
記住我









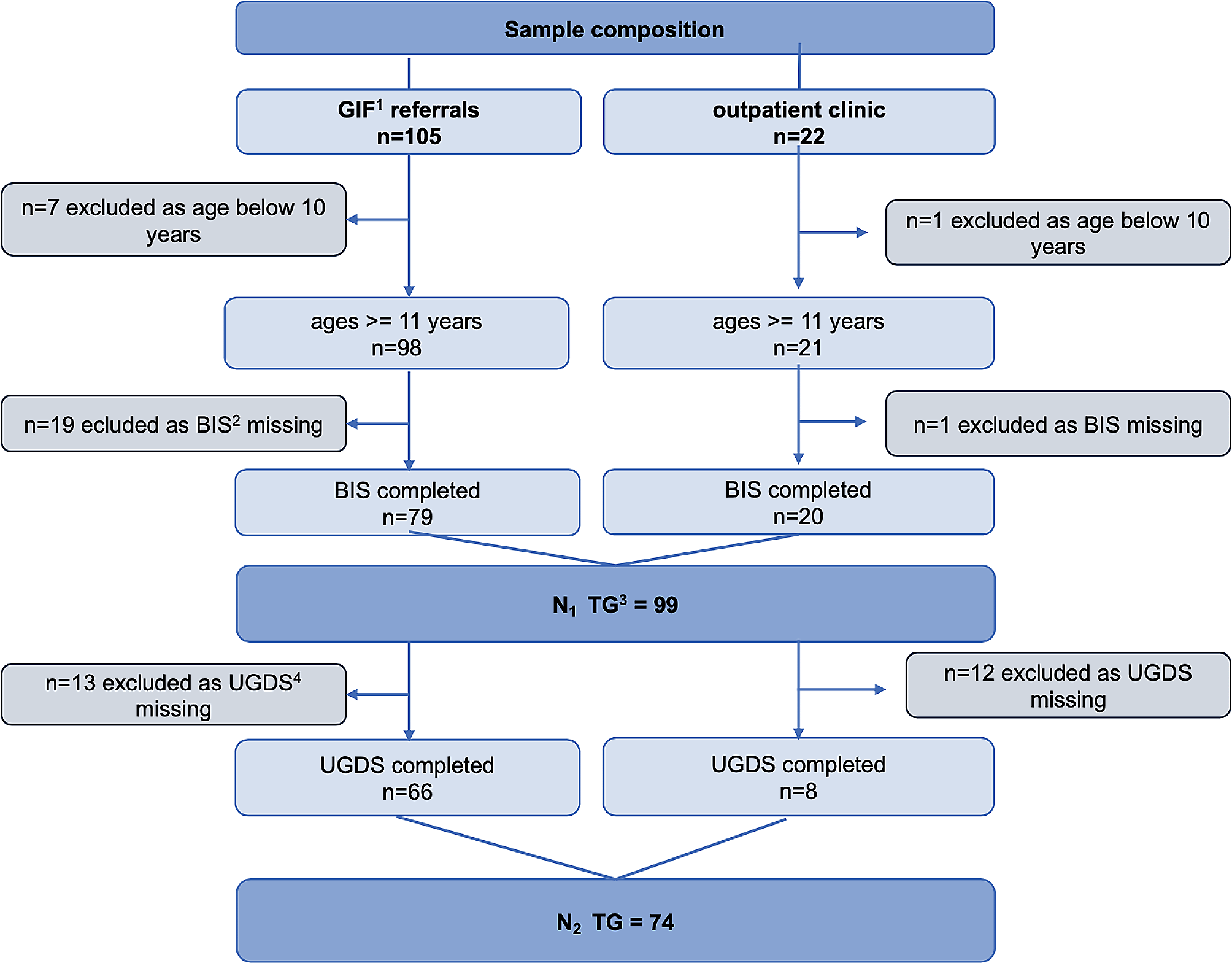
50 adolescents between the age of 12 and 18 years (Mage = 15.8, SDage = 1.52) with a history of depression (n = 25 current depression, n = 25 remitted depression) took part in the study (see flowchart, Additional file 1). The presence of a current or remitted depression based on ICD-10 [27] and potential current or past comorbid disorders were assessed with the standardized interview “Diagnostic Interview for Mental Disorders for Children and Adolescents” (Kinder-DIPS; [28, 29]) administered by a clinician. Participants were classified as remitted if they did not meet the criteria for a depressive episode in the last two months prior to diagnostic assessment based on the “Kinder-DIPS”, as this time span is used to define full remission [30]. Participants completed the Beck Depression Inventory-II (BDI-II; [31]) as self-report to assess the severity of current depressive symptoms. Participants were in- and outpatients of the Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy, Hospital of the Ludwig-Maximilians-University (LMU) Munich. Further inclusion criteria required sufficient German language skills and an intelligence quotient (IQ) ≥ 80. If available, we used IQ information from clinical routine care based on the the Wechsler Intelligence Scale for Children - Fourth Edition (WISC-IV) [32] or the Wechsler Intelligence Scale for Children - Fifth Edition (WISC-V) [33]. If no information from routine care was available, the Culture Fair Intelligence Test-Revised (CFT-20-R) [34] was conducted instead in the context of the present study to obtain information on IQ. Exclusion criteria were acute suicidality, a current or past diagnosis of asthma (as the control information booklet informed about asthma), or a current or past comorbidity with schizophrenic disorder, pervasive developmental disorder, bipolar disorder, or mental and behavioral disorder caused by psychotropic substances. Participants were randomly assigned to one of two groups: The experimental group (EG), who received an information booklet about youth depression; and the active control group (CG), who received an information booklet about asthma in youth. Randomization was based on a predefined list which included a 1:1 randomization stratified by sex and age (< 15 years vs. ≥ 15 years of age). The EG and the CG were comparable in demographic and clinical characteristics (see Table 1). 60% of the participants in both groups had at least one current comorbid psychological disorder on axis I (mainly anxiety disorders).
Table 1 Demographic and clinical characteristics of the study sample (N = 50)As in the present study, we included questions about the acceptance of the information booklet, we assessed participants’ social desirability with the Social Desirability Scale-17 (SDS-17; [35]). The two groups did not differ in socially desirable response tendencies (p = .489). As depression may impact on cognitive functions, like attention [36], we applied the “d2” test (d2; [37]), a well-established paper-pencil instrument to assess concentration and attentional performance. The EG and CG were comparable in their attentional performance (MEG = 104.32, SDEG = 9.24, MKG = 101.52, SDKG = 9.36, p = .292).
The study was approved by the institutional review board and was performed in accordance with the latest version of the Declaration of Helsinki and national legislation. Participants were informed about the aims and procedures of the study and provided written informed assent (participants < 18 years) or written informed consent (18-year-olds). Additionally, for those < 18 years, written informed consent was obtained by at least one parent/legal guardian after they had been informed about all aspects of the study.
Materials and procedureThe information booklet about depressionThe information booklet about depression (“Paul down in the dumps. Understanding depression in adolescents”; German: “Paul ganz unten. Depression bei Jugendlichen verstehen.”) was developed by our group [16, 25]. It is a twenty-sided hardcopy information booklet, which addresses healthy adolescents as well as adolescents with depression. The storyboard is about Paul who suffers from depressive symptoms. Emilie, his friend, suffered from depression in the past and now supports Paul by offering him advice. The booklet presents evidence-based information on seven depression-related topics in an age-appropriate way (prejudices, symptoms, treatment, antidepressants, causes, suicidality, and helping behavior). The content and layout of the booklet are described in detail elsewhere [16, 25]. Exemplary illustrations of the booklet are shown in Fig. 1.
Fig. 1
Cover illustrations and the page about information on symptoms of the diseases (written in German). For an English translation of the textual information imbedded in these illustrations, see Additional file 2.
The information booklet about asthmaFor this study, we developed a hardcopy control information booklet which informs about asthma as one of the most common chronic somatic conditions in youth [38] (“Paul out of breath. Understanding asthma in adolescents.”; German: “Paul außer Atem. Asthma bei Jugendlichen verstehen.”). Apart from differing contents, both booklets show utmost comparability in relevant aspects: The booklet about asthma has the same format, the same page count, the same illustrations as well as the same multi-color printing as “Paul down in the dumps”. Furthermore, the addressed condition-specific topics are similar (e.g., including symptoms, causes, treatment, helping offers). The narrative in the booklet about asthma is adapted to this specific condition and presents Paul who suffers from asthma-specific symptoms. Emilie’s brother suffered from asthma in the past and she now tries to help Paul by offering him advice (e.g., on healthy lifestyle, avoidance of triggers). As in the booklet about depression, the language of the control information booklet is age-appropriate and easy to understand. For illustrations see Fig. 1.
Assessment of changes in knowledgeA self-designed knowledge questionnaire based on [25] and [16] was applied to measure both the baseline knowledge (pre-assessment; pre) and changes in knowledge on depression at post-assessment (post) and follow-up assessment (fu). The questionnaire included 48 items, addressing seven different topics, that are included in the information booklet about depression: (1) “prejudices” (4 items, e.g., “Seeking help for depression is a sign of weakness.”); (2) “symptoms” (19 items, e.g., “One is secluding oneself more.”); (3) “treatment” (10 items, e.g., “The psychiatrist or psychotherapist offers help when someone suffers from depression.”); (4) “antidepressants” (3 items, e.g., “When taking antidepressants, you are no longer yourself.”); (5) “causes” (6 items, e.g., “Negative experiences (e.g., death) can contribute to the development of a depression.”); (6) “suicidality” (2 items, e.g., “Suicide is a common cause of death in adolescents”); (7) “helping behavior” (4 items, e.g., “If someone is affected by depression or suicidality, one should listen and offer help.”). The questionnaire used a four-point rating scale (0: not accurate, 1: somewhat accurate, 2: mainly accurate, 3: entirely accurate) with a possible sum score range from 0 to 144 (a higher sum score reflects higher knowledge). In our sample, the internal consistency (Cronbach’s α) for the total knowledge score was 0.45 (pre), 0.78 (post), and 0.70 (fu), respectively. The higher internal consistencies at post and fu compared to pre likely reflects that the questionnaire specifically related to the contents of the booklet, which was presented after the pre-assessment.
Acceptance of the information bookletAs in [25] and [16], a self-designed evaluation questionnaire was used to assess the layout, content, utility, and overall assessment of both information booklets. The evaluation questionnaire was nearly identical for the EG and CG except that the items referred to depression or asthma, respectively. The questionnaire also used a four-point rating scale. Items are summarized in the Additional file 3.
ProcedureThe pre and post testings took place at the research laboratory of the department. Whenever possible, also the fu testings were conducted at the department. However, due to the corona pandemic, some participants had to be offered the opportunity to fill in the fu questionnaires at home. These participants (n = 6 in the EG and n = 9 in the CG) did not complete the BDI-II at fu as in our department, the BDI-II is only applied when the presence of professionals is guaranteed. The study design including the assessments is illustrated in the Additional file 4. After diagnostic information had been obtained at a diagnostic appointment (T0; Kinder-Dips, BDI-II), participants were randomly assigned to the EG or CG. At the second appointment, all participants completed the d2 and filled out the self-designed depression-specific knowledge questionnaire (T1a: pre). Participants were then instructed to attentively read the information booklet quietly to themselves (depending on group assignment either the booklet about depression or asthma) in a concentrated manner in the presence of the experimenter. Participants had 15 min to read through the booklet and were allowed to scroll back and forth. If participants indicated that they had read through the booklet before the 15 min were over, they were encouraged to scroll through the booklet once again. After the 15 min reading time, all participants completed the same knowledge questionnaire (T1b: post), which they had completed at pre. In addition, they were asked to fill out the evaluation questionnaire. After four weeks at the third appointment (T2: fu), participants filled out the same knowledge questionnaire as before (pre, post). At T2, depressive symptoms based on the BDI-II were reassessed to allow explorative analyses on the differential effects of the information booklets on depression symptomatology. Participants who received the information booklet about asthma were given the opportunity to receive the information booklet about depression after fu.
Data analysisStatistical data analysis was carried out using IBM SPSS Statistics version 26. For all analyses, the significance level was set to p = .05 (two-tailed). To obtain knowledge scores for the three time points in both groups, we calculated unweighted index values [39] based on [16]. For a similar approach and details see [16].
To compare baseline knowledge between the EG and CG, independent t-tests were calculated. Changes in total knowledge were analysed using a repeated-measures analysis of variance (ANOVA) for the index value calculated across all seven subdomains (factor time (pre/post/fu) as within-subject factor; factor group (EG/CG) as between-subject factor). To investigate changes in knowledge over time for the subdomains, we calculated a global repeated-measures ANOVA with the within-subject factors subdomain (7 subdomains) and time (pre/post/fu), and group (EG/CG) as the between-subject factor. Thereafter, a follow-up repeated-measures ANOVA with the within-subject factor time (pre/post/fu) and the between-subject factor group (EG/CG) was calculated for each subdomain. In case of significant effects in the repeated-measures ANOVAs, we conducted post-hoc t-tests, thereby applying a Bonferroni-correction for multiple testing. If the sphericity assumption was violated in the ANOVAs, Greenhouse-Geisser’s correction was applied (Mauchly’s test). To exploratively address the question whether baseline knowledge and changes in knowledge in the EG were influenced by depressive symptomatology, sociodemographic or cognitive variables, multiple regressions were conducted (for details and results see the Additional file 5).
To analyse the acceptance of the information booklet about depression in the EG, descriptive statistics (M, SD) were calculated. The overall acceptance rate between the EG and CG was compared based on an independent t-test. Spearman’s rank correlations were computed between SDS-17 scores and the answers of the evaluation questionnaire to investigate whether participants’ social desirability was related to participants’ answers. For these analyses, we applied no correction for multiple comparisons, which - in this case - is the more conservative approach with regard to the validity of our results.
In explorative subgroup analyses, we calculated Mann-Whitney U tests to determine if there are any differences in knowledge change over time (pre to post, pre to fu, post to fu) between inpatients (n = 8) and outpatients (n = 17) in the EG (for details and results see the Additional file 6).
In an explorative analysis, we investigated changes in depressive symptoms based on the BDI-II from pre to fu and ran a 2 × 2 ANOVA with group (EG/CG) as between and time (pre/fu) as within-subjects factor. Due to some missing data for the BDI-II at fu (6 out of 25 in the EG, 9 out of 25 in the CG, for details see “Procedure”), this analysis was restricted to a subsample of n = 35 participants.
Power analysisTo determine the necessary sample size to test our main hypothesis of knowledge gain in the EG from pre to post and from pre to fu, a priori power analysis was computed. As there are no other comparable studies evaluating an information booklet within a randomized controlled study design, we based our analysis on a previous study [26], which examined knowledge gain in youth after reading an information booklet about psychotherapy and mental disorders applying a pre-post-fu design. The authors found large effect sizes for knowledge gain from pre to post, as well as from pre to fu (d ≥ 1.13). Based on these results and a conservative assumption of only medium to large effect sizes in adolescents with a history of depression who presumably have prior knowledge about depression, n = 24 participants in the EG are needed to detect these effects (assuming an alpha error of 0.05 and a power of 0.80). Thus, the sample of the present study with n = 25 participants in the EG was sufficiently large to detect the expected effects.
留言 (0)