
記住我


Sickle cell disease (SCD) is a collection of inherited hemoglobin disorders that affects up to 100,000 people in the United States.1The abnormality resides in the hemoglobin molecule with the substitution of valine for glutamic acid in the beta globin chain. The resultant abnormal hemoglobin (called sickle hemoglobin or HbS) is less soluble than the wild type and forms a polymer upon deoxygenation and that results in shape change from the normal red cell disk to an elongated sickle form. SCD occurs when the HbS mutation is homozygous or is coinherited with another beta globin chain gene mutation such as beta thalassemia or hemoglobin C. Patients with SCD have a chronic hemolytic anemia and intermittent episodes of vaso-occlusion of small blood vessels leading to acute pain episodes, as well as acute and chronic injury to lungs, heart, kidneys, bone, and the central nervous system.2
When preparing a patient with SCD for surgery, there are many factors to consider. Intraoperatively, surgery may lead to hypotension, acidosis, hypoxia, frequent exposure to low temperatures, vasoconstriction, venous stasis, and increased stress, all of which can promote increased sickling and potentially induce vaso-occlusive episodes (VOEs).3,4 Additionally, patients with SCD have higher risks of perioperative infection due to functional asplenia,5 and increased risk of perioperative thrombosis as a result the underlying hypercoagulable state. Preoperative planning is required to help minimize the risks of perioperative morbidity and mortality.
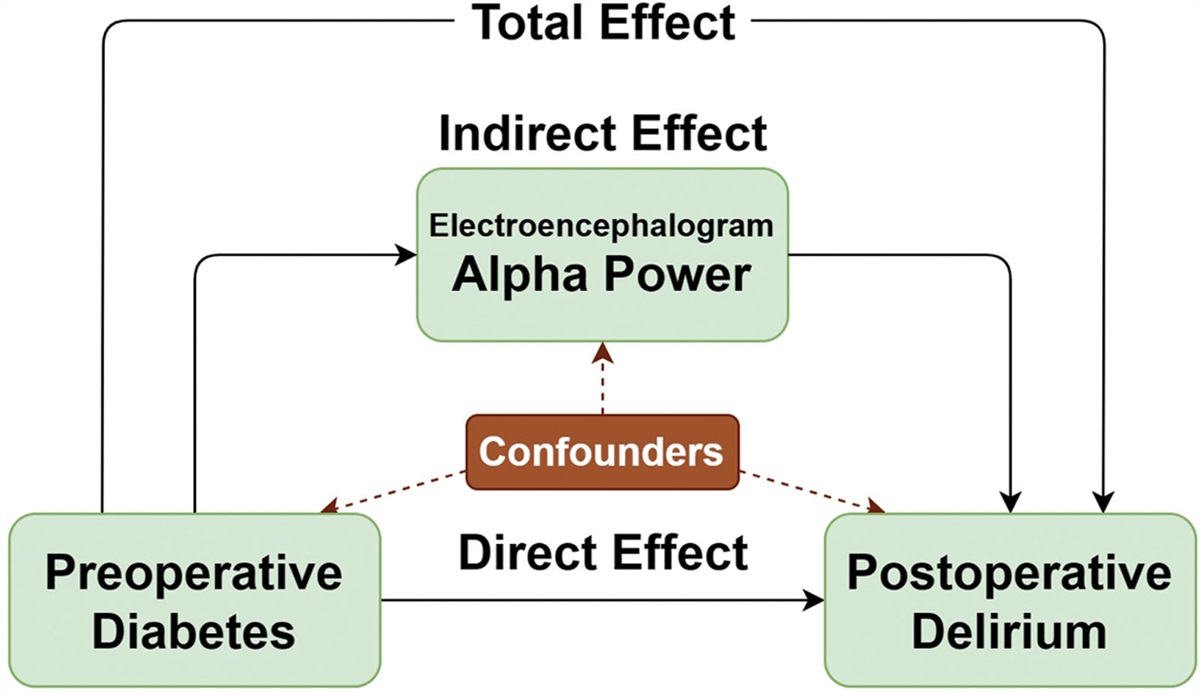
 Figure 1.: Risk of mortality by type of surgery. Adapted from the work by Koshy et al 1995.12
Figure 1.: Risk of mortality by type of surgery. Adapted from the work by Koshy et al 1995.12While standard tools are used to consider perioperative risks for all patients,6,7 none of these tools include SCD and likely underestimate the perioperative risks for this specific patient population. And currently, there are no specific tools for perioperative risk estimation in SCD.
GENERAL CONSIDERATION Fluid ManagementFluid management in the SCD population can be complicated by the presence of underlying cardiopulmonary disease and renal dysfunction. Renal dysfunction is not always reflected in serum estimated glomerular filtration rate (eGFR), and patients with normal serum creatinine values may still have degrees of tubular acidification defects, impaired potassium secretion, and decreased concentrating ability.8,9 These impairments increase the risk of dehydration and electrolyte derangements in patients with SCD. Frequent reassessments of serum chemistries and fluid balance status are recommended to avoid both complications in this population. Specifically, underhydration can lead to decreased intravascular volume, which can increase the risk of sickling, and potentially increase the risk of a VOE. On the other hand, overhydration, particularly in patients with underlying cardiovascular disease, can lead to pulmonary edema and increased risk of acute chest syndrome (ACS). Additionally, prolonged intravenous (IV) fluid use can lead to undesired fluid shifts, and rates of administration should be adjusted when patients have resumed adequate oral intake.5 Currently, there is no evidence to support an optimal rate or type of fluid.10 Normal saline (NS) is typically avoided due to in vitro studies suggesting that NS increases sickle red blood cell stiffness11 and potentially increases the risk of microvascular occlusion. Additionally, a pediatric emergency room retrospective study found that patients who received NS boluses had poorer pain control; however, this was compared to no bolus rather than to bolus with a different type of fluid.12 While the use of isotonic balanced crystalloids such as Lactated Ringer’s (LR) has been shown to decrease renal complications and risk of death in critically ill adults compared to NS,13 they have not been thoroughly investigated in the SCD population. Unless giving rapid bolus infusions, it is still recommended to use hypotonic solutions such as dextrose-containing half-NS, rather than isotonic fluids such as NS or LR, for prolonged maintenance fluid therapy given the above limited data in patients with SCD.
In all patients with SCD, we recommend careful monitoring of hydration and electrolyte status with regular chemistries, strict measurement of intake and output, and daily weights. Careful timing of surgery, preferably first case, should be undertaken to avoid prolonged NPO times and prevent intravascular volume depletion.
Temperature RegulationCold weather and temperatures have been noted to precipitate VOEs,3 and patients with SCD may additionally be hypersensitive to warming and cooling.14 Optimization and thermoregulation with a warmed blanket, optimal operating room temperature, and warmed fluids are recommended.
Intravenous AccessPatients with SCD may have difficult IV access,15 requiring additional time for preoperative planning. The underlying mechanisms driving difficult IV access are not well-studied; however, chronic damage to the endothelial lining and vasculature associated with recurrent hemolysis may contribute. Additionally, repeated blood draws and intermittent placement of large-bore catheters during acute illness could potentially contribute to vasculature damage over time. While many patients on chronic IV therapies such as monthly crizanzlimuab or monthly exchange transfusions may have indwelling ports, careful planning and appropriate allotment of time for IV access placement should be incorporated into preoperative planning. If temporary central venous catheters are required due to poor peripheral, they should be removed as early as possible to avoid the increased risk of developing venous thromboembolic (VTE) complications.16
Risk in Type of SurgeryKoshy et al17 found a wide range in risk of SCD-related complications depending on the type of surgery, with 0% in patients undergoing tonsillectomy and adenoidectomy, up to 17% for patients undergoing cesarean delivery and hysterectomy (Figure 1). Additionally, the use of laparoscopy has reduced hospital length of stays but may not reduce the risk of SCD-related complications such as ACS.18
PREOPERATIVE TRANSFUSIONS BackgroundIn general, the goal of transfusing red blood cells preoperatively in patient with SCD is to increase hemoglobin, decrease the percent of HbS, and suppress erythropoiesis.19 Unlike in the general population, the need for transfusion is really geared toward decreasing HbS% and less about concerns about blood loss and anemia.
In 1995, Vichinsky et al20 published a large prospective study involving 551 patients and 604 operations. Patients were randomized to receive the “aggressive” regimen aimed at a preoperative hemoglobin goal of 10 g/dL and HbS% <30, or “conservative” regimen aimed at a hemoglobin goal of 10 g/dL without a HbS% goal. Patients received HbSS-negative blood and leukorerduced blood if there was a history of prior febrile transfusion reaction. The study found no significant differences in intraoperative serious blood loss, postoperative ACS, or postoperative painful crisis in the aggressive versus conservative transfusion treatment groups. The investigators did, however, find a significant increase in new alloantibody formation and hemolytic transfusion reactions in the aggressive transfusion arm.
The largest prospective observation study of perioperative risk in people with SCD was published in 1995 and consisted of 717 patients undergoing a total of 1079 surgical procedures.17 The majority of those patients were homozygous for hemoglobin S (HbSS/sickle cell anemia), followed by those who were compound heterozygotes for HbS and HbC (HbSC). Transfusion specifications such as leukoreduction and antigen phenotype matching were not specified. In patients with HbSS, they found that preoperative transfusion was associated with decreased SCD-related postoperative complications only in those undergoing low-risk procedures, and no associated benefit in those undergoing medium- or high-risk procedures. Patients with HbSC disease demonstrated benefit for all surgical procedures.
A multicenter randomized prospective study published in 1999 investigated perioperative complications in patients with sickle cell anemia who were undergoing tonsillectomy and/or adenoidectomy or myringotomy at 36 participating centers. Patients were randomized similarly to the Vichinsky et al trial, with the “aggressive transfusion” arm defined as targeting a hemoglobin of 10 g/dL and HbS <30% via exchange transfusion, or “simple transfusion” defined as targeting a hemoglobin of 10 g/dL irrespective of HbS percentage. The authors did not describe the process for leukoreduction or antigen matching in this study. Both simple and aggressive transfusion were equally effective with regard to SCD-related complications, infection-related serious complications, and postoperative serious complications. Of note, 10% of patients in both arms developed ACS postoperatively, which reinforces the risks of life-threatening complications postoperatively in this population. The study found no significant differences in the aggressive versus simple transfusion groups, although they did find a higher risk of developing a new red cell alloantibody in the aggressive transfusion arm. A minority of patients enrolled in the study received no transfusion, or nonrandomized transfusion and their complications were not reported. Therefore, the study did not provide data on the comparison of complications between patients who were transfused versus not transfused. An interesting finding in this study was that underlying pulmonary disease (unspecified) was a risk factor for postoperative sickle cell-related events,21 which supports the Vichinksy trial finding that a history of pulmonary disease was a predictive factor for postoperative ACS.20
Another multicenter randomized prospective study 2012 in the United Kingdom, Ireland, the Netherlands, and Canada investigated the difference in outcomes between patients undergoing low- and medium-risk procedures. Patients were randomized to no preoperative or preoperative transfusion. In this trial, preoperative transfusion was done within 10 days of the surgery, via simple transfusion for patients with a hemoglobin <9 g/dL to achieve a hemoglobin >10 g/dL or via partial exchange in patients with a hemoglobin >9 g/dL to achieve a HbS% <60%. The study was ultimately terminated early due to increased severe adverse effects in the no preoperative transfusion group, which included mostly episodes of ACS. The study was limited by enrolling a relatively healthy sickle cell population and by several errors in the randomization process.22 However, compared to the previous studies discussed, this study did utilize prestorage leukoreduced red blood cells that were fully matched for ABO, full Rhesus (Cc/D/Ee), K1, and any other antigens against which the patient had known antibodies.
Several Cochrane reviews have been done dating back to 2001, with the most recent update being published in 2020.23 The review included 3 trials, including the Vichinksy 1995 trial, the Howard et al trial, and a third randomized control trial (RCT), comparing no preoperative transfusion to simple or partial exchange transfusion.24 The majority of the patients enrolled in the trials were children, had HbSS genotypes, and were undergoing either low- or medium-risk procedures. When comparing simple to aggressive transfusion (Vichinsky trial), both arms were found to be equally effective, with the only difference in risk being that of developing a new antibody in the aggressive arm (relative risk [RR], 3.05; 95% confidence interval [CI], 1.14–8.20). However, it is important to again note that patients in this trial did not receive phenotype-matched red blood cells, as is now standard practice25 to prevent alloimmunization.
The other 2 trials (Howard and Al-Jaouni) compared preoperative transfusion to no transfusion. With the exception of ACS, there were no differences in SCD-related serious complications for either group. In the Howard et al trial, there were more incidences of ACS in the no preoperative transfusion arm, resulting in premature termination of the trial. Regarding perioperative complications, there was no difference in intraoperative blood loss, surgery-related complications, or respiratory events. However, the Al-Jaouni trial did report an increased risk of surgery delay (RR, 43.32; 95% CI, 6.04–311.00) in the transfusion group. They also reported an increased risk in the development of circulatory overload in the transfusion group (meta-analysis not done given not reported in the Howard trial). There were no other transfusion-related complication or length-of-stay differences. The Howard trial did report a higher mean quality of life when controlling for baseline in the transfusion arm, and significantly fewer incidences of intraoperative and postoperative transfusions (27.5% difference between groups; P < .007).
One systematic review of RCTs and observational studies investigating the risks and benefits of different preoperative transfusion studies was published in 2014. The analysis included 17 studies, 10 of which (3 randomized trials and 7 observational studies) were included in the meta-analysis. Low-risk surgeries included eye, nose, and ears, dental, and distal extremity procedures. Moderate risk involved orthopedic, genitourinary system, and intra-abdominal areas. High-risk surgeries involved the intracranial, cardiovascular, and intrathoracic systems. Unfortunately, all of the RCTs included in this review were underpowered to detect the main clinical outcomes. However, the review did find that exchange transfusion compared to simple transfusion was associated with higher use of transfused blood and higher incidence of transfusion reactions, without benefit in perioperative mortality or postoperative transfusion need. Additionally, preoperative transfusion of any kind was not associated with protection from SCD-related adverse outcomes.19
The American Society of Hematology (ASH) released updated guidelines in 2020 regarding perioperative transfusion support in patients with SCD.25 The guidelines were based on a systematic review of 14 studies (including the Howard, Al-Jaouni, and Vichinksy RCTs, 7 comparative observational studies, and 4 noncomparative observational studies). They again noted an absence of high-quality evidence for the benefits of preoperative transfusion over no preoperative transfusion. The guideline panel did note that there was low-quality evidence from 1 RCT that preoperative transfusion reduced the risk for postoperative transfusion ACS. Because of the association of increased morbidity and mortality associated with ACS, and the risks of transfusion (mainly alloimmunization with aggressive transfusion) being deemed small, the panel concluded that the large desire to prevent postoperative ACS favors the use of preoperative transfusion in the SCD population.25
Summary of the BenefitsWhile the current data on preoperative transfusions in patients with SCD are limited and mixed, the results suggest that in some populations, preoperative transfusion may decrease the risk of the development of postoperative ACS and of other SCD-related complications in low- to medium-risk surgeries. The ASH guideline panel judged that the prevention of postoperative ACS had a large desirable effect. Preoperative transfusions may also increase the quality of life compared to baseline quality of life based on the EuroQol-5D (EQ-5D), which could potentially be due to transfusions decreasing fatigue and pain and, therefore, promoting ability to conduct daily activities of life. Additionally, preoperative transfusions were associated with fewer incidences of intraoperative and postoperative transfusions.
Summary of the RisksTransfusions undoubtedly carry an increased risk of developing new antibodies (alloimmunization) and/or causing an acute or delayed transfusion reaction. Alloimmunization is a significant complication in patients with SCD given the associated delayed hemolytic transfusion reactions (DHTRs), which if associated with hyperhemolysis when patients not only destroy the newly transfused red cells but also their own, can be a life-threatening complication that is difficult to treat.25 Patients with SCD are thought to be at increased risk of alloimmunization due to the differences in frequency of antigen distribution in the donor pool versus recipient pool, and this risk increases as the number of lifetime transfusions increases.26 Preoperative transfusion may also delay surgery given the need for antigen phenotype matching, which can be difficult if the patient has a history of alloimmunization. None of the aforementioned studies found significant differences in transfusion-related serious complications. The ASH guideline panel ultimately judged the potential harms of preoperative transfusions to be small in comparison to the benefits of preventing postoperative ACS.
When to Consider Preoperative TransfusionCurrently, ASH does suggest transfusion over no preoperative transfusion in all patients with SCD undergoing surgery requiring general anesthesia and lasting >1 hour, which is a conditional recommendation based on very low certainty data.25 The guidelines note that decision should be individualized based on genotype, risk of surgery, baseline hemoglobin, prior transfusion-related complications, and disease severity.
We, therefore, recommend exercising caution in patients with underlying SCD-related complications, especially underlying pulmonary disease or prior transfusion-related complications, given the increased risk of volume overload in this population. Preoperative transfusion needs should be made in consultation with a hematologist familiar with the management of people with SCD. At our institutions, we approach each patient individually, taking into account their SCD genotype, risk level of surgery, baseline total hemoglobin, complications with prior transfusion, known blood antigens, and SCD disease severity. All patients receive leukoreduced, nonsickle trait blood as is recommended by ASH. Additionally, patients receive ABO and Rh-antigen matched blood. Patients with known antibodies should receive extending matching based on phenotype, which includes matching beyond ABO and Rh-antigens, such as Jka/Jkb, Fya/Fyb, and S/s antigens. Additionally, whenever possible, we recommend prophylactic extended phenotypic matching for patients without known antibodies if available, as is suggested by ASH for patients with SCD of all genotypes.25 However, in emergency settings, it is reasonable to give O¯ blood, regardless of shelf-life and sickle trait status, if necessary.
 Figure 2.:
Figure 2.: Preoperative transfusion management. In addition to the above transfusion parameters, we additionally recommend that all patients receive leukoreduced, nonsickle trait blood. All patients should also receive ABO and Rh-antigen-matched blood, and patients with known antibodies should receive extended matching based on their phenotype.
When transfusing preoperatively, we recommend simple transfusion if Hb <8.5 g/dL for patients with all SCD genotypes, with a posttransfusion hemoglobin goal no >11 g/dL to avoid the risk of hyperviscosity (Figure 2). We recommend exchange transfusion if total hemoglobin ≥8.5 g/dL, with a posttransfusion goal of 10 to 11 g/dL. We do not target a specific HbS% at our institutions for patients with HbSS (or HbS/β0-thalassemia) disease; however, we recommend a target HbA of 70% for patients with HbSC or HbS/β +-thalassemia disease.
OTHER PERIOPERATIVE CONSIDERATIONS History of Venous Thromboembolic DiseaseThromboembolic disease is common, yet an underdiagnosed complication in patients with SCD. This was supported by the finding that there is less utilization of computed tomography (CT) in patients with SCD compared to non-SCD patients,28 and by one study’s finding of incidental pulmonary thrombus on CT in 17% of patients with ACS.29
One large retrospective review found a prevalence of VTE of 50% in patients with SCD who were hospitalized (compared to 33% of patients without SCD).30 Notably, the prevalence of deep vein thrombosis (DVT) was the same in patients with and without SCD, suggesting that patients with SCD may have more rates of pulmonary thrombus in situ rather than true pulmonary embolus. Autopsy studies quote a similar prevalence of 50%.28
Table. - Management of Specific Anticoagulants in Patients With SCD and History of VTE Undergoing a Surgical Procedure Agent Preoperative Postoperative Heparin Pause/hold day of procedure (at least 8 h before start). Resume 12–24 h after procedure, or 4–6 h in high-risk patientsa. Direct factor Xa inhibitors If CrCl >50 mL/min, hold dose 1 d before procedure for low-bleeding risk and 2 d prior for high-bleeding risk proceduresb. If CrCl > 50 mL/min, resume 1 d post- and 2 d postprocedure for low- and high-risk procedures, respectivelyb. Oral direct thrombin inhibitors Same as DOAC management, except those with renal dysfunction (CrCl <30) hold dose an additional 1 day prior. Same as DOAC management, except those with renal dysfunction (CrCl <30) resume dose an additional 2 days postprocedure. Warfarin Hold dose 5 d before procedurec. Consider bridging with heparin in high-risk patientsa. Resume 12–24 h after procedure.aHigh-risk thrombotic patients = patients with VTE within last 3 mo and/or patients with severe thrombotic burden.
bSee DOAC-specific guidelines if CrCl <50 mL/min.
cWith the exception of certain cardiovascular procedures such as endovascular stenting, ablations, and/or implantable device placement.33,34Patients with SCD and VTE on chronic anticoagulation regimens are managed per the same guidelines as patients without SCD, taking into account renal clearance, provoked versus unprovoked status, and risk/benefit ratio of chronic anticoagulation. In the perioperative setting, home anticoagulation and bridging should be managed per specific agent (Table).31,32
Risk of VTE From the ProcedureCertain procedures are associated with higher risk of VTE disease, including invasive neurosurgery, orthopedic (especially total hip arthroplasty), major vascular surgery, colectomies, and radical cystectomies.27,33 For patients who are not already anticoagulated due to a history of VTE, we recommend prophylactic VTE prophylaxis in all SCD patients hospitalized presurgery and postsurgery.
Autologous Cell SalvageThere is currently no strong evidence investigating the use of autologous cell salvage therapy in patients with SCD. There are a few case reports with varying degrees of success using cell salvage. In 1 case report of a pediatric patient with HbSS undergoing scoliosis surgery, the patient successfully received prestored autologous units that had been collected 2 weeks before surgery, as well as salvaged blood collected intraoperatively.34 Another case report described a patient with SCD and a history of multiple red blood cell antibodies who presented at 30 weeks gestation with hemolysis, elevated liver enzyme, and low platelets (HELLP) syndrome.35 The patient then developed ACS and was taken for urgent cesarean delivery. Due to lack of available compatible red blood cell units, blood lost during the surgery was collected for cell salvage. Despite warming, acidosis-minimizing techniques, and heparinization, the collected blood clotted and was unable to be retransfused. The authors hypothesized that the patient’s red blood cells had sickled and hemolyzed. There are currently no national or societal guidelines on the use of cell salvage therapy in this population, and ASH has identified the risk-benefit ratio of its use as a priority research question.25 We, therefore, do not recommend the use of this therapy in this population given limited data and potential risks.
DISCUSSIONIn summary, perioperative planning is critical to reduce risks of surgery in patients with SCD. Preoperatively, careful consideration with regard to timing of surgery, rate and type of IV fluid, and operating room temperature can help decrease the need for prolonged NPO times, risk of underhydration or overhydration with IV fluids, and potential risks of VOE precipitation or volume overload (Figure 3). Patients with SCD and VTE are managed the same as the general population with regard to holding anticoagulation before the procedure, and prompt resumption of anticoagulation (or VTE prophylaxis for those without current VTE disease) is important given the increased risk of postprocedural VTE risk in this population. Intraoperatively, general knowledge of the anesthetic plan and its associated risks aid in planning for possible postprocedure complications, such as hypotension or rebound pain.
 Figure 3.: Sickle cell disease-specific perioperative checklist. Adapted from the work by Sanders et al.27
Figure 3.: Sickle cell disease-specific perioperative checklist. Adapted from the work by Sanders et al.27Preoperative transfusion is recommended for all patients with SCD who are undergoing surgery that either requires general anesthesia or any moderate anesthesia lasting >1 hour. This evidence-based recommendation is aimed mainly at reducing the high-mortality postprocedure risk of ACS. Preoperative transfusion should be done on an individualized basis, taking into account the patient’s SCD genotype and disease severity, history of antibodies and/or transfusion reactions, risk of surgery, and baseline hemoglobin levels. Extra time may need to be allotted for potential extended phenotyping matching in those patients with a history of alloimmunization, and the associated time it takes to receive matched RBC units for those patients. Preoperative transfusion planning should always be done in conjunction with the patient’s primary hematologist to assist with determining whether the patient would benefit from simple or partial exchange transfusion and what hemoglobin level to target posttransfusion.
DISCLOSURESName: Roberta C. G. Azbell, MD.
Contribution: This author wrote the initial manuscript and reviewed the final manuscript.
Conflicts of Interest: None.
Name: Sophie M. Lanzkron, MD, MHS.
Contribution: This author provided edits and reviewed the final manuscript.
Conflicts of Interest: Bluebird Bio: Consultancy, CSL Behring: Research Funding, GBT: Research Funding, Imara: Research Funding, Novartis: Research Funding, Novo Nordisk: Consultancy, Pfizer: Current holder of individual stocks in a privately held company, Shire: Research Funding, Teva: Current holder of individual stocks in a privately held company.
Name: Payal C. Desai, MD.
Contribution: This author provided edits and reviewed the final manuscript.
Conflicts of Interest: Consultant for GBT for grant review; advisory board for Forma; funding from the National Institutes of Health, University of Tennessee, and University of Pittsburgh; and speaker for Novartis.
This manuscript was handled by: Susan Goobie, MD, FRCPC.
REFERENCES 1. Sundd P, Gladwin MT, Novelli EM. Annual review of pathology: mechanisms of disease pathophysiology of sickle cell disease. Rev Adv first. 2019;14:263–292. 2. Kanter J, Kruse-Jarres R. Management of sickle cell disease from childhood through adulthood. Blood Rev. 2013;27:279–287. 3. Stanley AC, Christian JM. Sickle cell disease and perioperative considerations: review and retrospective report. J Oral Maxillofac Surg. 2013;71:1027–1033. 4. Khurmi N, Gorlin A, Misra L. Perioperative considerations for patients with sickle cell disease: a narrative review. Can J Anesth. 2017;64:860–869. 5. Paschal RD. Perioperative management in sickle cell disease. South Med J. 2016;109:557–559. 6. Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med. 2010;152:26–35. 7. Vaid S, Bell T, Grim R, Ahuja V. Predicting risk of death in general surgery patients on the basis of preoperative variables using American College of Surgeons National Surgical Quality Improvement Program data. Perm J. 2012;16:10–17. 8. Cazenave M, Audard V, Bertocchio JP, et al. Tubular acidification defect in adults with sickle cell disease. Clin J Am Soc Nephrol. 2020;15:16–24. 9. Nath KA, Hebbel RP. Sickle cell disease: renal manifestations and mechanisms. doi:10.1038/nrneph.2015.8 10. Okomo U, Meremikwu MM. Fluid replacement therapy for acute episodes of pain in people with sickle cell disease. Cochrane Database Syst Rev. 2017;2017. 10.1002/14651858.CD005406.pub5. 11. Carden MA, Fay M, Sakurai Y, et al. Normal saline is associated with increased sickle red cell stiffness and prolonged transit times in a microfluidic model of the capillary system. Microcirculation. 2017;24. doi:10.1111/micc.12353. 12. Carden MA, David BC, Ahmad FA, et al. Normal saline bolus use in pediatric emergency departments is associated with poorer pain control in children with sickle cell anemia and vaso-occlusive pain. Am J Hematol. 2019;22:689–696. 13. Semler MW, Self WH, Wanderer JP, et al.; SMART Investigators and the Pragmatic Critical Care Research Group. Balanced crystalloids versus saline in critically ill adults. N Engl J Med. 2018;378:829–839. 14. Brandow AM, Stucky CL, Hillery CA, Hoffmann RG, Panepinto JA. Patients with sickle cell disease have increased sensitivity to cold and heat. Am J Hematol. 2013;88:37–43. 15. Fields JM, Piela NE, Au AK, Ku BS. Risk factors associated with difficult venous access in adult ED patients. Am J Emerg Med. 2014;32:1179–1182. 16. Woods GM, Sharma R, Creary S, et al. Venous thromboembolism in children with sickle cell disease: a retrospective cohort study. 2018. doi:10.1016/j.jpeds.2018.01.073 17. Koshy M, Weiner SJ, Miller ST, et al. Surgery and anesthesia in sickle cell disease. Blood. 1995;86:3676–3684. 18. Adjepong KO, Otegbeye F, Adjepong YA. Perioperative management of sickle cell disease. Mediterr J Hematol Infect Dis. 2018;10:e2018032. 19. Alotaibi GS, Alsaleh K, Bolster L, Mcmurtry MS, Wu C, Alotaibi S. Preoperative transfusion in patients with sickle cell disease to prevent perioperative complications: a systematic review and meta-analysis transfusion in patients with sickle cell disease to prevent perioperative complications: a systematic review and me. Hematology. 2014;19:463–471. 20. Vichinsky EP, Haberkern CM, Neumayr L, et al. A comparison of conservative and aggressive transfusion regimens in the perioperative management of sickle cell disease. N Engl J Med. 1995;333:206–213. 21. Waldron P, Pegelow C, Neumayr L, et al. Tonsillectomy, adenoidectomy, and myringotomy in sickle cell disease: perioperative morbidity. J Pediatr Hematol Oncol. 1999;21. 22. Howard J, Malfroy M, Llewelyn C, et al. The transfusion alternatives preoperatively in sickle cell disease (TAPS) study: a randomised, controlled, multicentre clinical trial. Lancet. 2013;381:930–938. 23. Estcourt LJ, Kimber C, Trivella M, Doree C, Hopewell S. Preoperative blood transfusions for sickle cell disease. Cochrane Database Syst Rev. 2020;2020. doi:10.1002/14651858.CD003149.pub4. 24. Al-Jaouni SK, Al-Muhayawi SM, Qari MH, Nawas MA, Al-Mazrooa A. Randomized clinical trial to evaluate the safety of avoiding pre-operative transfusion in sickle cell anemia. Bahrain Med Bull. 2006;28:164–167. 25. Chou ST, Alsawas M, Fasano RM, et al. American Society of Hematology 2020 Guidelines for sickle cell disease: transfusion support. Blood Adv. 2020;4:327–355. 26. Ballas SK, Kesen MR, Goldberg MF, et al. Beyond the definitions of the phenotypic complications of sickle cell disease: an update on management. Sci World J. 2012;2012:55. 27. White RH, Zhou H, Romano PS. Incidence of symptomatic venous thromboembolism after different elective or urgent surgical procedures. Thromb Haemost. 2003;90:446–455. 28. Novelli EM, Huynh C, Gladwin MT, Moore CG, Ragni MV. Pulmonary embolism in sickle cell disease: a case-control study. J Thromb Haemost. 2012;10:760–766. 29. Dessap AM, Deux JF, Abidi N, et al. Pulmonary artery thrombosis during acute chest syndrome in sickle cell disease. Am J Respir Crit Care Med. 2011;184:1022–1029. 30. Stein PD, Beemath A, Meyers FA, Skaf E, Olson RE. Deep venous thrombosis and pulmonary embolism in hospitalized patients with sickle cell disease. Am J Med. 2006;119:897.e7–897.e11. 31. Spyropoulos AC, Douketis JD. How I treat anticoagulated patients undergoing an elective procedure or surgery. Blood. 2012;120:2954–2962. 32. Shaw JR, Li N, Vanassche T, et al. Predictors of preprocedural direct oral anticoagulant levels in patients having an elective surgery or procedure. Blood Adv. 2020;4:3520–3527. 33. Gangireddy C, Rectenwald JR, Upchurch GR, et al. Risk factors and clinical impact of postoperative symptomatic venous thromboembolism. J Vasc Surg. 2007;45:335–342.e1. 34. Fox JS, Amaranath L, Hoeltge GA, Andrish JT. Autologous blood transfusion and intraoperative cell salvage in a patient with homozygous sickle cell disease. Accessed April 28, 2022. www.ccjm.org. 35. Schott NJ, Yazer MH, Krohner R, Waters JH. Failure of intraoperative red cell salvage: a patient with sickle cell disease and HELLP (hemolysis, elevated liver enzymes and low platelets) syndrome. J Extra Corpor Technol. 2014;46:314–316.
留言 (0)