
記住我

In the last five decades, technological inventions and enhancements have attempted to improve our understanding of AD. β-amyloid accumulation, along with several determinants like tau phosphorylation, oxidative stress, dyshomeostases of the gut microbiome and biometals have been linked to AD neuropathology. In our previous report, some of these factors were thoroughly analyzed [1]. Despite unclear mechanisms, some of these determinants appear to work both synchronously and independently. For example, oxidative stress augments β-amyloid levels to cause neurodegeneration. Correspondingly, accumulated β-amyloid triggers mitochondrial dysfunction, leading to oxidative stress [2]. Therefore, to target only one factor of the disease may not effectively result in a significant improvement. Similarly, as AD has got an intricate pathophysiological mechanism, it is possible that a combination of different interventional agents may have to be employed to effectively manage and treat the disease. In recent times, interventional agents (sodium oligomannate, aducanumab and lecanemab) have been approved by health agencies to manage the condition [2,3,4]. The more recent approval of aducanumab has received a lot of criticisms from research and medical experts, with Walsh and colleagues doing a comprehensive thought-provoking editorial in the BMJ [5]. Most of the criticisms are in relation to the lack of substantial evidence to necessitate its approval. Indeed, aducanumab does significantly mitigate β-amyloid levels. However, whether decreased β-amyloid by aducanumab is concomitant with improved cognition and ADCS-ADL (Alzheimer's Disease Co-operative Study-Activities of Daily Living Inventory) to justify its approval for usage in the clinical setting is unclear. Although one clinical trial showed aducanumab to meet both its primary and secondary clinical objectives (EMERGE) amid longer follow-up and increased dose, results from another clinal study (ENGAGE) showed the contrary [6, 7].
Trace biometals like Cu and Zn have been heavily investigated in relation to AD [8]. Both Cu and Zn are key players in oxidative stress, protein misfolding and aggregation [9, 10]. Although these biometals have been investigated at great length, minimal progress has been made in terms of their utilization as interventional agents or targets for AD. The excessive research has presented several conflicting reports to the extent of some researchers calling for the discontinuation of metal chelators for AD, while others are still in favor of them [11, 12]. Further, the tremendous studying of Cu and Zn has led to less attention being afforded to other trace biometals that are used by the human body. Cobalt is a trace biometal and a major factor in vitamin B12 synthesis. This vitamin necessitates several neurological functions including cognition [13]. There are reports showing that decreased serum vitamin B12 may enhance neurodegenerative disease risk [14, 15]. Until recently, no study had reported the connection between cobalt and PIN-1 (Peptidyl-prolyl cis–trans isomerase NIMA-interacting 1) in neurodegeneration. PIN-1 has been demonstrated to cause AD when its expression is downregulated [16]. Contrastingly, when its expression is upregulated, cancer may be triggered [16, 17]. In a recent study, cobalt decreased PIN-1 expression, and halted the G0/G1 phase of the cell cycle by curtailing cyclin D protein levels, which in turn resulted in apoptosis of H4 human neuroglioma cells. Furthermore, in increasing the concentration of cobalt, disrupted activity and function of PIN-1 mice were discerned. In the in-vivo analysis using C57BL/6J mice, significant levels of cobalt were detected in the hippocampus, cortex, and blood. This coincided with mitigated levels of PIN-1, culminating in aggravated phosphorylated tau protein, β-amyloid protein, cognitive dysfunction, and neuronal loss in both hippocampus and cortex. More importantly, the same study analyzed blood samples of patients who had undergone metal-on-metal hip replacements. Following assessment, increased amount of cobalt was observed and was concomitant with reduced PIN-1 protein [18]. Although the study results are interesting, it is also a cause for concern. This is because patients who have had such hip replacements might need regular blood checks to ascertain the level of cobalt and modulate its level should there be an increase beyond the safety threshold, thereby preventing the potential development of AD.
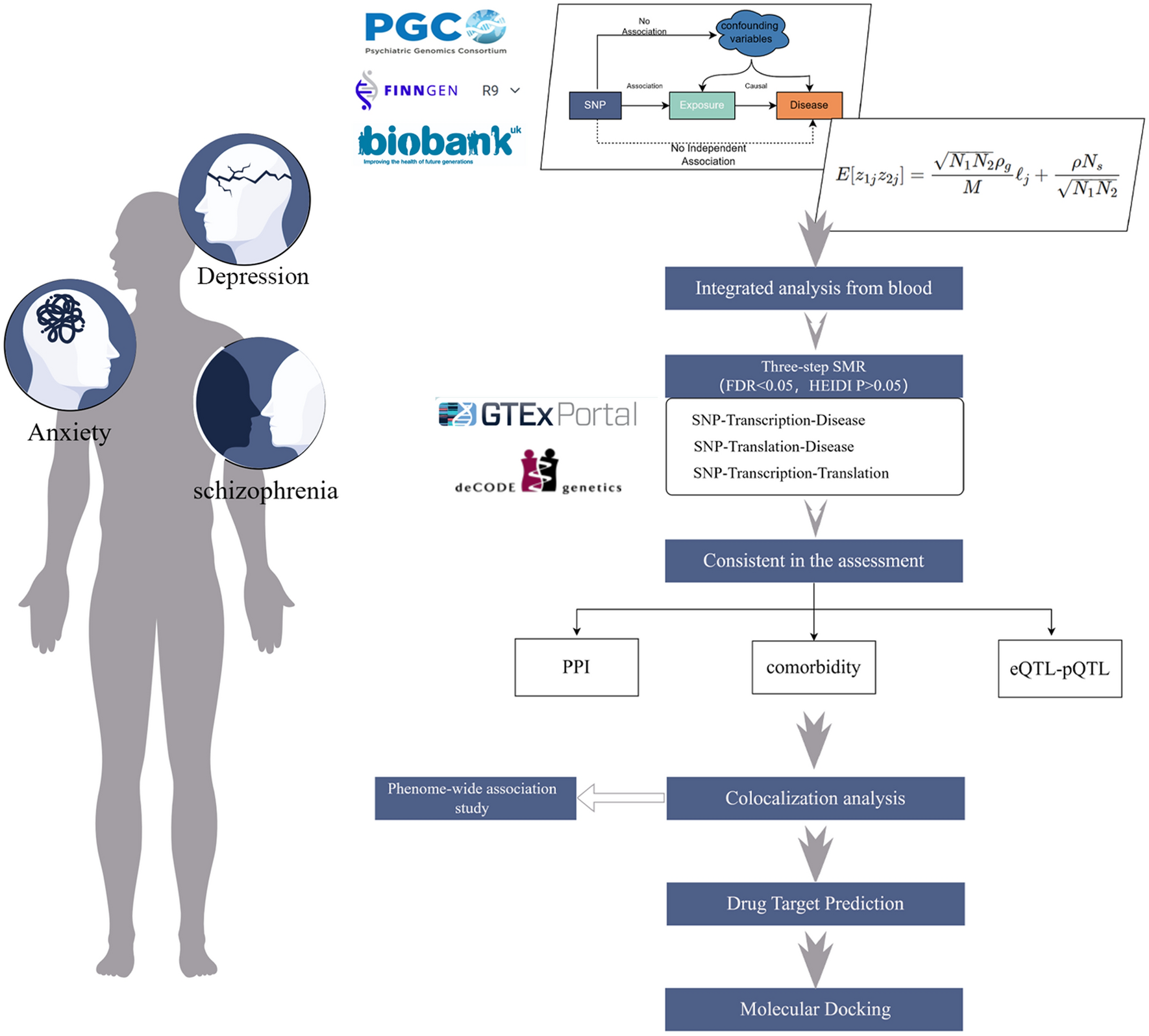
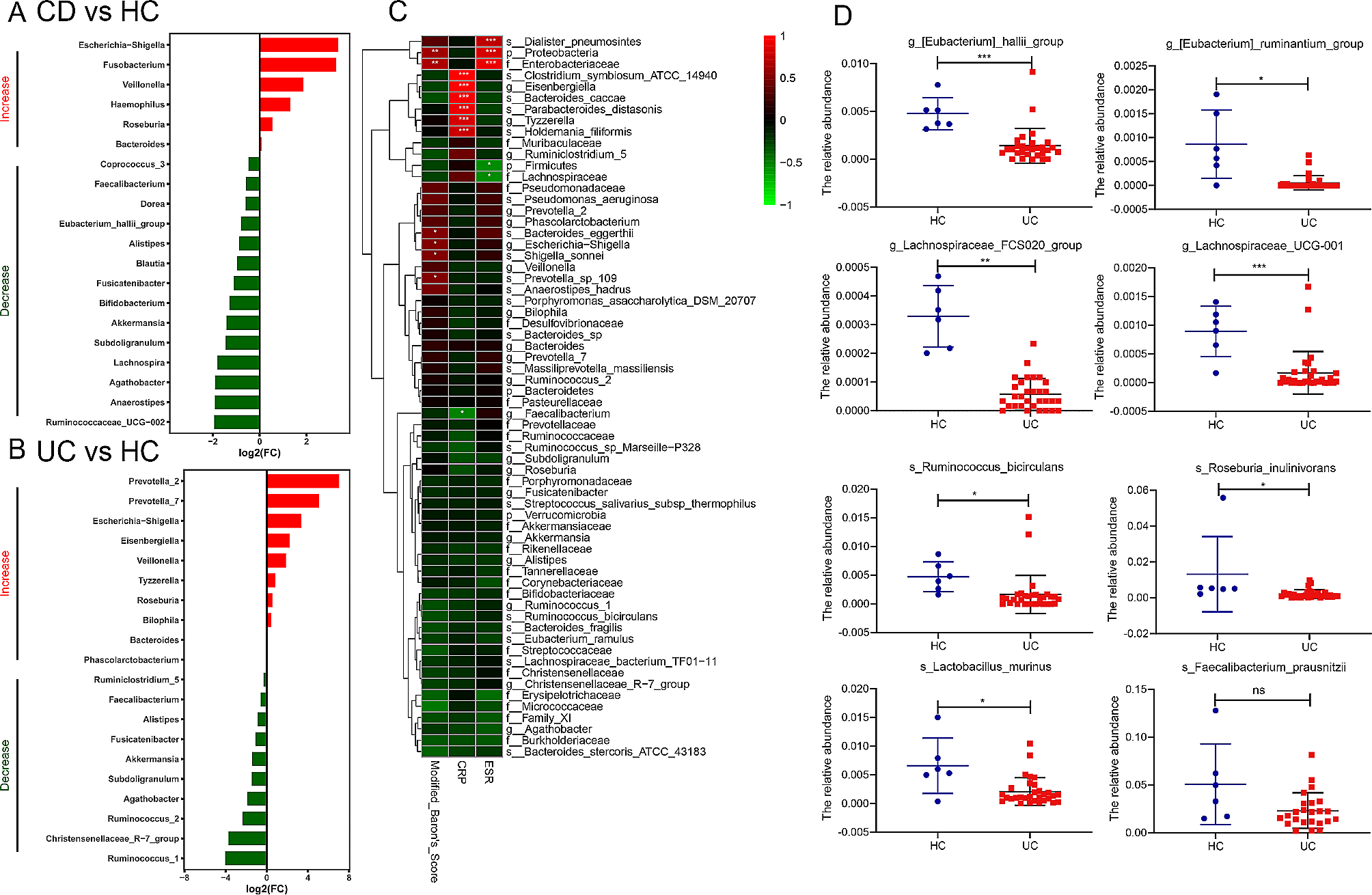
The study above underlies the need for thorough investigation of other trace biometals in AD. In that regard, we analyzed the role of two biometals (Mo and iodine) that we believe that been largely overlooked. We elaborate on their potentiality in not only as prospective interventional agents, but also as diagnostic medium for the disease. Lastly, we present figures that summarizes our report. Figure 1a shows the effects of biometal deficiencies leading to AD, Fig. 1b illustrates the potential effectiveness of molybdenum and iodine in countering AD, and Fig. 2 differentiates the level of Zn, Cu, molybdenum (Mo), and iodine between a healthy brain and an AD brain.
Fig. 1
a The effects of zinc, copper, and cobalt deficiencies in AD. In AD brain, the paucity of zinc limits the accessibility of metalloproteinase, and causes β-amyloid to aggregate. The built-up β-amyloid that forms plaques traps copper and abate its level, subsequently expediting the possibility of oxidative stress. Similarly, the AD brain has augmented levels of cobalt, which potentially downregulates PIN-1 expression and decreases the level of cyclin D. Downregulated PIN-1 expression instigates cognitive dysfunction by accelerating phosphorylated tau protein and β-amyloid accumulation. b The therapeutic effect of molybdenum and iodine. Dietary iodine may counteract oxidative stress in AD by mitigating hydrogen peroxidation formation and enhancing the output of glutathione peroxidase. Similarly, molybdenum may impair neuroinflammation through the inhibition of astrocyte and microglia formation, and result in hindering both oxidative stress and β-amyloid
Fig. 2
The different levels of zinc, copper, molybdenum, and iodine between healthy brain and AD brain. Metalloproteinases can break down β-amyloid, with zinc necessitating that function. Zinc transporters are abnormally expressed in AD brains. As zinc is displaced in AD, metalloproteinases are reduced, with the resultant effect of accumulated β-amyloid protein in the brain. Whereas some brain regions in AD patients might have lower copper levels, other areas may be in excess. Furthermore, AD brains (specifically, within the β-amyloid plaques) have higher concentration of copper than healthy brains. Besides, β-amyloid oligomers instigate cell membrane disruption and alter actin structure. However, the usage of MoS2 quantum dots may reverse these detrimental effects. Concerning iodine, its level in the brain of healthy individuals may be low and unevenly distributed. Notwithstanding, brain regions involved in cognition appear to have highest level of iodine
Overview of copper and zinc in ADConsidering the extensive reportage, we summarize some studies that have attempted to elucidate the link regarding Zn and Cu in AD.
Copper (Cu)Cu is a key trace element important for all oxygen-requiring processes, neurotransmitter synthesis, and neuronal myelination. In addition, Cu regulates the brain’s metabolic needs owing to its involvement in energy and iron metabolism [19,20,21]. Cu, as an essential cofactor, readily binds to enzymes and shifts between the Cu2+ and Cu+ oxidative states [19]. The brain is susceptible to oxidative stress triggered by the redox nature of Cu given that about 7.3% of total body Cu content is present in the brain [19]. Cu homeostasis is tightly regulated and mediated through trafficking and transportation. Ceruloplasmin is one of the main Cu-binding proteins in the plasma. In both serum and brain of AD patients, ceruloplasmin levels are elevated [22, 23]. Besides, cultured primary and secondary microglia have been used to evidence the instigation of proinflammatory response by ceruloplasmin. The inflammatory response was demonstrated by enhanced NO release and cytokines, such as tumour necrosis factor (TNF) and interleukin-1 beta (IL-1β) [24].
Cu, as an essential neuro-regulator, is released into the synaptic cleft of glutamatergic synapses during neurotransmission at micromolar concentrations [19, 25]. Free ionic Cu released at NMDA-responsive synapses activates the NMDA receptor. It is therefore not surprising that glutamatergic dysfunction in AD brain may be partly due to Cu dyshomeostasis [26]. Initially, Cu was thought to be a negative regulator of neurotransmission. However, a recent finding showed Cu to have a unique biphasic mechanism in neurotransmission [27]. In that study, hippocampal neurons of Sprague–Dawley rats exposed to Cu for 3 h resulted in augmented AMPAergic neurotransmission. This, in part, might have been due to the accumulated AMPA receptors at the plasma membrane [27].β-amyloid peptides are generated through amyloid precursor protein (APP) proteolysis [28]. APP is a transmembrane glycoprotein involved in axonal transport, vesicular trafficking, and neuronal survival. There are two alternate pathways of APP processing: the amyloidogenic and nonamyloidogenic pathways [29, 30]. The APP has two Cu-binding binding domains, one localized in the β-amyloid region and the other in the N-terminus. The presence of Cu (II) reductase activity within the Cu-binding domain of APP may potentiate ROS formation via Cu reduction [19]. Regarding the amyloidogenic processing of the APP, β-amyloid is formed through the cleavage of APP by β- and γ-secretases [29, 30]. In the nonamyloidogenic pathway, APP generates p3 peptide after it undergoes cleavage by α- and γ-secretases. Promotion of the amyloidogenic pathway and increased synthesis of β-amyloid have been consistently linked to AD neuropathology.
It is worth noting that modulation of secretases’ expression by metal ions is most likely to play a role in determining the pathway by which the APP is processed. Zn has been implicated in the regulation of α-secretase and γ-secretase activities [31, 32]. The interaction between Cu and β-secretase BACE 1 promotes the amyloidogenic processing of the APP. Moreover, Cu modifies the APP not only through the Cu-binding domain but also its processing and control of β-amyloid synthesis [33]. For instance, the work by Cater and colleagues showed that altered levels of intracellular Cu may influence the APP metabolism. In addition, elevated intracellular Cu enhanced the secretion of the α-cleaved APP, while the β-cleaved APP formation and secretion were higher in Cu-deficient cells [34].
In AD patients, some brain regions appear to have excess Cu while other areas are deficient. This mis-localization of Cu has significant effects on neuronal function, having been implicated in cognitive deficits and other AD neuropathological facets [35, 36]. In affected areas of AD brains, Cu levels are markedly curtailed and could be attributed to its entrapment in senile plaques. Specifically, the Cu content in β-amyloid plaques was nearly five-fold higher than normal age-matched controls. Additionally, tissues surrounding the senile plaques showed lowered Cu levels, indicating a possible local Cu deficiency [37].
Post-mortem examination remains the best option in ascertaining the amount of Cu in the brain and to directly detect β-amyloid plaques [35]. Measuring serum Cu may provide an insight regarding the extent of Cu in living patients, and thus, could be a prospective diagnostic tool for AD [38]. Noteworthy is that serum Cu can be in the form of non-ceruloplasmin-bound-copper (non-Cp–Cu) or bound to either ceruloplasmin or albumin. It is the uptake of free Cu ion that passes both the blood–brain barrier (BBB) and blood-cerebrospinal fluid barrier and is distributed to the CSF and brain parenchyma. In comparison to non-healthy controls, AD patients have higher copper serum levels (particularly non-Cp–Cu) [38,39,40].
In summary, Cu is necessary for various neurological functions—neuronal myelination, neurotransmitter formation and brain metabolism. Presently, there is significant gaps regarding the specific level of Cu in AD. While senile plaques may partly account for Cu paucity in some sections of the brain, what could be the rationale behind its augmented serum content in AD? What will be the best strategy in shifting Cu in the serum to other Cu-deficient compartments? In any case, will the effectiveness of that strategy correspond with significant improvement in AD? Future studies addressing some of these uncertainties could be instrumental in the development of an effective interventional mechanism for AD.
Zinc (Zn)Zn is an essential trace biometal that maintains the function of various metalloenzymes in diverse non-enzymatic biological reactions and serves as a crucial component in hormone-receptor interactions, neurotransmission, and neurogenesis [41, 42]. It participates in signal transduction processes. As a neuro-regulator, Zn modulates brain excitability by inhibiting excitatory and inhibitory receptors. Noteworthy is that Zn qualifies as both neurotransmitter and second messenger [43]. It regulates synaptic plasticity in the form of long-term potentiation (LTP) and long term-term depression (LTD), which underlies learning and memory. Both LTP and LTD are regulated by the NMDA (N-methyl-d-aspartate) receptor subunits. Far more, Zn is co-released with glutamate into the synaptic cleft to control the activity of post-synaptic proteins, NMDA and AMPA receptors (α-amino-3-hydroxyl-5-methyl-4-isoxazolepropionate-acid) [43,44,45].
Zn homeostasis in the brain is primarily modulated by metallothioneins, Zn transporters, and members of the ZiP (zinc-regulated and iron-regulated transporter proteins) family [46]. Metallothionein (MT) is a Zn and Cu modulator that induces antioxidant reaction. Growth inhibitory factor (i.e., MT-3), an isoform of metallothionein, is abundant in astrocytes, cerebellar cortex, and Zn-enriched neurons. In AD brain, MT-3 level is considerably lower. Reduced MT-3 and loss of its protective effects may exacerbate AD pathogenesis. Besides, MT-3 has been associated with various neurodegenerative diseases, such as amyotrophic lateral sclerosis, Parkinson disease, and prion disease [47, 48]. Zn transporters are divided into two major families: SLC30 (ZnTs1-10) and SLC39 (ZiPs1-14). In the cytoplasm, SLC30 and SLC39 families of zinc transporters decreases and increases intracellular Zn level respectively [49]. ZnT1 is ubiquitously expressed and exports Zn to the extracellular space of the brain. Its interaction with the GluN2A-containing NMDA receptors forms the GluN2A/ZnT1 complexes and modulates postsynaptic receptors [50]. ZnT4 is present in lysosomal and endosteum compartments of the hippocampus, and functions by loading cytoplasmic Zn in the secretory vesicles [51]. Also, ZnT6 is found in the membrane of the Golgi apparatus where Zn binds to the APP and inhibits the cleavage of the APP at the α-secretase site [52, 53]. Like ZnT1, the ZiP1 transporter is ubiquitously expressed in human tissues [54]. It increases with advancing age of the human frontal cortex [55]. In AD brains, ZiP1 level is markedly increased with disease progression and Braak staging [56]. Hence, it is possible that the upregulation of ZiP1 levels could be an attempt to maintain normal Zn homeostasis as cytoplasmic Zn concentration may decrease with AD progression [56]. Notwithstanding, further studies using appropriate animal models may provide some insight and improve our current understanding.
AD is classified into preclinical AD (PCAD), MCI, early-stage AD (EAD), and late-stage AD (LAD). PCAD patients have normal cognitive functions but with existing AD neuropathology, while MCI patients have memory loss and evidence of neuropathology but with normal daily activities [57, 58]. In AD, alteration of the SCL30 group of Zn transporter is dependent on the pathological phase of the disease. For instance, in PCAD patients, increased cytoplasmic Zn concentration is concomitant with downregulated and upregulated ZnT1 and ZnT6 expressions respectively in the hippocampus. In contrast, both EAD and LAD patients have increased expression levels of ZnT1, ZnT4, and ZnT6 [59, 60]. We are unsure of the specific reasons underlying these variations. Speculatively, during AD progression, increased level of ZnT1 might compel Zn accumulation in the extracellular space that in turn would aggravate β-amyloid deposition. In addition, Zn concentration in the trans-Golgi network increases due to upregulated ZnT6 expression that exacerbates β-amyloid aggregation through the inhibition of the APP cleavage by α-secretase. Conclusively, the effects of altered ZnT1 levels on NMDA receptor function, and how ZnT4 influences AD neurobiology is presently not clear and warrants further studies.
Controversies surrounding zinc in ADMetalloproteinases are enzymes that can necessitate the breakdown of β-amyloid. Interestingly, Zn is required for the normal functioning of metalloproteinases [61]. In AD, Zn displacement curtails the overall availability of metalloproteinases within the brain. With the decrement of this enzyme, β-amyloid is likely to aggregate in the brain and gradually instigate AD-associated symptoms, such as cognitive decline. Therefore, attenuated metalloproteinases owing to Zn dysfunction could partly account for the possible rationale behind β-amyloid accumulation in the brain of AD patients. It is worth noting that the blood–brain barrier (BBB) limits the traversal of molecules and pathogens from the peripheral to the CNS, and Zn is no exception. Interestingly, when Zn2+ was conveyed across the BBB of APP23 mice, mitigated β-amyloid plaques, cytokines, and synaptic loss were observed at a significant degree [61].
Several contentions regarding Zn and its resultant effect in AD have been put forward. Notably, β-amyloid and APP proteins were exacerbated in APP/PS1 mice that were given water containing ZnSO4 (20 mg/mL or 20 ppm). This led to compromised memory and spatial learning [62]. In a subsequent preclinical study, hippocampal synaptic proteins (PSD—93&95, NR2B, NMDA-NR2A, AMPA-GluR1) and dendritic spines were considerably lower in 21-day old ICR mice that had been administered water containing high doses of Zn (60 ppm or 60 mg/mL). In addition, memory dysfunction, along with curtailed level of hippocampal BDNF and TrkB neurotrophic signaling were reported [63].
On the contrary, some reports have observed Zn supplementation to improve cognition and improve mitochondria function. For instance, Corona and colleagues did observe increased BDNF levels as well as decrement in both tau and β-amyloid pathologies in 3xTg-AD mice that had been administered with ZnSO4-supplemented tap water. The enhanced BDNF levels was related to the instigation of matrix metalloproteinases. Additionally, mitochondrial activities were restored in the hippocampal region [64]. In a more recent study, Zn supplementation improved the short- and long-term recognition memory of young rats as well as the short-term recognition memory and spatial working memory of adult rats. Interestingly, exacerbated Cu contents were neutralized by zinc supplementation [65].
Zn supplementation regulates oxidative stress. For example, adult male Wistar rats were exposed to cadmium for 6 months to induce oxidative stress in the brain. When Zn (either 30 or 60 mg/L) was administered to these animals, the cadmium-instigated oxidative damage was reversed. This was evidenced by the enhanced antioxidative markers (SOD, CAT, GPx) and mitigated pro-oxidant factors (such as myeloperoxidase and H2O2) [66]. In a meta-analysis study involving adults taking Zn supplements, decreased oxidative stress was observed following serum analysis. Interestingly, this also coincided with decreased inflammatory markers (TNF-α and C-reactive protein) [67].
While the precise role of Zn in neurodegeneration, particularly AD, remains a topic of interest, we believe its homeostasis in the brain must be tightly controlled. As such, studies addressing the optimal level of Zn in the brain necessary for favorable outcomes in AD would be worthwhile. Further, whether increase in Zn concentration in the brain via supplementation or diet has a direct effect on biomarkers such as SOD in curtailing oxidative stress in AD is presently unclear. In addition, whether excessive Zn level in the brain might compromise the function of SOD and lead to oxidative stress is open to question. To thoroughly understand Zn’s mechanism, feasibility, and potential applicability in AD, prospective studies will have to address some of these challenges.
The need for investigations of other biometals: significance of molybdenum and iodine in ADIodineIodine is a biometal whose role in biological processes in humans cannot be overstated. Besides being involved in the metabolic processes of thyroid hormones (thyroxine (T4) and triiodothyronine (T3)), conditions such as goiter come about because of its decreased intake in diet [68, 69]. There is presently no study that has specifically investigated and correlated iodine levels directly to AD. However, several reports have attempted to link iodine and AD via thyroid hormones [70, 71]. Some of the association being made pertains to thyroid hormones involvement in neurotransmission, cognition, and hippocampal function, with reports such as that of Redman et al. thoroughly reviewing these relations [71]. As previously stated, synaptic plasticity promotes learning and memory. Therefore, its dysfunction is likely to affect cognition [
留言 (0)