
RESULTS Descriptive characteristics of the study populationThere were 296 patients (15.7%) excluded from mailed FIT outreach because of a family history of CRC and offered a survey (Figure 1). Of these, 233 patients (78.7%) were included in the chart abstraction because they had a confirmed family history of CRC in a first-degree or second-degree family member in the EHR. Of these 233 patients, 66.1% were female and 49.8% were White, and the mean age was 60.3 years (SD = 7.02).
 Figure 1.:
Figure 1.: Designation of the study population. Of the 1,882 patients excluded from the mailed fecal immunochemical test (FIT) outreach, 296 were excluded because of a family history of colorectal cancer (CRC). Of these 296 patients, 182 patients were found to be overdue for CRC screening. UCLA, University of California, Los Angeles.
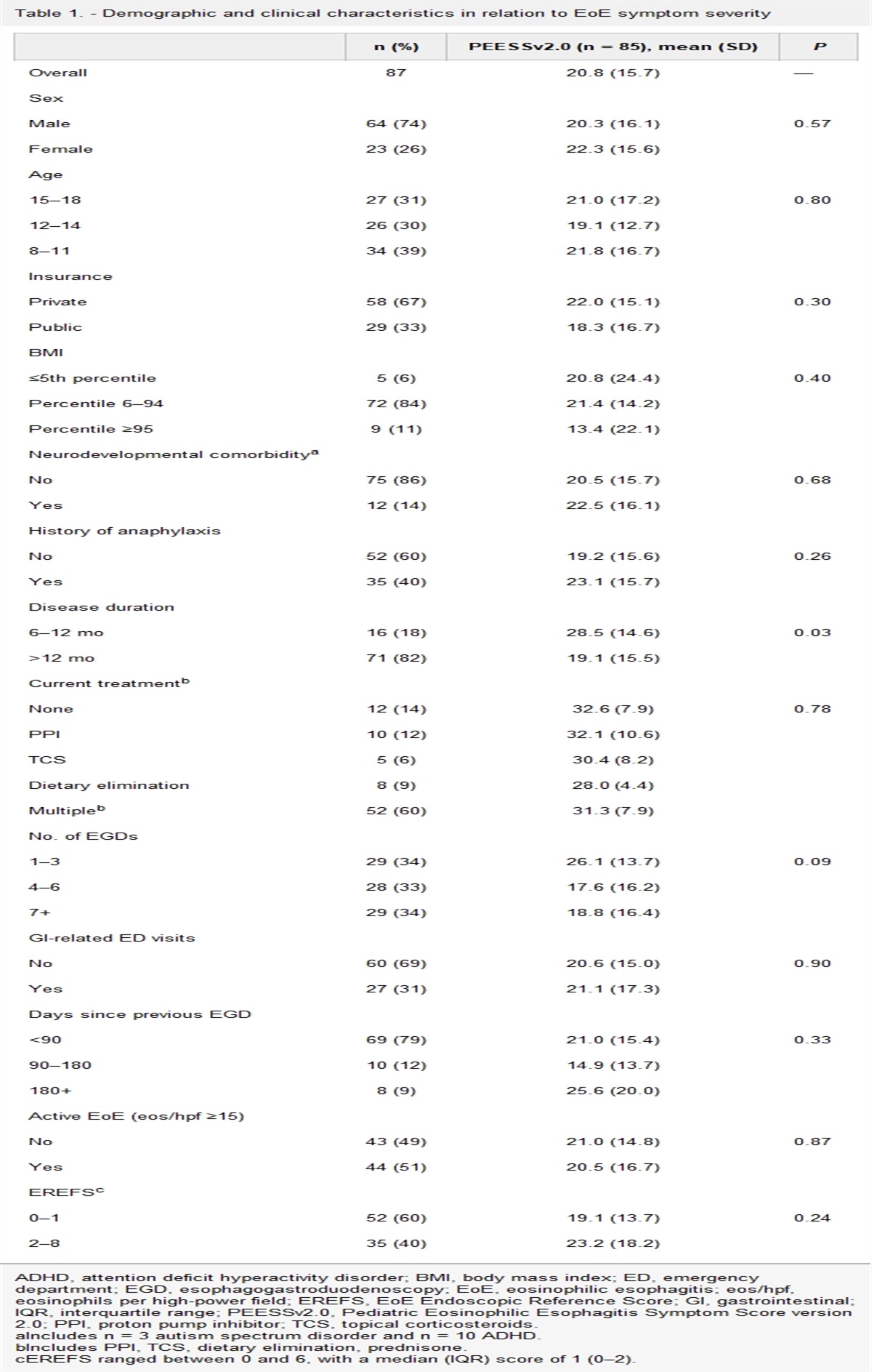
Chart abstraction resultsOf the 233 patients with a confirmed family history of CRC, 182 (78.1%) were overdue for CRC screening (Table 1). There were no significant demographic or health status differences between patients overdue and not overdue for CRC screening. There were also no significant differences in the total number of family members with CRC or the proportion of patients with only FDRs with CRC among patients who were overdue versus not overdue for screening (P = 0.25, P = 0.30). Overdue status for screening mammography was more common among women overdue for CRC screening than women not overdue (P < 0.001). In addition, an incorrectly documented screening interval (e.g., screening interval >5 years) in the EHR was more common among patients overdue for CRC screening than for patients not overdue (P < 0.001).
Table 1. - Demographic, health status, and healthcare utilization characteristics for patients with a first-degree or second-degree family history of CRC confirmed by a chart review (n = 233) Demographic characteristics OverdueBolded P values are those that were considered statistically significant (< 0.05).
BMI, body mass index; CRC, colorectal cancer; GI, gastrointestinal; PCP, primary care provider; SVI, social vulnerability index.
aComparing overdue (n = 182) with not overdue (n = 51) patients with a family history of CRC.
bSVI is based on US Census data and determines the social vulnerability of every census tract based on socioeconomic status, vehicle access, housing, race, ethnicity, preferred language, etc. Higher SVI values represent more social vulnerability.
cHealth status variables are factors generally associated with the overall health.
dAlcohol use disorder is defined as >7 drinks per week in women and >14 drinks per week in men.
eHealthcare utilization variables are factors depicting a patient's overall engagement with the healthcare system.
The response rate for the mailed survey was 14.5% (43 of 296), and the total survey response rate increased to 26.7% (79 of 296) after telephone outreach. Among participants, 81.0% (64 of 79) reported a history of CRC in at least 1 family member: 75.0% (48 of 64) had one FDR with CRC; 6.3% (4 of 64) had first-degree and second-degree relatives with CRC; and 3.1% (2 of 64) had multiple FDRs with CRC (Figure 2).
 Figure 2.:
Figure 2.: Responses to survey questions about the presence and degree of a family history of colorectal cancer (CRC). Of the 296 patients excluded from mailed fecal immunochemical test outreach because of a family history of CRC, 79 responded to the mailed or telephone survey. The survey participants indicated whether they had a family history of CRC and, if so, which relative was diagnosed with CRC.
Most of the participants with a family history of CRC (59 of 64, 92.2%) indicated that they were aware that they were at increased risk of CRC, but only 57.8% (37 of 64) said that a healthcare worker had notified them of this increased risk. Overall, 95.3% (61 of 64) reported receiving a recommendation from a healthcare provider to have a screening colonoscopy. Only 77.0% of participants (4 of 64) reported a prior colonoscopy, and of those, 21.3% (10 of 47) were overdue for their next colonoscopy.
Comparison of survey responses with EHR documentationSurvey responses about the presence and degree of family history matched chart abstraction data for 86.1% of survey participants (68 of 79); 3.8% (3 of 79) reported a family history of CRC that was not documented in the EHR; and 3.8% (3 of 79) denied a family history of CRC that was documented in the EHR. Interestingly, age at diagnosis of CRC in family members was not documented in the EHR 50.0% (32 of 64) of the time. Last documented CRC screening matched survey responses for 71.9% of participants (46 of 64), but 21.9% (14 of 64) reported more recent screening than documented in the EHR.
Patient-reported barriers and facilitators to CRC screeningOf the 81.0% of survey participants (64 of 79) who reported a family history of CRC, 17 of 64 (26.1%) reported no history of colonoscopy. For the 17 participants without prior colonoscopy, major barriers to screening colonoscopy included patient forgetfulness (6, 35.9%), competing demands (5, 29.4%), hesitancy about bowel preparation (5, 29.4%), fear of sedation during the procedure (4, 23.5%), and fear about pain/discomfort during the procedure (3, 17.7%) (Figure 3). When asked what would facilitate participation in screening, the 64 survey participants with a family history of CRC recommended telephone reminders to schedule colonoscopy (36, 56.3%), education about familial risk (32, 50.0%), letter reminders to schedule colonoscopy (25, 39.1%), and colonoscopy procedure education (23, 35.9%).
 Figure 3.:
Figure 3.: Responses to survey questions about reasons for lack of screening colonoscopy. Among the 79 survey participants, 17 participants had never had a screening colonoscopy. These participants were asked to indicate all of the barriers they faced to complete screening colonoscopy out of a list of possible barriers created based on a literature review, including “other.”
DISCUSSIONPopulation health interventions are an important component of CRC prevention. However, these efforts often target average-risk individuals and exclude individuals at high risk, including those with a family history of CRC. Our study found that CRC screening rates are low in patients with a family history of CRC who were excluded from mailed FIT outreach in our large academic medical center. We determined that EHR documentation of family history of CRC and last colonoscopy was often incomplete and inaccurate, which potentially contributed to overdue screening. In addition, we identified several patient-reported barriers to CRC screening, including forgetfulness and fear about the procedure. Patient suggestions for interventions to improve screening participation included more reminders to schedule their screening colonoscopy and increased education about the colonoscopy procedure and familial risk. Overall, this study highlights the need for additional targeted interventions for individuals with a family history of CRC.
Previous studies to evaluate screening participation among individuals with a family history of CRC have identified multiple barriers to screening. One systematic review reported barriers including fear of procedural pain, lack of symptoms, and not having a physician recommend screening (17,18). Our patients similarly emphasized fear about the procedure, sedation, and bowel preparation, pointing to a lack of understanding and discussion about the colonoscopy procedure. However, over 90% of our survey participants reported that a healthcare provider recommended a screening colonoscopy, so this barrier was not a dominant one in our population. Another review reported lack of knowledge about a family history of CRC as a cause of overdue screening (3). Only 2.5% of our survey participants did not know that they had a family history of CRC.
In the literature, factors that have facilitated CRC screening in this population include having multiple or more closely related family members with CRC, private insurance, a doctor's recommendation to complete screening, and a discussion about the family history of CRC with their provider (17–23). Our study participants did indicate that further education from their providers about familial risk and about the colonoscopy procedure would increase their likelihood of completing screening; however, we did not identify any of these other facilitators in our study. This may reflect that most of our population had private health insurance. In addition, over 90% of survey participants reported provider recommendation for screening, yet they were still overdue for screening, highlighting the importance of focusing on patient-reported barriers when designing interventions.
Of note, studies looking at barriers and facilitators to screening in average-risk populations have identified patient forgetfulness and competing demands as primary reasons for lack of CRC screening (13). These were the 2 major barriers to CRC screening identified by our survey participants as well. This finding was surprising because we expected that high-risk patients would have greater motivation to complete screening. Instead, we see similar barriers as in average-risk populations.
Previous studies identified male sex, young age, unmarried status, low socioeconomic status, and lack of insurance as sociodemographic risk factors of being overdue for CRC screening in patients with and without a family history of CRC (13,21,22,24–26). We did not identify these sociodemographic risk factors in our study population, which may reflect a more homogeneous population than previous studies. Contrarily, similar to previous studies, we found that adherence to other cancer screening recommendations is associated with adherence to CRC screening (13,27). This finding may reflect the impact of individuals' health motivation and belief in preventative medicine on screening adherence and highlights the need for increased patient education about the importance of CRC screening to improve screening rates (28).
Our study expands on the current knowledge about potential approaches to increase CRC screening participation by exploring patient perspectives of barriers to screening and interventions to address lack of screening in patients with a family history of CRC. Although one review article suggested several interventions to increase screening in this high-risk population (e.g., improved collection of family history of CRC and involvement of family members), it did not reflect patient input on the usefulness or acceptability of these interventions (3). Our study's recommended interventions came from the high-risk patients themselves and included telephone and mailed reminders about CRC screening and increased education about the colonoscopy procedure and familial risk. We anticipate that implementing patient-informed interventions will have more patient buy-in.
Our study had several limitations. First, most of our study population was English-speaking, was at least high school-educated, and had health insurance. Thus, our findings may not be generalizable to other populations or settings. Despite this limitation, our patient population was racially/ethnically diverse (50.2% non-White), and the survey focused on all patient-reported barriers and facilitators, not just those related to cost and education. Second, we were limited by the lack of documentation of age of family members at the time of CRC diagnosis, making it difficult to accurately determine the recommended initial screening age and screening interval. This limitation was unavoidable because we were limited to retrospective data, but it highlights the need to improve the accuracy of EHR documentation of family history of CRC. Third, this survey provided participants with options to choose from general barriers to and facilitators of screening, which did not allow us to delineate the more granular reasons within the broader categories such as “competing demands” and “forgot to schedule colonoscopy.” However, this study was the first step to identify the overall themes of patient barriers and facilitators, and it points to the importance of future qualitative interviews to further understand patient perspectives. Fourth, owing to the survey nature of our study and the survey response rate of 26.7%, there is a potential for response bias and/or sampling bias. However, we offered the survey to the entire study population, and we received responses from patients who were both overdue and not overdue for screening, allowing us to understand various perspectives. In addition, we confirmed patient-reported family history and last CRC screening with EHR documentation. Overall, these limitations highlight the need for further studies aimed at understanding patient barriers to and facilitators of CRC screening.
Despite these limitations, our study has many strengths. First, we evaluated a patient population that is at high risk of developing CRC, but vastly understudied. While many studies aim to increase screening in the average-risk population, there are few that address this high-risk group. Second, we gained critical insight directly from high-risk patients to increase knowledge about what may be effective interventions in that population. Prior research has primarily focused on patient perspectives in average-risk populations, provider perspectives, and EHR documentation. Third, using patient perspectives to design future interventions will increase patient buy-in and, therefore, the impact on screening rates and outcomes. Finally, we had 64 patients provide their perspectives on barriers of and facilitators to CRC screening. Thus, this study offers a more robust sample of patient perspectives compared with previous studies.
In conclusion, our study has several implications for patients, providers, and healthcare systems. Most health systems are focused on increasing CRC screening uptake by addressing individuals who are average-risk (14–16,29). Without a similar emphasis on increasing CRC screening rates in high-risk populations with a family history of CRC, which contributes to a significant portion of CRC cases, we cannot optimize CRC screening participation and outcomes (2–4). Our study also showed that family history of CRC is not well-documented. In over 50% of cases, documentation of family history of CRC did not include the family members' age at CRC diagnosis, limiting provider ability to recommend appropriate initial screening age and screening intervals. Health systems need to establish standardized practices of asking about and documenting family history of CRC in the EHR, including the number of family members affected, degree, and age at diagnosis, to improve the ability to provide appropriate CRC screening recommendations (30,31). Our findings also emphasize a need for increased and better patient education (3). Patients commonly reported that they knew they were at increased risk of developing CRC, but had not discussed this familial risk with a provider. Patients in this study also suggested increased mailed and telephone reminders to address their forgetfulness about screening and increased education and discussion about the colonoscopy procedure. Our large health system can identify patients with a family history of CRC in the EHR and, therefore, should be able to facilitate targeted patient education and regular screening reminders for this population. All healthcare systems should endeavor to implement these patient-recommended interventions to address low CRC screening participation in high-risk individuals with a family history of CRC to reduce the overall CRC incidence and mortality.
CONFLICTS OF INTERESTGuarantor of the article: Folasade P. May, MD, PhD, MPhil.
Specific author contributions: S.J.: conceptualization, data curation, formal analysis, investigation, methodology, visualization, and writing—original draft. A.G.: conceptualization, methodology, investigation, and writing—review and editing. H.W.: data curation, formal analysis, visualization, and writing—review and editing. S.M.: resources, data curation, and writing—review and editing. F.P.M.: conceptualization, funding acquisition, methodology, resources, supervision, and writing—review and editing.
Financial support: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. However, F.P.M. is supported by the UCLA Jonsson Comprehensive Cancer Center and the Eli and Edythe Broad Center of Regenerative Medicine and Stem Cell Research Ablon Scholars Program. Funding sources did not have any involvement in the study design; in collection, analysis, and interpretation of data; in the writing of this manuscript; or in the decision to submit the article for publication.
Potential competing interests: F.P.M. is a consultant for Takeda, Medtronic, Geneoscopy, and Freenome, outside the submitted work. F.P.M. receives funding support from Exact Sciences, outside the submitted work. The remaining authors report they have no conflicts of interest.
Ethical approval: All clinical investigations were conducted in accordance with the ethical standards of the Declaration of Helsinki and its amendments. This study was conducted with ethical approval and informed consent, and the study and consent process was approved by the UCLA Institutional Review Board.
Study Highlights
WHAT IS KNOWN ✓ Patients with a family history of colorectal cancer (CRC) are at significantly increased risk of CRC. ✓ Patients with a family history of CRC require earlier and more frequent screening. WHAT IS NEW HERE ✓ Patients with a family history of CRC are often excluded from population health interventions to increase screening rates. ✓ Most of the patients excluded from mailed fecal immunochemical test outreach because of a family history of CRC were overdue for screening. ✓ Electronic health record documentation of family history of CRC and last colonoscopy is often incomplete and inaccurate. ✓ Patient-reported barriers to screening included forgetfulness and fear and uncertainty about the colonoscopy procedure, bowel preparation, and sedation. ✓ Patients recommended increased colonoscopy scheduling reminders and increased education about colonoscopy and familial risk. ✓ Multilevel interventions are needed to increase CRC screening participation among patients with a family history to help reduce CRC incidence and mortality. REFERENCES 1. Henrikson NB, Webber EM, Goddard KA, et al. Family history and the natural history of colorectal cancer: Systematic review. Genet Med 2015;17(9):702–12. 2. Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Gastroenterol Rev 2019;14(2):89–103. 3. Lowery JT, Ahnen DJ, Schroy PC 3rd, et al. Understanding the contribution of family history to colorectal cancer risk and its clinical implications: A state-of-the-science review [published correction appears in Cancer 2017;123(19):3857]. Cancer 2016;122(17):2633–45. 4. Tsai MH, Xirasagar S, Li YJ, et al. Colonoscopy screening among US adults aged 40 or older with a family history of colorectal cancer. Prev Chronic Dis 2015;12:140533. 5. Wilkinson AN, Lieberman D, Leontiadis GI, et al. Colorectal cancer screening for patients with a family history of colorectal cancer or adenomas. Can Fam Physician 2019;65(11):784–9. 6. Schoenfeld P. Evidence-based guidelines for screening individuals with a family history of colorectal cancer: More questions than answers. Gastroenterology 2018;155(5):1298–300. 7. Rex DK, Boland RC, Dominitz JA, et al. Colorectal cancer screening: Recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 2017;112(7):1016–30. 8. Wilkins T, McMechan D, Talukder A, et al. Colorectal cancer screening and surveillance in individuals at increased risk. Am Fam Physician 2018;97(2):111–6. 9. Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: Clinical guidelines and rationale: Update based on new evidence. Gastroenterology 2003;124(2):544–60. 10. Issaka RB, Avila P, Whitaker E, et al. Population health interventions to improve colorectal cancer screening by fecal immunochemical tests: A systematic review. Prev Med 2019;118:113–21. 11. Dougherty MK, Brenner AT, Crockett SD, et al. Evaluation of interventions intended to increase colorectal cancer screening rates in the United States: A systematic review and meta-analysis. JAMA Intern Med 2018;178(12):1645–58. 12. Hogan WR, Wagner MM. Accuracy of data in computer-based patient records. J Am Med Inform Assoc 1997;4(5):342–55. 13. Brown LJ, Roeger SL, Reed RL. Patient perspectives on colorectal cancer screening and the role of general practice. BMC Fam Pract 2019;20(1):109.
留言 (0)