
記住我

This investigation was an open-label, non-randomized, single-arm phase I clinical trial with a 3 + 3 dose escalation design, which was approved by the institutional review board of the Shohada Tajrish hospital and the ethics committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.REC.1396.224). This clinical trial was also registered at the Iranian Registry of Clinical Trials (IRCT20200502047277N2). In the present study, all patients who were referred to the neurosurgery department of Shohada Tajrish hospital due to recurrent GBM between October 2020 to March 2021 were screened for eligibility. Before enrollment, patients were fully informed regarding the experimental nature of the study intervention, all potential outcomes, and possible complications or intervention-related adverse events (AEs). After that, written informed consent, including all the study procedures was obtained from all patients. To improve the reporting quality, this clinical trial followed Consolidated Standards of Reporting Trials (CONSORT) guidelines.
The inclusion criteria were age ≥ 18 years, Karnofsky performance scale ≥ 70, previous diagnosis of GBM based on histopathological examination of the tumor specimen, recurrent GBM with clinical and radiological evidence highly suggestive of true progression (exclusion of pseudoprogression as mentioned later in this section), complete course of standard treatment for GBM previously, including standard chemoradiotherapy regimen with or without surgical resection, and tumor location accessible for stereotactic cell injection. Exclusion criteria were surgical resection for recurrent GBM, inaccessible tumor location (e.g., brainstem), high suspicion of pseudoprogression (mentioned later in this section), abnormal renal (serum creatinine > 1.5 mg/dL), hepatic (serum bilirubin > 1.5 mg/dL or serum transaminases level > 3 x upper limit of normal), immunologic (known immunosuppression or white blood cell < 3 × 103 cells/µL or neutrophil < 2 × 103 cells/µL), and coagulation profile (INR > 1.2 or platelet < 100,000 cells/µL), active systemic infection or positive tests for human immunodeficiency virus, hepatitis B and C viruses, any prior history of drug hypersensitivity following the use of ganciclovir, pregnancy, any contraindication for magnetic resonance (MR) imaging, and participation in another clinical trial for GBM treatment simultaneously.
Moreover, in order to exclude cases with pseudoprogression, the clinical and radiological characteristics of the patient were taken into account. Regarding this, any case with increased contrast-enhanced tumor (CET) volume, who also had clinical deterioration, increased steroid intake, and mutation status associated with poor prognosis, was included in this study. However, in case of unremarkable clinical status and absence of mutations associated with poor prognosis, further imaging studies were utilized. In this study, radiological evidence suggestive of true progression was considered as apparent diffusion coefficient ratio < 1.5 on diffusion MR imaging, relative cerebral blood volume < 3.0 on perfusion MR imaging, or choline/N-acetylaspartate > 2 on magnetic resonance spectroscopy.
After recruitment, all patients were assigned to the single study arm and no blinding was performed given the goal of the trial, which was safety evaluation. This investigation was performed according to the Declaration of Helsinki and good clinical practice guidelines. All procedures for the preparation of stem cell vectors in this study, such as cell culture and vector transduction, were performed in a good manufacturing practice (GMP)- and clinical-grade clean room, which was specifically designed to produce cellular therapy products. Moreover, all the materials used during the vector preparation process were GMP-grade in order to prevent potential contamination. Quality control at the end of the production process was performed and ADSC vectors were controlled for any potential contamination before their use.
Cellular vector preparationFor ADSC isolation, 100 mL of subcutaneous adipose tissue was obtained from a healthy donor through lipoaspiration techniques, under sterile conditions. The isolated adipose tissue was then washed with a solution containing warm PBS and antibiotics. After that, using a blade, adipose tissue was cut into 1 mm pieces and mixed with equal volumes of 0.2% collagenase enzyme for 15–30 min in the incubator (95% humidity and 5% CO2 at 37 °C). To neutralize the enzyme, the mixture was washed with 10% FBS and centrifuged at 2000 rpm for 15 min. Thereafter by using a 70 μm filter, the stromal vascular fraction was filtered. The number of mononuclear cells was then counted, and in a T-150 flask with DMEM-F12 medium and 10% FBS, 106 cells were seeded. Incubation was performed in the standard condition (95% humidity and 5% CO2 at 37 °C) for 3 days, and the supernatant was transferred to a new flask afterward. This process was performed every 4 days for 3 weeks. After that, to confirm the cell types, flow cytometry was used in each passage to evaluate the surface CD markers, including CD105, CD90, CD73, CD45, and CD34. Furthermore, the differentiation capacity of cells to osteogenic and adipogenic lineages was assessed [17].
For lentivirus production, the human embryonic kidney (HEK) 293 cell line was cultured in a high-glucose DMEM medium, 10% FBS, 1% nonessential amino acids, and L-glutamine under the standard condition. The gain of function study was performed using a plasmid (pCDH-CMV-MCS-EF1-copGFP), which had been previously digested by BamHI and EcoRI endonuclease enzymes. The TK gene was cloned into the plasmid and the protocol was tested in vitro using the GFP product. After that, by using the calcium phosphate transfection method, the HEK 293 cells (packaging cell line) with 70% confluency were transfected with 21 µg PCDH-TK, 21 µg PsPAX2 plasmid (containing Gag, Pol, Rev, and Tat), and 10.5 µg PMD2 plasmid (containing vesicular stomatitis virus glycol protein) in T75 flask using four optimized reagents containing HBSS 2 × (0.05 M HEPES, 0.28 M NaCl, 0.75 mM Na2HPO4, 0.75 mM NaH2PO4 PH = 7:05,), TE1 × (10 mM Tris-HCL, 1 mM EDTA; PH = 8), Cacl2 (2.5 Mm) and Buffered Water ( 2.5 mM HEPES PH = 7.5) on a vortex [18]. In the mentioned method, First, 4000 HEK 293T cells were seeded in a T75 flask with DMEM culture media (Gibco, USA) and 10% FBS (Gibco, USA) in standard cell growth condition (at 37 °C and 5% CO2). Two hours before transfection, the culture media was changed with DMEM containing 4% FBS and stored at 37 °C and 5% CO2 for two hours. Then, the mentioned calcium phosphate reagents were blended with helper and lentiviral vectors (psPAX2, PMD2, and PCDH-TK) in a Falcon 50 mL tube on the vortex (this condition provided suitable O2 for calcium phosphate reaction). Thus, 912 µl buffered water, 33 µl TE 1X, 52.5 µg plasmids, and 105 µl CaCl2 (2.5 M) were added and mixed in a Falcon 50 mL tube. Then, 1050 µl of HBSS (2x) was slowly added to the Falcon in a dropwise manner, under agitation and vortexing. Finally, after incubation for 5–15 min, it was transferred to a T-75 flask, which was moved backward and forward as well as side to side homogenously. The transfection efficiency was determined with fluorescence microscopy at 16 h after transfection (Fig. 1A).
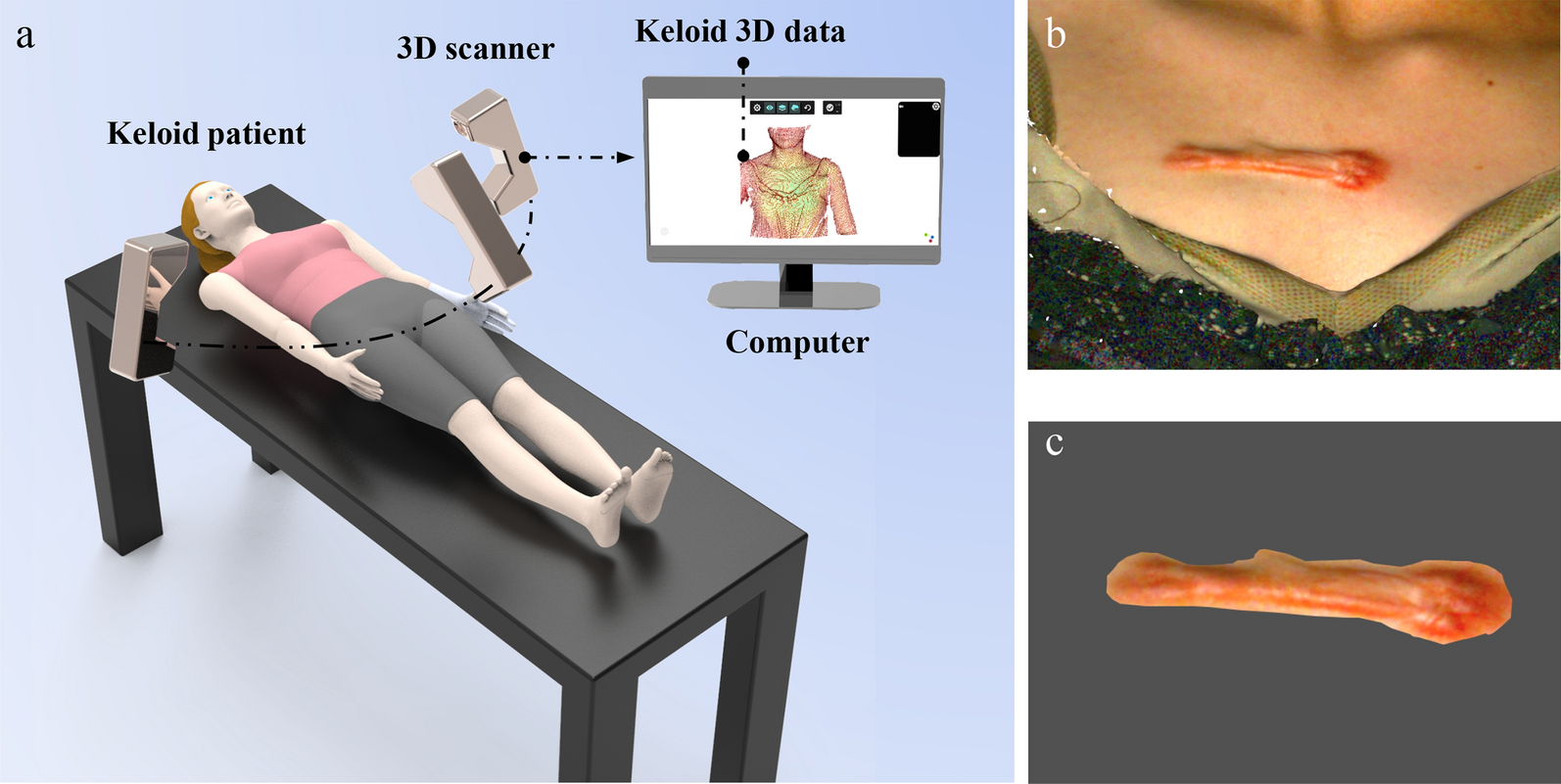
Fig. 1
Flow cytometry results demonstrating positive CD73, CD90, CD105, and negative CD34 and CD45 in mesenchymal stem cell (MSC) population
After confirming the high quality of transfection, the supernatant was isolated every 12 h for 3 days and concentrated using ultracentrifuge at 47,000 x g for 2 h at 4 °C. The TK expression in ADSCs was induced through their culture in DMEM-F12 medium and transduction with pCDH-TK lentivirus. A total of 3 × 105 cells were transferred to a T-25 flask and transduced with a multiplicity of infection (MOI) of 40 TU/cell. Moreover, cells transduced with pCDH-TK were selected using puromycin 2 µg/mL, and the efficiency of transduction was determined with fluorescent microscopy and flow cytometry (Fig. 2B, C). The U-251 cell line was also transduced and purified with concentrated mock viruses (pCDH) and pCDH-TK viruses (Fig. 3A).
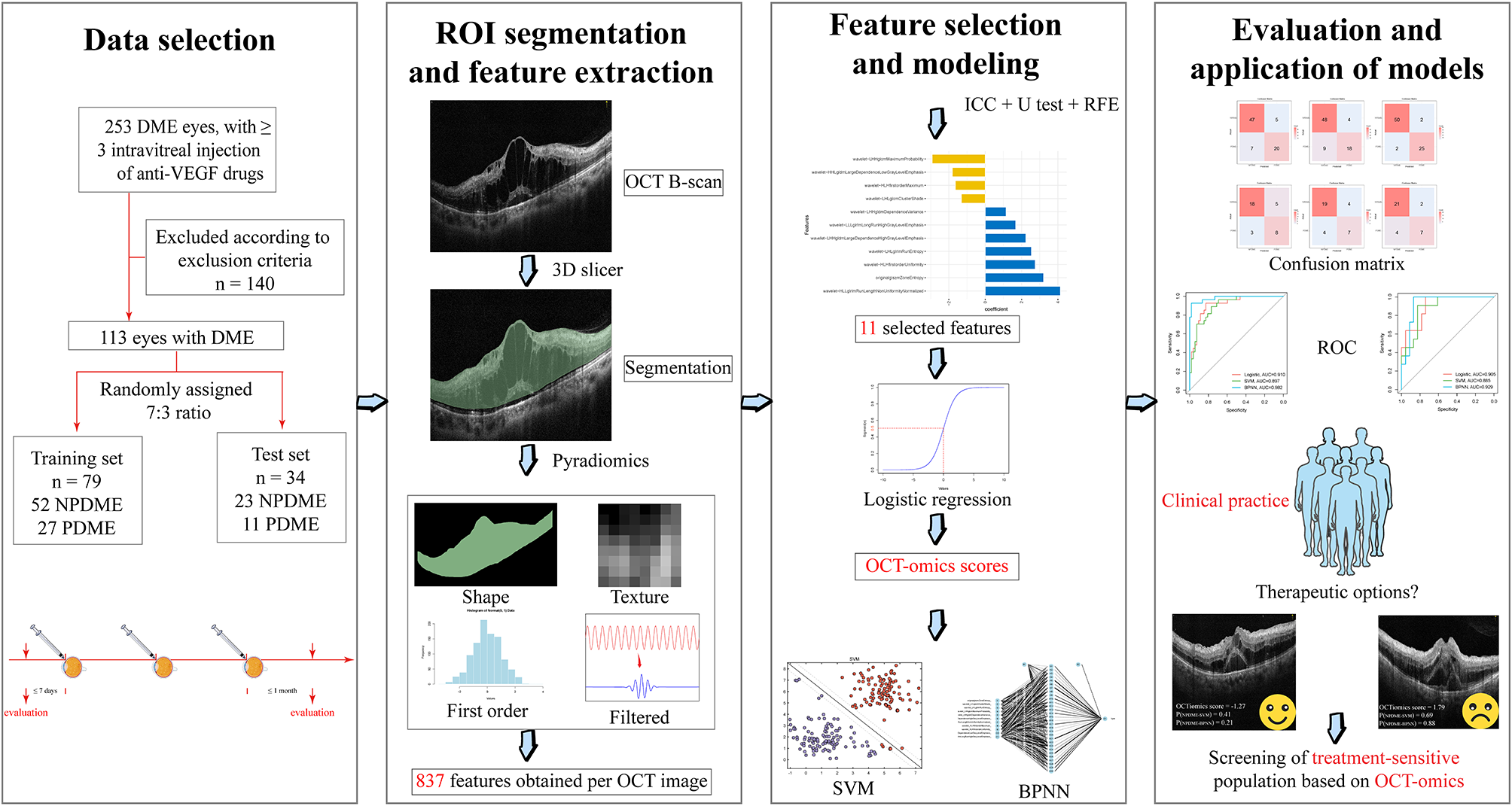
Fig. 2
HEK-293T, as packaging host, were co-transfected by psPAX2, pMD2.G, and PCDH-TK with the ratio of 2:1:2 and calcium phosphate reagent (A). Proliferation rate of high efficiency transduced MSCs based on fluorescent microscopy after 72 h (B). Flow cytometry assay confirmed the population of GFP + cells (92%) (C). The relative HSV-TK mRNA overexpression level in transduced MSCs and U-251 cells compared to control is demonstrated via bar chart (** p < 0.01)
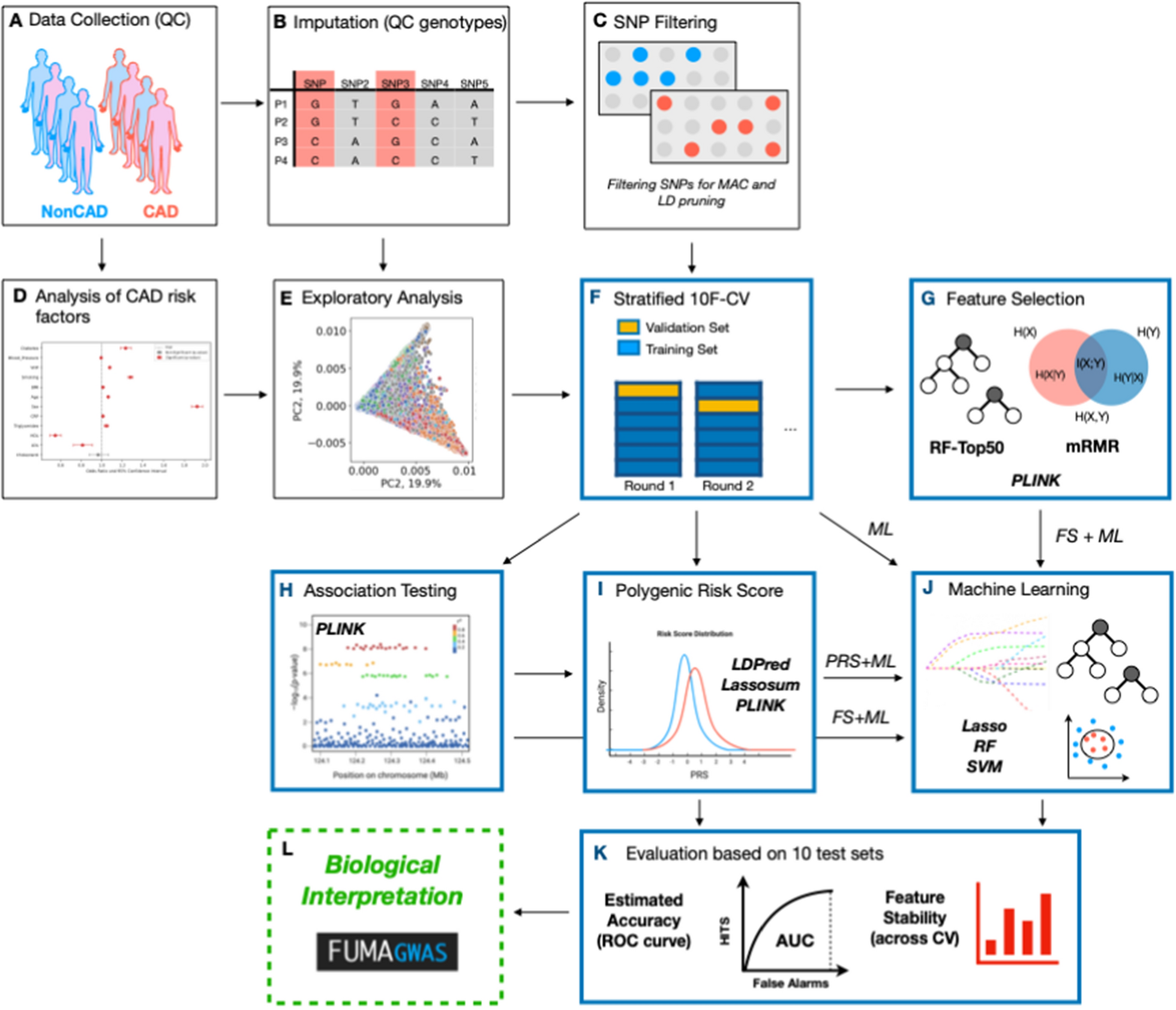
Fig. 3
The high efficiency transduced U-251/PCDH (transfected with the plasmid without the HSV-TK gene) and U-251/HSV-TK cells (more than 80% of population) observed using fluorescent microscopy (A). The viability of U-251 in serial dilution rate of ganciclovir (GCV) concentration was determined with MTT assay (* p < 0.05) (B). The relative cell survival rates of U-251/TK and U-251/PCDH cells treated in a range of GCV concentration for 96 h (* P < 0.05) (C). U-251/PCDH (D) and U-251/HSV-TK (E) in 0 µg/mL (A), 5 µg/mL (B), 10 µg/mL (C), and 20 µg/mL (D) of GCV
To investigate the HSV-TK expression, the total RNA was extracted from 5 × 105 transduced and control (un-transduced) MSCs and U-251 cell line 72 h after transduction using Trizol buffer (Thermo Fisher Scientific), according to manufacturer’s protocol. Then, the cDNA was synthesized from total RNA using reverse transcriptase enzyme -M-MuLV Reverse Transcriptase enzyme (Thermo Fisher Scientific), and random hexamer primer (for total mRNA). Finally, real-time PCR was performed in triplicate on the step one real-time PCR system (ABI, USA) using SYBR Green master mix2X (Ampliqon, Odense M, Denmark) as well as HSV-TK primers (forward primer: 5´-AATCGCGAACATCTACAC-3´; reverse primer: 5´-CCAGCATAGCCAGGTCA-3´) and HPRT1 primers as an internal control and normalizer (forward primer: 5´-CCT GGC GTC GTG ATT AGT G-3´, reverse primer: 5´-TCA GTC CTG TCC ATA ATT AGT CC-3´). The 2−∆∆CT method and graph pad prism with sample T-test were used for statistical analysis (Fig. 2D).
The effect of HSV-TK gene expression on the U-251 glioblastoma cell line in the presence of ganciclovir was measured by MTT assay. First, the resistance of the U-251 cell line against ganciclovir was determined by exposing this cell line to different concentrations of ganciclovir (0, 5, 10, and 20 µM) and investigating cell viability with MTT assay. Second, 5 × 103 of each transduced cell were seeded in the 96-well plate with DMEM culture medium (Gibco, USA) and 10% FBS (Gibco, USA) in triplicate. Then, the control (U-251-PCDH) and U-251-TK cells were treated with different concentrations of ganciclovir (0, 5, 10, and 20 µM) for 96 h under standard cell culture conditions. After that, the survival rate was calculated using the MTT assay (Fig. 3).
To prepare transduced MSCs for injection, following the purification using puromycin, cells were washed three times with normal saline and prepared for injection. Potential endotoxin contamination was prevented by using EndoFree Plasmid Qiagen Maxi Kit (Cat No./ID: 12,362) for plasmid extraction. Potential contamination with mycoplasma was evaluated using PCR-based methods with universal mycoplasma primers (forward primer: 5´-GGC GAA TGG GTG AGT AAC ACG-3´ and reverse primer: 5´-CGG ATA ACGC TTG CGA CCT ATG-3´) for detecting all mycoplasma species before and after the antibiotic usage. No mycoplasma infection was observed.
ProceduresPrior to study intervention and tumor recurrence, all patients had received standard treatment for newly diagnosed GBM, which was surgery followed by standard Stupp protocol, including radiation therapy with a total dose of 60 Gy given in 2 Gy daily fractions over a period of 6 weeks and chemotherapy with temozolomide 75 mg/m2/day. The standard chemoradiotherapy regimen was followed by adjuvant chemotherapy, including six cycles of temozolomide (150 mg/m2/day for 5 days in the first cycle and 200 mg/m2/day for 5 days every 28-day cycle). However, given the exclusion criteria of the study, no patient had undergone any treatment, including surgery for recurrent GBM before the suicide gene therapy.
The study intervention mainly consisted of two steps, including direct injection of HSV-carrying ADSCs into the tumor and prodrug administration. The ADSC administration was performed using frameless stereotaxy and neuronavigation system. Following the localization of the tumor by preoperative stereotactic MR imaging, intracerebral stereotactic injection to the cavity was performed under general anesthesia. After the needle reached the central portion of the tumor, through using a guiding cannula, 1 mL of ADSC-containing suspension was manually injected over 1 min. The needle was kept in place for two minutes after the injection. Given the study design, it included three cohorts of patients, and based on the cohort number, different numbers of HSV-TK-carrying ADSCs were administered. Cohort 1 (n = 3) received 2.5 × 105 ADSCs, cohort 2 (n = 3) received 5 × 105 ADSCs, and cohort 3 (n = 3) received 10 × 105 ADSCs. Following the stereotactic injection, patients underwent standard postoperative care. Three days after the cell injection, the prodrug administration regimen, including intravenous (IV) infusion of ganciclovir 5 mg/kg over one hour and every 12 h for 14 days, was initiated. During the postoperative course, all patients were given low-dose maintenance steroids. Patients were discharged on postoperative day 17.
OutcomesSince the main aim of this study was to evaluate the safety of suicide gene therapy, a data and safety monitoring board (DSMB), including different experts in relevant fields was established. Each patient was followed up for 24 months after the suicide gene therapy and the overall study duration was 26 months. The primary outcome measure of the present study was the safety profile of suicide gene therapy using allogeneic HSV-TK carrying ADSCs in patients with recurrent GBM, which was defined as the absence of dose-limiting toxicity (DLT). During this investigation, AEs were monitored and graded according to Common Terminology Criteria for Adverse Events (CTCAE) version 4. DLT was defined as any grade III or more non-hematological or grade IV or more hematological AEs associated with study intervention according to the DSMB decision and occurring within 4 weeks following the stereotactic cell injection. Based on the 3 + 3 design of the study, the maximum tolerated dose (MTD) was defined as the highest dose at which no more than 0/3 or 1/6 patients experienced a DLT. If one DLT was observed in any cohort, three more patients were recruited to that dosing cohort. Safety monitoring was performed using serial physical examinations, electrocardiography, and complete laboratory investigations, including serum biochemistry, hematological, coagulation, renal, hepatic, cardiac, and metabolic profiles. In addition to baseline, all the aforementioned assessments were performed on a daily basis during the first 17 days after the surgery and monthly afterward until 3 months postoperatively. Further, all patients were informed about all the potential treatment-related AEs before discharge, and also weekly contacted through regular telephone calls. As part of safety evaluation and potential early effects of suicide gene therapy, MR imaging was also performed at baseline, 3-day (before prodrug administration and after cell injection), and 17-day (before discharge) after the injection.
In addition, potential effects of suicide gene therapy using HSV-TK-carrying ADSCs on the tumor were investigated. Secondary outcome measures for potential efficacy assessment included CET and fluid-attenuated inversion recovery (FLAIR) volumes, progression-free survival (PFS), and overall survival (OS). Quantitative volumetric analysis of changes in CET and FLAIR volumes following the study intervention and over time was performed using semi-automated segmentation method. Moreover, tumor response and progression was evaluated based on Response Assessment in Neuro-Oncology (RANO) response criteria in the present study [19]. Therefore, for evaluation of the tumor response and progression status, in addition to baseline and early time points (3- and 17-day after the injection), MR imaging was carried out every 2 months after the cell injection. PFS was defined as the time from stereotactic cell injection to the first disease progression based on RANO response criteria, and OS was defined as the time from stereotactic cell injection to death. Furthermore, changes in level of serum cytokines, peripheral blood cells and CD markers were also evaluated using enzyme-linked immunosorbent assay (ELISA, Abcam) and flow cytometry, respectively. Concerning this, blood samples were drawn at baseline, day 3, day 17, and day 60 after the cell injection.
Statistical analysisBased on 3 + 3 design of the study, all patients in this study were included in statistical analysis (n = 12). In this study, quantitative data were presented as mean ± standard deviation or median with interquartile range and qualitative data were expressed as frequency and percentage. Kaplan-Meier curves were used to demonstrate OS and PFS with 95% confidence interval (CI) for the total study population, as well as based on MGMT methylation. To compare continuous variables between different time points and baseline, Wilcoxon signed-rank test was used. P < 0.05 were considered statistically significant. All statistical analyses in the present study were performed using “R” version 3.6.3.
留言 (0)